Page 1 of 11
CM2.1-2 | CM2.1-2 | Socio-cultural Assessment of Family and Community — SDL Guide
Learning Objectives
- Describe the steps in performing a clinico-socio-cultural and demographic assessment of an individual, family, and community
- Identify and explain the socio-cultural factors and family types that influence health and disease
- Demonstrate correct assessment of socio-economic status (SES) using validated Indian scales in a simulated environment
INSTRUCTIONS
A patient's health cannot be separated from where they live, what they earn, or who their family is. This module teaches you how to perform a systematic socio-cultural and socio-economic assessment — skills that every doctor practising in India needs to deliver equitable, contextualised care.
References
- Park K. Park's Textbook of Preventive and Social Medicine, 26th ed. Bhanot Publishers, 2023. Chapters: Social Determinants of Health; Family Health; Socio-economic Assessment (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Raju is a 6-year-old boy brought to your rural health centre with recurrent diarrhoea. His weight is far below the third centile. His mother is illiterate, the family of seven lives in a two-room mud house with no piped water, and his father works as a daily-wage labourer. The child's illness is only the surface of a much deeper story — one written in poverty, crowding, and cultural practices about food and hygiene. Before you can help Raju, you need to read that story accurately. This module teaches you exactly how to do that.
WHY THIS MATTERS
Social and cultural factors are the single largest determinants of population health — far more powerful than individual-level medical care for explaining why some communities suffer more disease than others. As a future doctor in India, you will encounter patients across vast gradients of education, income, caste, and custom. A prescription alone cannot address malnutrition rooted in poverty or infectious disease amplified by overcrowded housing. Competencies CM2.1 and CM2.2 equip you to gather the information that makes a real difference: understanding a family's structure and the forces shaping their lives so that you can offer care that is realistic, relevant, and effective.
RECALL
From your Introduction to Community Medicine, recall that health is a state of complete physical, mental, and social well-being (WHO, 1948) — not merely the absence of disease. You also learned that the community is the unit of study in social medicine and that determinants of health operate at multiple levels: individual biology, behaviour, family environment, community norms, and broader socioeconomic structures. Keep these concepts active as you work through this module, because the assessment tools you will learn here are designed to measure those very determinants systematically.
Social Determinants and Their Health Impact
Health inequities across Indian communities are not random — they follow predictable social patterns. The social determinants of health are the conditions in which people are born, grow, live, work, and age, shaped by the distribution of money, power, and resources at the global, national, and local levels. The World Health Organization's Commission on Social Determinants of Health (2008) documented that these structural factors explain the majority of variation in life expectancy, child mortality, and nutritional status between and within countries. In India, a child born in a poor rural household has a starkly different health trajectory than one born in an urban upper-income family — not primarily because of genetic differences, but because of differential access to nutrition, clean water, education, and healthcare.
The commission's framework distinguishes structural determinants (governance, macroeconomic policies, social norms including caste and gender, education systems) from intermediary determinants (living conditions, occupation and income, food security, access to health services, social support networks). Structural factors set the stage; intermediary factors translate that stage into day-to-day health or disease. For a practising physician, recognising this two-tier causation is essential: a patient with recurrent tuberculosis who lives in a crowded slum and is malnourished cannot be adequately managed without addressing those underlying realities.
In the Indian context, key structural determinants include literacy (especially female literacy, strongly associated with child survival), caste and social exclusion, rural-urban disparity, and access to social welfare programmes. Intermediary determinants include housing type, water and sanitation quality, occupation-related exposures, household food security, and social isolation in the elderly. Every community-level health programme — from immunisation coverage to anaemia reduction — shows better outcomes in socially advantaged groups, a phenomenon known as the social gradient in health.
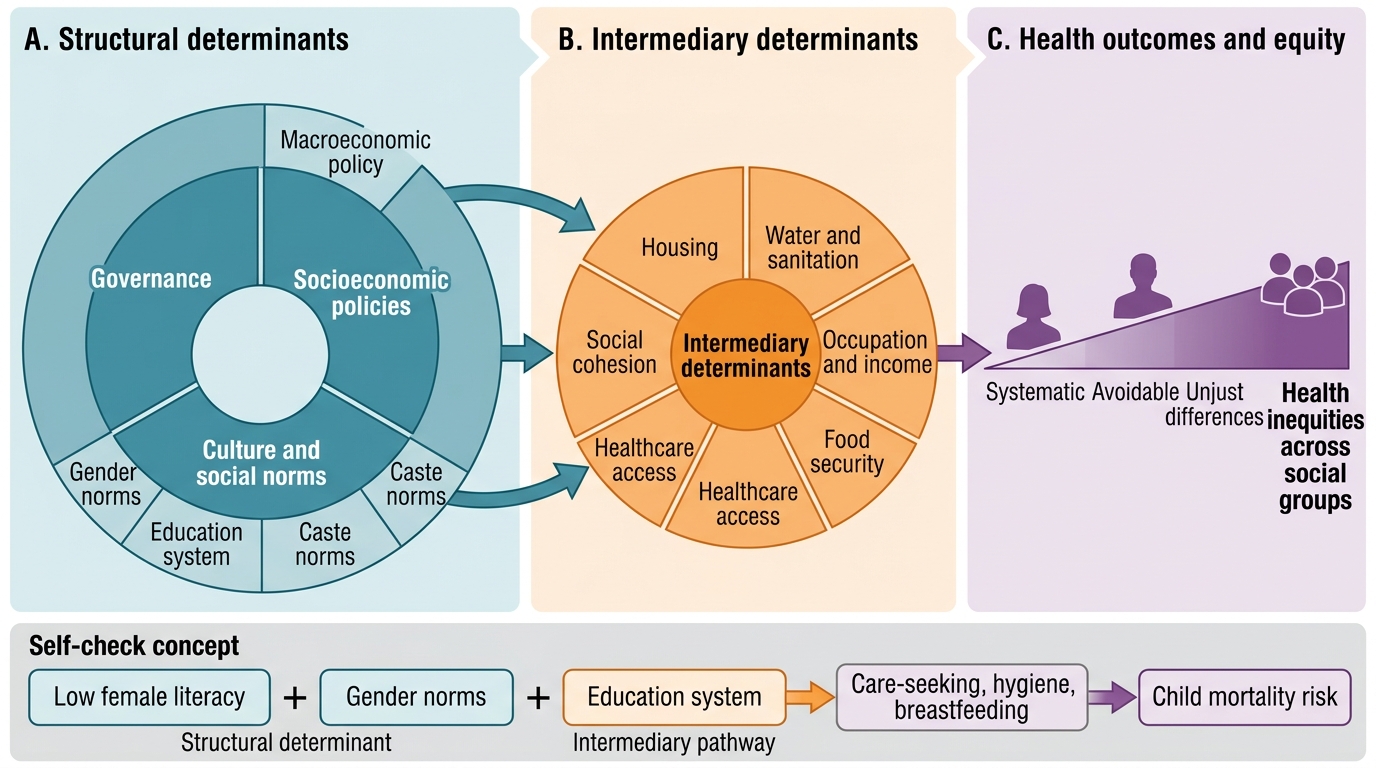
WHO Social Determinants of Health Framework
- Structural determinants: governance, macroeconomic policy, social norms (caste, gender), education
- Intermediary determinants: housing, water/sanitation, occupation/income, food security, healthcare access, social cohesion
- Outcome gradient: systematic, avoidable, and unjust differences in health across social groups
SELF-CHECK
Which component of the WHO social determinants framework most directly explains why girls in a community with low female literacy have higher child-mortality rates?
A. Intermediary determinant — poor water and sanitation
B. Structural determinant — education system and gender norms
C. Intermediary determinant — inadequate access to health services
D. Structural determinant — macroeconomic policy on healthcare spending
Reveal Answer
Answer: B. Structural determinant — education system and gender norms
Female literacy is a structural determinant — shaped by the education system and social norms about gender — that sets the conditions for later intermediary determinants (how a mother seeks and accesses care, hygiene practices, breastfeeding rates). It belongs in the structural tier, not the intermediary tier, even though its effect is mediated through daily-life factors.
Family Types and Socio-cultural Factors
The family is the fundamental social unit in India and the primary environment in which health behaviours, food practices, hygiene habits, and health-seeking decisions are formed. To assess a patient's health comprehensively, a doctor must understand the family's structure, composition, and the cultural values operating within it. The family types described in community medicine are defined by the relationships between household members and the sharing of resources.
A nuclear family consists of a married couple and their unmarried children. This is the simplest and increasingly common urban structure, offering fewer sources of social support but also fewer conflicts about decision-making. A joint family comprises two or more married couples — typically the patriarch and his sons with their families — who share a common dwelling, kitchen, and income. Joint families remain common in rural India and can be protective (multiple earners, childcare sharing, elder care) but also propagate transmitted cultural norms and restrict women's autonomy in healthcare decisions. An extended family includes the nuclear or joint family plus collateral relatives (uncles, aunts, cousins, or grandparents in a separate unit but close by). A three-generation family shares a single roof across three generations — grandparents, parents, and children — and is conceptually distinct from the joint family in that it does not require multiple married siblings.
Beyond structure, a family's role in health is shaped by its socio-cultural factors: the community's dominant religion and the food taboos, fasting norms, and birth and death rituals it prescribes; the caste-group and its occupational traditions and social exclusions; the education level of the head of household and of women (the latter most strongly predicting child nutrition and immunisation uptake); occupation and associated exposures (agricultural chemicals, construction dust, child labour); and social customs such as consanguineous marriages, which increase the risk of autosomal recessive disorders in South Indian communities.
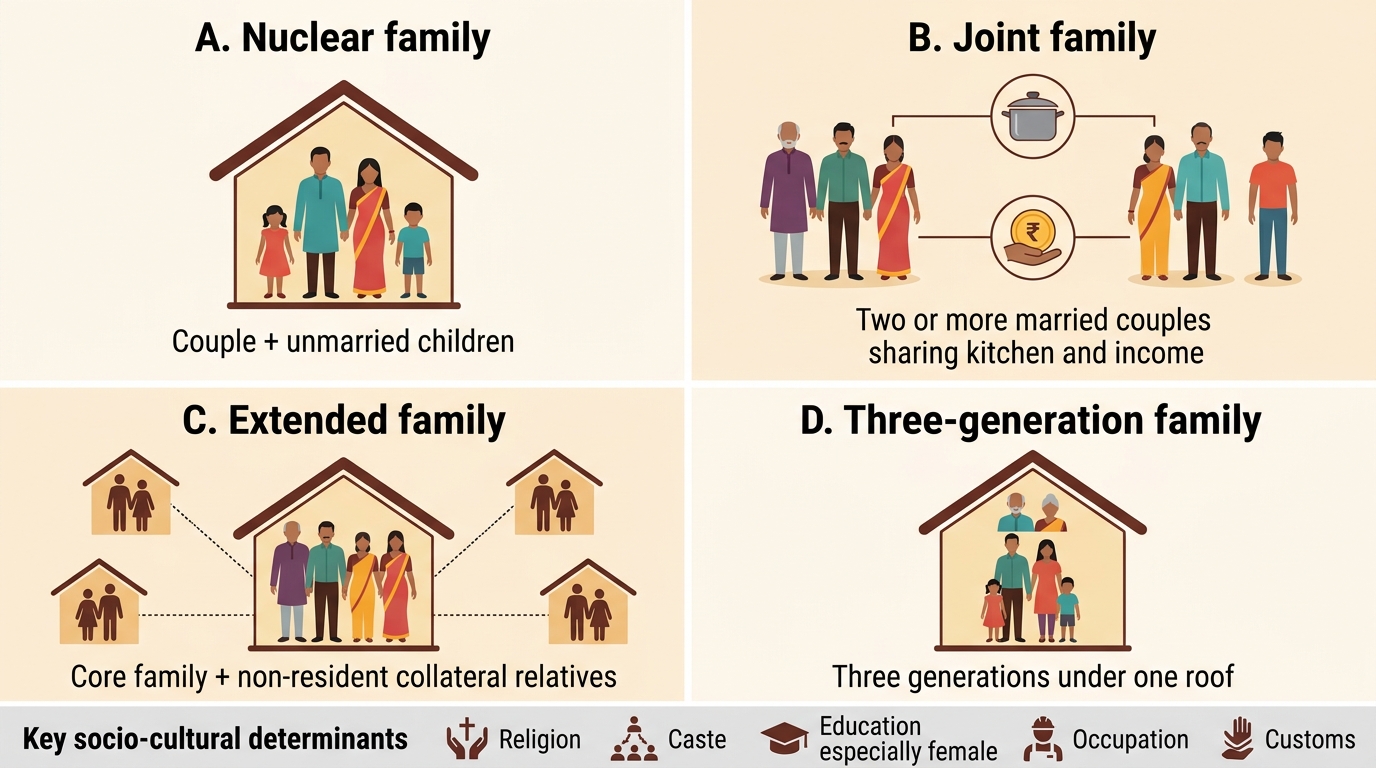
Indian Family Types in Community Medicine
- Nuclear: couple + unmarried children
- Joint: two+ married couples (brothers/parents-in-law) sharing kitchen + income
- Extended: nuclear/joint + non-resident collateral relatives
- Three-generation: three generations under one roof
- Key socio-cultural determinants: religion, caste, education (especially female), occupation, customs
SELF-CHECK
A field visit reveals a household in which the grandfather (retired government official), his son and daughter-in-law, their two children, and the son's younger brother (unmarried) all live together under one roof and pool income. Which family type best describes this household?
A. Nuclear family
B. Extended family
C. Joint family
D. Three-generation family
Reveal Answer
Answer: C. Joint family
This is a joint family — two married-sibling generations plus an unmarried member sharing residence and pooled income. Three-generation simply requires three generations on one roof without specifying multiple married couples; the defining feature of a joint family is two or more married couples (or a parental couple and a married child) sharing a common household and resources.
Assessment Methods: SES Scales and Clinico-social Tools
A systematic clinico-socio-cultural assessment integrates clinical findings with information about the patient's social circumstances. The assessment proceeds through five broad steps: (1) identify the presenting complaint and clinical findings; (2) obtain a detailed social history (family composition, housing type, water and sanitation, income sources, education levels, occupation, caste/religion, cultural practices); (3) classify socio-economic status (SES) using a validated scale; (4) identify specific socio-cultural risk factors relevant to the complaint; and (5) formulate a management plan that accounts for the social context.
For SES classification, Indian community medicine uses three validated scales, each designed for a different setting. Modified Kuppuswamy scale (designed for urban populations) evaluates three domains: education of the head of household (scores 1–7, from illiterate to graduate and above), occupation (scores 1–10, from unemployed to professional), and per-capita monthly income of the family (scores 1–12, updated periodically with the Consumer Price Index for Industrial Workers, CPI-IW). Total score ranges from 3 to 29 and is classified into five classes: Class I (Upper, 26–29), Class II (Upper-Middle, 16–25), Class III (Lower-Middle, 11–15), Class IV (Upper-Lower, 5–10), Class V (Lower, 3–4). Because income values are CPI-linked, the cut-off income values for each score must be updated to the current year — the percentage weight remains constant but the absolute rupee amounts change.
The B.G. Prasad classification uses per-capita monthly income alone, divided into five classes (Class I to V). Like Kuppuswamy's income component, its rupee cut-offs are regularly updated with the CPI-IW. It is simpler to use in rapid surveys but captures less information than the Kuppuswamy scale. The Pareek scale is designed for rural populations and encompasses a broader set of variables: education of head, occupation, social participation, land ownership, housing type, farm power, material possessions, and self-sufficiency in food. Each variable is scored; the total score classifies the family into upper, middle, or lower SES. Its multidimensional nature makes it more sensitive to the diverse rural Indian context.
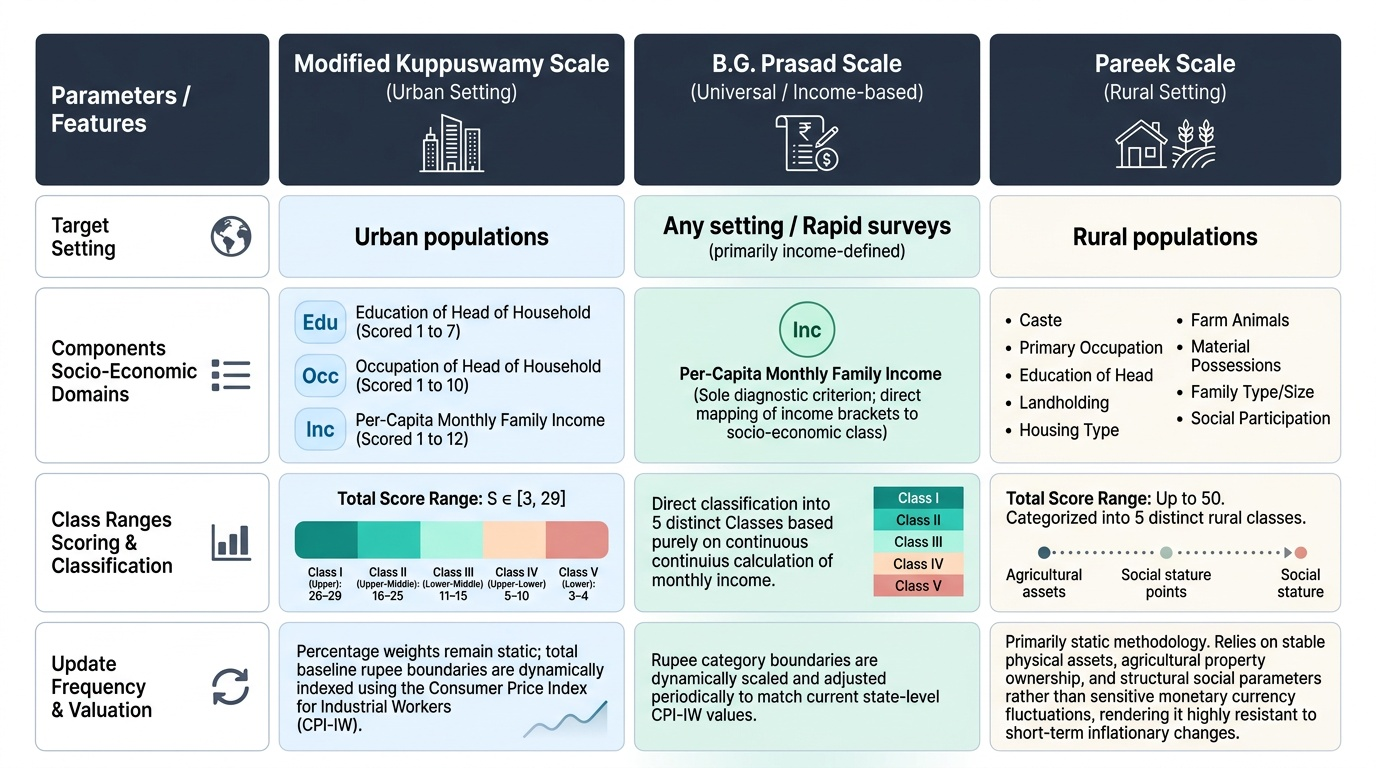
Provided image
| Scale | Setting | Domains | Classes | Update mechanism |
|---|---|---|---|---|
| Modified Kuppuswamy | Urban | Education + Occupation + Income | I–V (score 3–29) | CPI-IW (income component) |
| B.G. Prasad | Urban/general | Income (per-capita/month) | I–V | CPI-IW |
| Pareek | Rural | Education, occupation, land, housing, social participation, material possessions | Upper/Middle/Lower | No standard CPI-link; revised by committee |
SELF-CHECK
A doctor in an urban clinic wants to classify the SES of a family. The head of household is a graduate employed as a supervisor (occupation score 7) with a per-capita income placing it in the fourth income bracket. Education score is 6. Which scale and what approximate class would apply?
A. Pareek scale, Middle class
B. Modified Kuppuswamy scale, Class I (Upper)
C. Modified Kuppuswamy scale, Class II (Upper-Middle)
D. B.G. Prasad scale, Class II
Reveal Answer
Answer: C. Modified Kuppuswamy scale, Class II (Upper-Middle)
Urban setting → Modified Kuppuswamy. Education 6 + Occupation 7 + Income bracket 4 (approximately 4) = total approximately 17, which falls in Class II (Upper-Middle: 16–25). The B.G. Prasad scale and Pareek scale are either income-only or rural; neither applies here for the three-domain scoring the question implies.