Page 1 of 11
DR5.1 | Scabies Treatment Planning — SDL Guide
Learning Objectives
- Recognise the characteristic morphology and distribution of scabies that signal the diagnosis and trigger treatment.
- Explain the Sarcoptes scabiei life cycle and the hypersensitivity basis of itch as the rationale for scabicide choice and treatment timing.
- Devise a complete, evidence-based treatment plan for scabies, selecting the correct scabicide for each patient group.
- State the adverse drug reactions and cautions of permethrin, ivermectin, benzyl benzoate and sulphur.
- Plan simultaneous treatment of all close contacts and environmental measures, and identify crusted (Norwegian) scabies as a distinct, highly contagious entity.
INSTRUCTIONS
Scabies is one of the commonest reasons a patient presents to an Indian dermatology or general clinic with intractable itch, and it is one of the most frequently mismanaged. The reason is rarely the choice of drug — permethrin and ivermectin are cheap and widely available — but the failure to treat the whole household, to give clear application instructions, and to warn the patient that itch persists for weeks after the mite is dead. This module builds the treatment plan competency (DR5.1) from morphology through to a household management plan, with explicit attention to the adverse drug reactions the competency demands.
References
- Khanna N. Illustrated Synopsis of Dermatology and Sexually Transmitted Diseases, 6th ed. Ch: Infestations — Scabies (textbook)
- Sacchidanand S, et al. IADVL Textbook of Dermatology, 4th ed. Section: Parasitic Infestations (textbook)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
A 9-year-old boy is brought to the clinic with two weeks of relentless night-time itching. His mother, his younger sister and his grandmother — all sharing one bedroom — have started scratching too. On examination there are tiny serpiginous grey lines between his fingers and excoriated papules on his wrists and around his waist. His genitals carry a few intensely itchy nodules. The previous prescriber gave a steroid cream, which made him worse. This is textbook scabies, and the clue that should clinch it is not just the rash but the family clustering and the nocturnal itch. The treatment is simple, cheap and curative — provided you treat the whole family at once and tell them what to expect.
WHY THIS MATTERS
Scabies is a public-health-scale problem you will meet constantly — in paediatric wards, in crowded hostels, in old-age homes and in any household living in close contact. Getting the treatment plan right matters because the commonest cause of 'treatment failure' is not drug resistance but an incomplete plan: the index patient is treated while asymptomatic but infested contacts re-infest them, or the patient stops the scabicide too early, or panics when the itch persists for three more weeks and demands stronger steroids. As the clinician who devises the plan, you control whether this family is cured in one cycle or churns through months of misery — and whether you recognise the immunocompromised patient whose crusted scabies can seed an entire ward.
RECALL
Before building the treatment plan, recall three things from your earlier years. From anatomy, the epidermis is layered (stratum corneum, granulosum, spinosum, basale) — the scabies mite burrows only within the dead, keratinised stratum corneum, which is why topical scabicides applied to intact skin can reach it. From physiology and immunology, delayed (type IV) hypersensitivity to mite antigen, faeces and eggs is what produces the itch — this explains the 4-6 week delay before symptoms in a first infestation and the persistence of itch after the mite is killed. From pharmacology, ivermectin acts on glutamate-gated chloride channels found only in invertebrate nerve and muscle, paralysing the mite while sparing human cells, and pyrethroids such as permethrin disrupt invertebrate sodium channels.
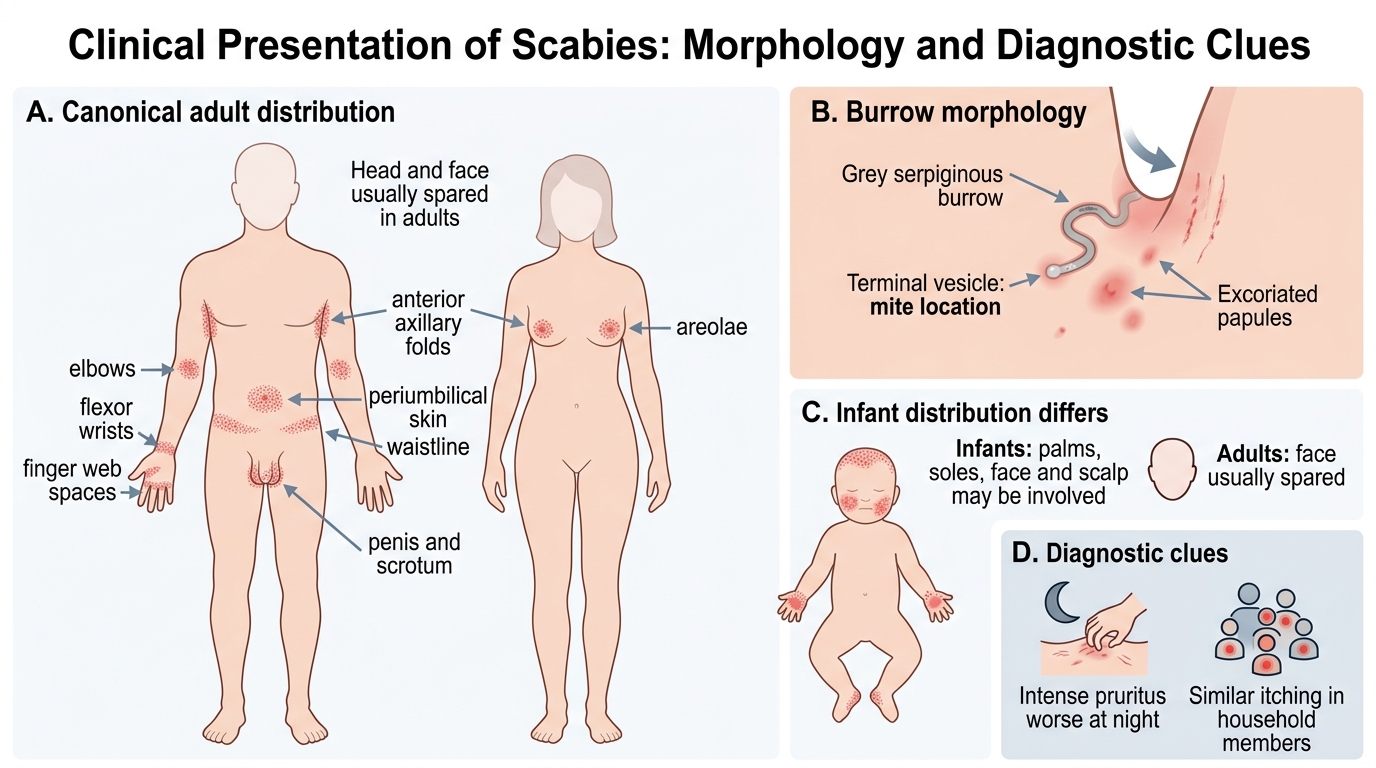
Clinical Presentation of Scabies: Morphology and Diagnostic Clues
Scabies: Distribution, Burrows, and Diagnostic Clues
The diagnosis of scabies rests on recognising a characteristic distribution of intensely pruritic lesions rather than any single lesion type. The pathognomonic primary lesion is the burrow — a short, grey, serpiginous or S-shaped line a few millimetres long, often ending in a tiny vesicle where the female mite sits — but burrows are frequently obscured by scratching, so much of the diagnosis comes from the company the lesions keep. Scabies has a strong predilection for the finger web spaces, the flexor aspects of the wrists, the elbows, the anterior axillary folds, the periumbilical skin and the waistline, and in men the penis and scrotum, where firm itchy nodules are highly suggestive. In women the areolae are involved, and in infants the palms, soles, face and scalp — areas spared in adults — may be affected. Critically, the itch is worse at night and there is usually a history of similar symptoms in other household members, the two clues that separate scabies from eczema or insect bites.
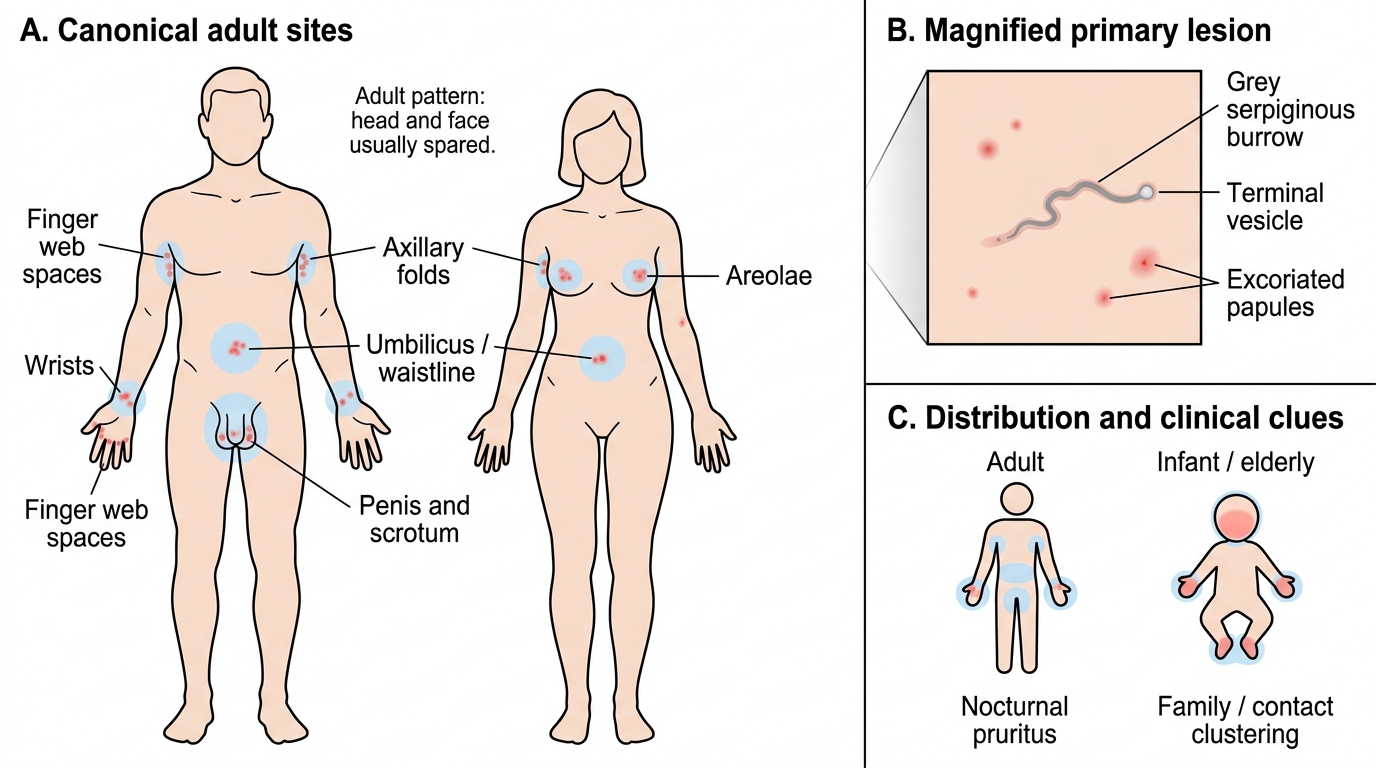
Scabies: Canonical Sites and Burrow Morphology
- Primary lesion: burrow (grey serpiginous line, few mm, may end in vesicle)
- Secondary lesions: excoriated papules, nodules (penis/scrotum), eczematisation, impetiginisation
- Adult distribution: web spaces, wrists, axillae, waist, genitalia, areolae — head/face spared
- Infant/elderly distribution: palms, soles, face, scalp may be involved
- Cardinal clues: nocturnal pruritus + family/contact clustering
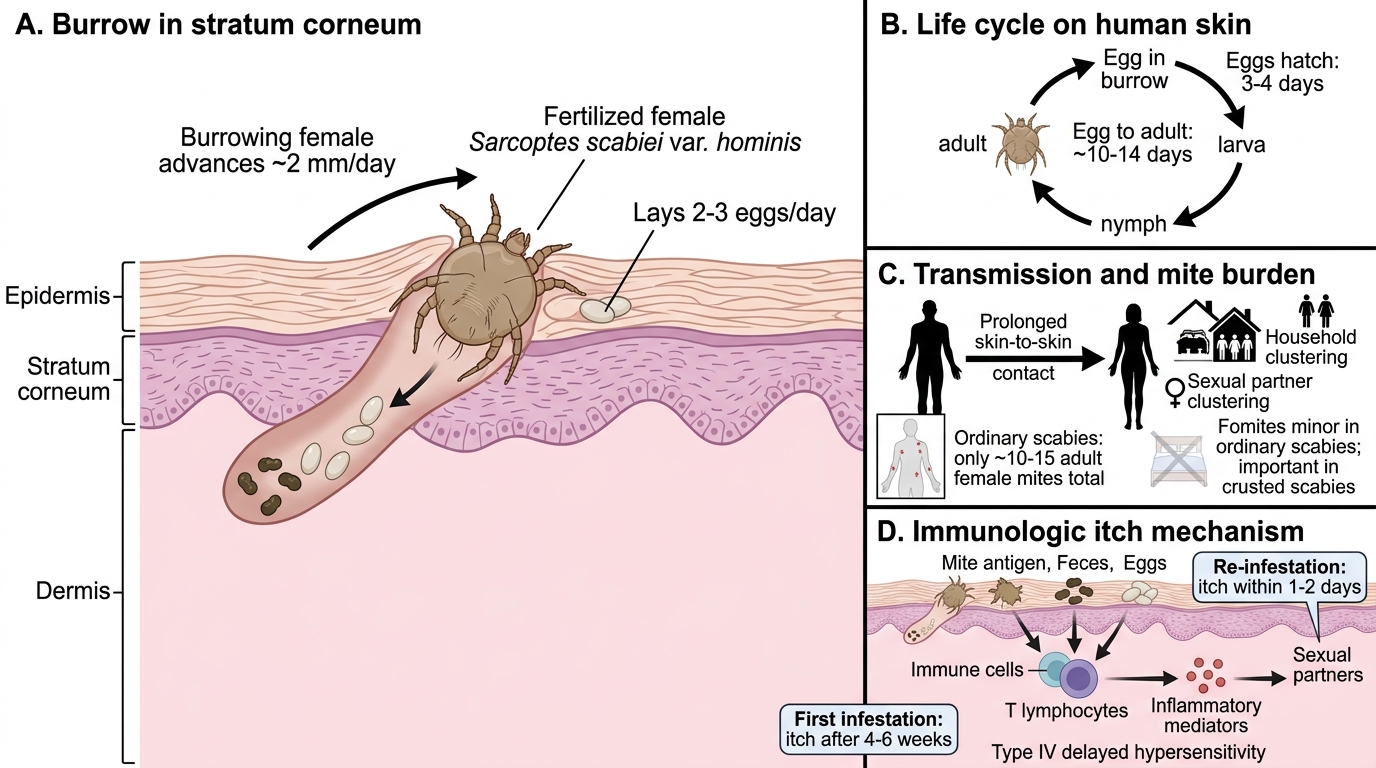
Pathogenesis of Scabies: Sarcoptes scabiei Life Cycle and Itch Mechanism
Pathogenesis of Scabies: Life Cycle and Itch Mechanism
Scabies is caused by Sarcoptes scabiei var. hominis, an eight-legged mite (an arachnid, not an insect) that completes its entire life cycle on human skin. The fertilised female burrows into the stratum corneum at roughly 2 mm per day, laying two to three eggs daily as she advances; the eggs hatch into larvae in three to four days, mature through nymphal stages into adults in about ten to fourteen days, and the cycle repeats. In ordinary (non-crusted) scabies the total mite burden is small — typically only 10 to 15 adult female mites on the whole body — which is why the disease is intensely itchy yet the mites are hard to find. Transmission is by prolonged skin-to-skin contact, which is why it clusters in households and among sexual partners; fomite transmission via shared bedding and clothing is minor in ordinary scabies but becomes important in the crusted form. The dominant symptom, itch, is a type IV (delayed) hypersensitivity response to mite proteins, faeces and eggs, so in a first infestation symptoms appear only after a 4-6 week sensitisation period, whereas re-infestation provokes itch within one to two days.
- Organism: Sarcoptes scabiei var. hominis (8-legged mite, arachnid)
- Burrowing female lays 2-3 eggs/day; egg→adult in ~10-14 days
- Ordinary scabies burden: ~10-15 female mites total
- Transmission: prolonged skin-to-skin (household, sexual); fomites minor (major in crusted)
- Itch = type IV hypersensitivity → 4-6 wk delay first time, 1-2 days on re-infestation
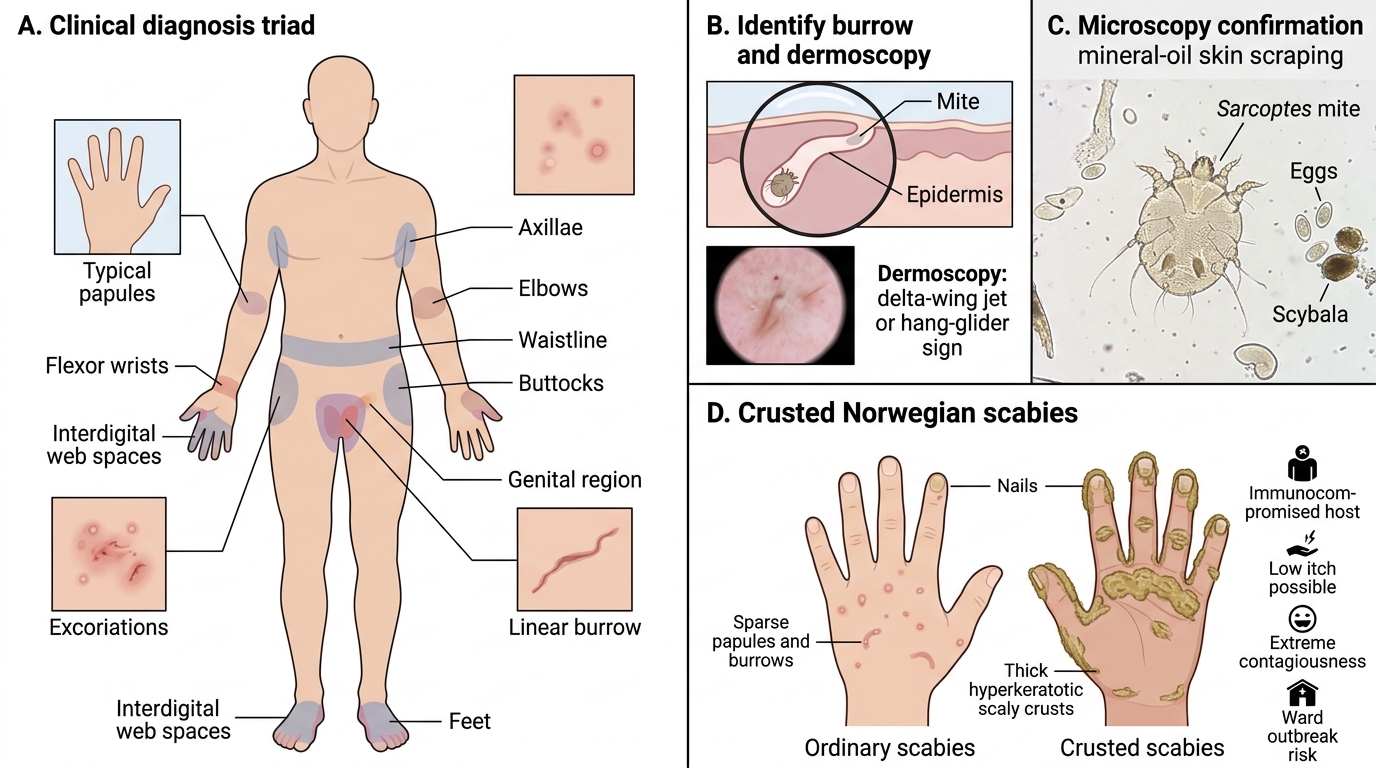
Clinical Features and Diagnosis
Clinical Features and Diagnosis of Scabies
Diagnosis is usually clinical, made on the triad of characteristic morphology, characteristic distribution and a supportive epidemiological history of itchy contacts. The single most useful confirmatory step at the bedside is to identify a burrow and demonstrate the mite, eggs or faecal pellets (scybala) from it — dermoscopy reveals the classic 'delta-wing jet' or 'hang-glider' sign (the dark triangular head of the mite at the end of the burrow), and light microscopy of a skin scraping taken from a fresh burrow in mineral oil can show the mite or eggs. It is essential to recognise crusted (Norwegian) scabies as a separate clinical entity: occurring in the immunocompromised (HIV, lymphoma, long-term steroids, severe learning disability, the very elderly), it presents as thick, hyperkeratotic, scaly crusts — often on the hands, feet, scalp and under the nails — that teem with thousands to millions of mites. Crusted scabies may itch little or not at all, is extraordinarily contagious, and is a frequent source of institutional and ward outbreaks, so it demands isolation and aggressive combined treatment.
- Diagnosis is clinical: morphology + distribution + contact history
- Confirmation: visualise burrow; dermoscopy 'delta-wing jet' sign; microscopy of scraping (mite/eggs/scybala)
- Crusted (Norwegian) scabies: immunocompromised host; thick hyperkeratotic crusts; thousands–millions of mites
- Crusted form: may itch little, extremely contagious, causes ward/institutional outbreaks → isolate
SELF-CHECK
A 60-year-old man on long-term oral corticosteroids for lymphoma develops thick, scaly, hyperkeratotic crusts on his hands and feet with surprisingly little itch. Two nurses on his ward have since developed itchy rashes. What is the diagnosis and its key implication?
A. Ordinary scabies; treat the patient alone with permethrin
B. Crusted (Norwegian) scabies; he is highly contagious, must be isolated, and needs combined topical permethrin plus oral ivermectin
C. Psoriasis; itch is unusual so scabies is excluded
D. Contact dermatitis from his medication; no infection-control measures needed
Reveal Answer
Answer: B. Crusted (Norwegian) scabies; he is highly contagious, must be isolated, and needs combined topical permethrin plus oral ivermectin
Hyperkeratotic crusts in an immunocompromised host with low itch but high transmissibility (two staff infested) is classic crusted (Norwegian) scabies — a hyperinfestation with thousands to millions of mites. It requires isolation and aggressive combined treatment (topical permethrin plus repeated oral ivermectin, often with a keratolytic), not single-agent therapy.