Page 5 of 11
CM2.3-5 | CM2.3-5 | Health Seeking Behaviour and Community Relationships — SDL Guide (Part 2)
Poverty, Social Security Measures, and Their Relationship to Health
Poverty is not merely a background characteristic — it is an active and potent driver of disease. The relationship between poverty and ill-health is bidirectional and self-reinforcing: poverty increases exposure to environmental hazards (unsafe water, overcrowding, malnutrition), reduces the ability to use preventive and curative services, and impairs physical and cognitive development; illness in turn reduces earning capacity and productivity, pushing families further into poverty. This cycle — known as the poverty-disease spiral — is especially vicious when it affects children, because early-life health deprivation compounds across a lifetime.
In India, poverty measurement has evolved through successive expert committee recommendations. The Tendulkar Committee (2009) defined the poverty line as per-capita daily consumption expenditure of Rs 27 (rural) and Rs 33 (urban) at 2004–05 prices. This line was widely criticised as too low to capture actual deprivation. The Rangarajan Committee (2014) revised it upward to Rs 32 (rural) and Rs 47 (urban) at 2011–12 prices, which translated to a substantially higher proportion of the population classified as poor. Neither poverty line represents the threshold for adequate nutrition and health — both are minimum-subsistence benchmarks. The Below Poverty Line (BPL) card system uses these estimates to identify households eligible for subsidised services, though targeting errors (exclusion of genuinely poor households and inclusion of non-poor) remain significant.
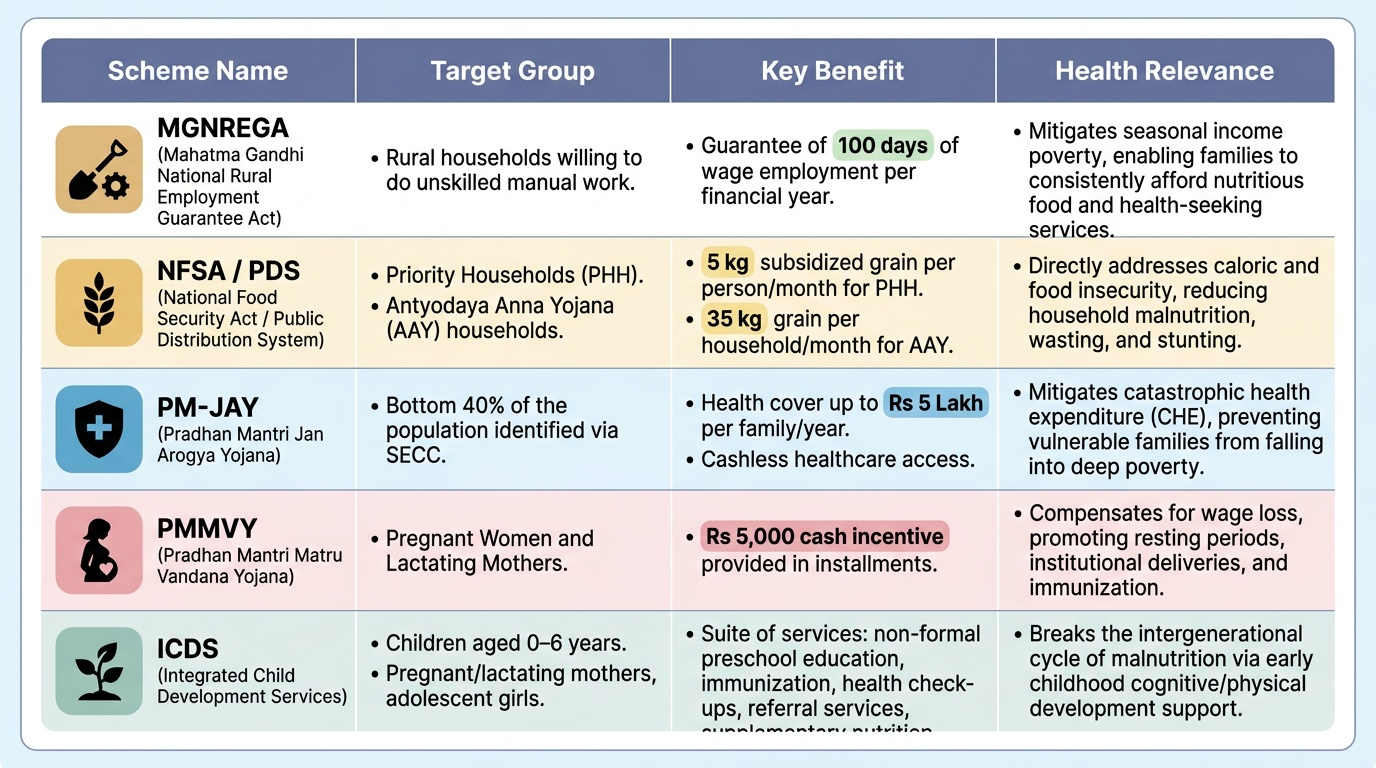
India's social security architecture is designed to buffer the most vulnerable against the health consequences of poverty, though coverage and implementation are uneven. Key schemes with direct health relevance include:
- MGNREGA (Mahatma Gandhi National Rural Employment Guarantee Act, 2005): guarantees 100 days of wage employment per household per year in rural areas; addresses income poverty and enables health spending.
- National Food Security Act (NFSA), 2013 / Public Distribution System (PDS): priority households receive 5 kg of subsidised foodgrain (rice/wheat/coarse grain) per person per month; Antyodaya Anna Yojana households receive 35 kg per household per month at nominal prices — directly addresses food insecurity, a root cause of malnutrition.
- PM-JAY (Pradhan Mantri Jan Arogya Yojana / Ayushman Bharat): provides cashless health insurance of Rs 5 lakh per family per year for secondary and tertiary hospitalisation, targeting approximately 50 crore beneficiaries from the bottom 40% of the population. This is the largest enabling-barrier intervention in Indian health care.
- ICDS (Integrated Child Development Services): through anganwadi centres, delivers supplementary nutrition, immunisation, preschool education, and referral services to children under-6 and pregnant/lactating women — directly addresses child undernutrition and maternal health.
- PMMVY (Pradhan Mantri Matru Vandana Yojana): cash transfer of Rs 5,000 to first-time pregnant women for antenatal care, institutional delivery, and postnatal care — addresses economic enabling barriers for maternal health.
Provided image
| Scheme | Target group | Key benefit | Health relevance |
|---|---|---|---|
| MGNREGA | Rural poor | 100 days wage employment/household/year | Income for health expenditure |
| NFSA/PDS | Priority households (BPL) | 5 kg/person/month subsidised grain; Antyodaya: 35 kg/household/month | Food security → reduces malnutrition |
| PM-JAY | Bottom 40% (~50 crore) | Rs 5 lakh/family/year hospitalisation cover | Removes economic enabling barrier |
| ICDS | Children <6, pregnant/lactating women | Nutrition, immunisation, preschool, referral | Child nutrition + maternal health |
| PMMVY | First-time pregnant women | Rs 5,000 cash transfer | Antenatal care, institutional delivery |
SELF-CHECK
A pregnant woman from a Below Poverty Line household is reluctant to deliver at a government hospital because her family cannot afford the costs of travel and the loss of a day's income for the accompanying relative. Which social security scheme most directly addresses this enabling barrier?
A. MGNREGA — provides 100 days of wage employment
B. NFSA — provides subsidised foodgrain to priority households
C. PMMVY — provides Rs 5,000 cash transfer to first-time pregnant women for antenatal and delivery care
D. ICDS — provides supplementary nutrition through anganwadi centres
Reveal Answer
Answer: C. PMMVY — provides Rs 5,000 cash transfer to first-time pregnant women for antenatal and delivery care
PMMVY directly addresses the economic enabling barrier for maternal health by providing a cash transfer to the pregnant woman, which can offset travel and opportunity costs for institutional delivery. MGNREGA is a general income-support scheme, not targeted at maternal health enabling costs. NFSA addresses food security. ICDS addresses child nutrition and antenatal supplementary nutrition — useful but not the direct cash transfer for delivery-related costs.
Assessing Barriers to Health Seeking in a Simulated Environment
Assessment of barriers to health seeking is a structured clinical skill — not an informal conversation. The goal is to systematically identify which barrier categories (predisposing, enabling, need-based) are operating for a specific patient or family, so that the management plan can target those barriers precisely. In a simulated environment (and later, in field and clinical settings), you should follow a structured probing interview approach.
The interview begins with open-ended questions that invite the patient to describe their experience without leading them toward expected answers: 'Can you tell me what happened from when you first noticed this problem until today?' 'Was there anything that made it difficult to come earlier?' 'Who in your family helped you decide to come here?' These questions surface the patient's own account before the interviewer imposes a framework. The interviewer then follows up with probing questions that systematically cover the Andersen model domains: economic access ('How did you manage the cost of coming here today?'), geographic access ('How long did it take to travel here?'), social permission ('Did anyone in your family advise you on whether to seek care?'), and cultural belief ('Have you tried any other treatment first? What do you think caused this problem?').
For community-level assessment, barrier patterns are identified through surveys, focus group discussions (FGDs), and key informant interviews (KIIs) with community members, healthcare workers (ASHAs, ANMs), and community leaders. Quantitative surveys establish prevalence of each barrier; qualitative methods (FGDs, KIIs) explain the social processes underlying the numbers. Together they provide a community health diagnosis that is actionable — identifying the 2–3 dominant barriers that, if addressed, would most improve utilisation.
Documentation in clinical practice should record: presenting barrier categories, their perceived severity by the patient, social support available, and which schemes or services the patient is or should be enrolled in. This structured record enables targeted referral and follow-up.
- Open-ended questions first: 'What happened from when you first noticed this until today?'
- Probe systematically: economic access, geographic, social permission, cultural beliefs
- Community-level: surveys (quantitative) + FGDs + KIIs (qualitative) for barrier diagnosis
- Document: barrier categories, social support, scheme eligibility, referral plan
Applying Social Assessment: From Individual to Community Action
The integration of health-seeking behaviour assessment, community psychology, and poverty analysis comes together in a coherent action framework that operates simultaneously at individual, family, community, and health system levels. A practitioner who has completed this assessment can move from diagnosis to intervention at all four levels.
At the individual/family level, the action is personalised: identify the dominant barriers, address enabling barriers with scheme linkages (PM-JAY enrolment, PMMVY registration, ICDS anganwadi referral), address cultural barriers with accurate and respectful health education that names the specific belief and provides evidence-based counter-information, and mobilise family and community social capital (recruiting a trusted family member as a health ally). For Meena, the breast cancer patient from the hook scenario, a structured barrier assessment would have identified: economic barrier (transport cost) → JSSK or PM-JAY referral; social-permission barrier (husband's anticipated reaction) → involve the husband in a counselling session that explains the medical situation; informational barrier (not knowing about free care) → register her with the local ASHA and VHSNC; cultural belief (neighbour's reassurance that the lump was harmless) → clear correction with clinical facts.
At the community level, the action is population-based: present aggregate barrier data to the VHSNC, identify the two or three modifiable barriers that account for the largest share of under-utilisation, and design targeted behaviour-change communication (BCC) that addresses the specific social norms and beliefs operating in that community. Community-level action often requires engaging informal leaders (religious figures, teachers, traditional healers) because they are trusted information sources and norm-setters. A campaign that only uses government health workers to counter vaccine hesitancy spread through a religious leader will be outgunned — a campaign that recruits the religious leader as a champion will succeed.
At the health system level, barrier data inform facility planning (adding outreach camps in under-served areas), staff training (cultural competence, reducing discrimination), and scheme implementation (PM-JAY enrolment drives at community level). The feedback loop from community barrier assessment to health system redesign is the formal function of the District Health Action Plan process.
- Individual: scheme linkages + targeted counselling + family mobilisation
- Community: VHSNC presentation + BCC targeting identified norms + informal leader engagement
- Health system: outreach planning + cultural competence training + scheme enrolment drives
- Feedback loop: barrier assessment → District Health Action Plan → system redesign
CLINICAL PEARL
When assessing a patient's delay in seeking care, resist the clinical reflex to attribute it to a single cause. Real delays are almost always multi-barrier: a patient who says 'I could not afford it' was also influenced by a family member who minimised the symptom, a culturally sanctioned first step to consult a traditional healer, and an enabling factor of the government hospital being 12 km away with no bus service. The Andersen model's power is that it forces you to check all three domains — predisposing, enabling, need — before concluding you understand the barrier. Addressing only the economic barrier while leaving the social-permission or geographic barrier unaddressed will not change utilisation.