Page 8 of 20
DR12.4 | Cutaneous Adverse Drug Reaction Recognition — SDL Guide
Learning Objectives
- Distinguish the major cutaneous adverse drug reactions — fixed drug eruption, DRESS, and the SJS/TEN spectrum — from one another and from non-drug skin conditions.
- State the body-surface-area thresholds that separate SJS, SJS-TEN overlap and TEN.
- Recognise fixed drug eruption by its recurrence at the same site on re-exposure.
- Recognise DRESS by its long latency, eosinophilia and internal organ involvement.
- Identify common culprit drugs and the immune mechanisms behind severe cutaneous reactions, and triage by severity.
INSTRUCTIONS
Almost any drug can cause a skin reaction, and most are trivial — but a small group of cutaneous adverse drug reactions are life-threatening, and the doctor who can tell them apart at the bedside saves lives. This module trains you to recognise three reactions you must never miss: fixed drug eruption (benign but characteristic), DRESS (a slow-burning multiorgan reaction), and the Stevens-Johnson syndrome / toxic epidermal necrolysis spectrum (dermatological emergencies graded by body surface area). Recognising which reaction you are looking at, and distinguishing it from non-drug skin conditions, is the focus of competency DR12.4 and the first step before any treatment.
References
- Khanna N. Illustrated Synopsis of Dermatology and Sexually Transmitted Diseases, 6th ed. Ch: Cutaneous Adverse Drug Reactions (textbook)
- Sacchidanand S, et al. IADVL Textbook of Dermatology, 4th ed. Section: Drug Reactions (SJS/TEN, DRESS, Fixed Drug Eruption) (textbook)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
Three patients arrive in a single clinic morning, each with a rash, each having recently taken a drug. The first has a single dark, well-defined patch on his lip that he says appears at the exact same spot every time he takes a painkiller. The second, a young woman three weeks into a new epilepsy drug, has a fever, a swollen face, a widespread rash, and — on her blood count — a high eosinophil count. The third, started on a sulfa drug a week ago, has fever, painful red skin peeling away in sheets, and raw erosions in his mouth and eyes. These are three completely different cutaneous adverse drug reactions — a fixed drug eruption, DRESS, and Stevens-Johnson syndrome / toxic epidermal necrolysis — and only one of them is benign. Telling them apart is the skill this module builds.
WHY THIS MATTERS
Cutaneous adverse drug reactions are among the commonest iatrogenic problems in medicine, and while most are mild, the severe forms — DRESS and the SJS/TEN spectrum — carry significant mortality and are true emergencies. The doctor who recognises a severe reaction early, stops the drug, and escalates care changes the outcome; the one who mistakes early TEN for a simple viral rash loses critical time. Competency DR12.4 asks you specifically to distinguish these reactions from each other and from other skin conditions, because the management of a benign fixed drug eruption (reassure, avoid the drug) is worlds apart from that of TEN (emergency burns-type care). Pattern recognition here is genuinely life-saving clinical medicine.
RECALL
Recall the immune mechanisms you have already met, because they underlie these reactions. Type IV (delayed, T-cell-mediated) hypersensitivity is the dominant mechanism in fixed drug eruption, DRESS and SJS/TEN — which is why these reactions take days to weeks rather than minutes to appear, unlike the immediate type I (IgE-mediated) reactions that cause urticaria and anaphylaxis. Recall too the concept of body surface area (BSA) as a measure of how much skin is involved — the same measure used in burns — because the SJS/TEN spectrum is graded entirely by the percentage of skin that detaches. And recall eosinophils, the white cells whose rise in the blood is a clue to a drug hypersensitivity reaction. These three ideas — delayed T-cell immunity, BSA, and eosinophilia — frame everything that follows.
The Spectrum of Skin Reactions to Drugs
Severity Spectrum of Cutaneous Adverse Drug Reactions
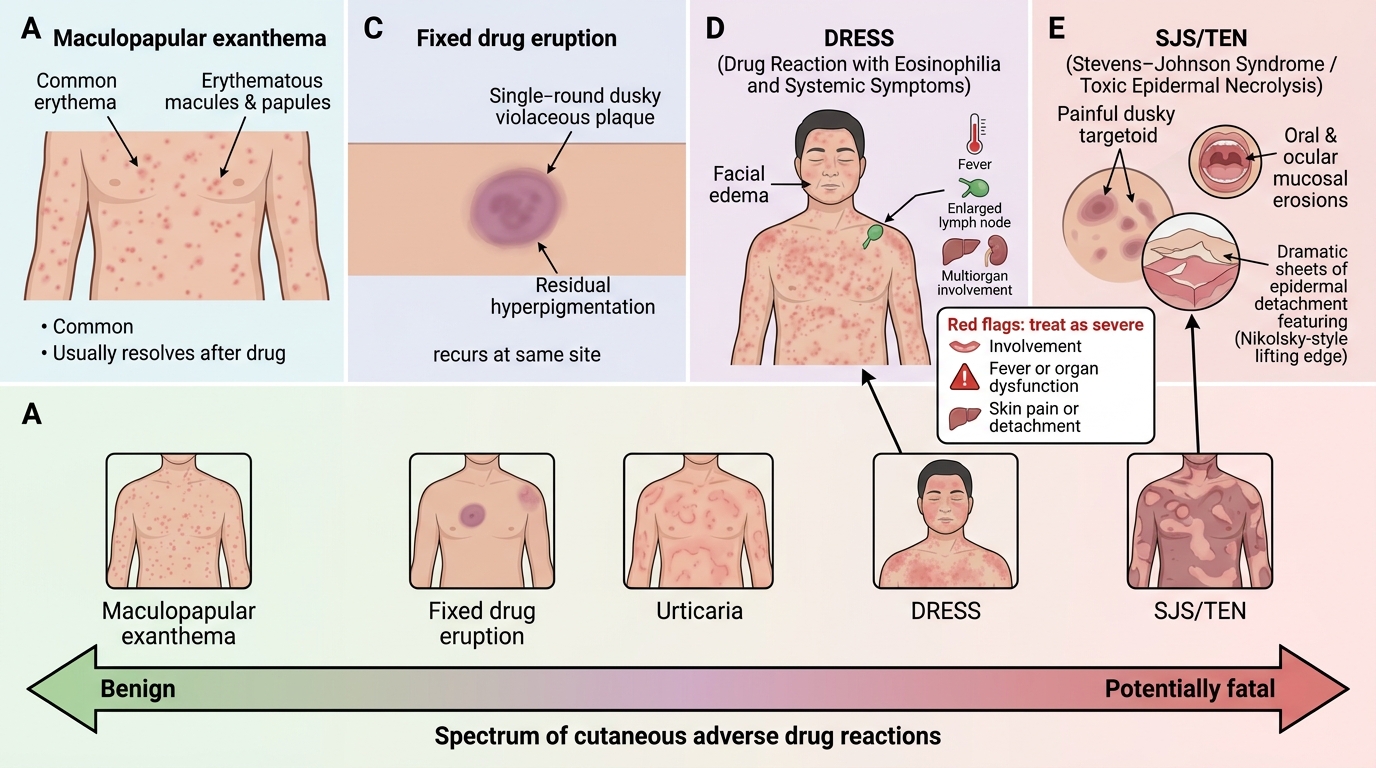
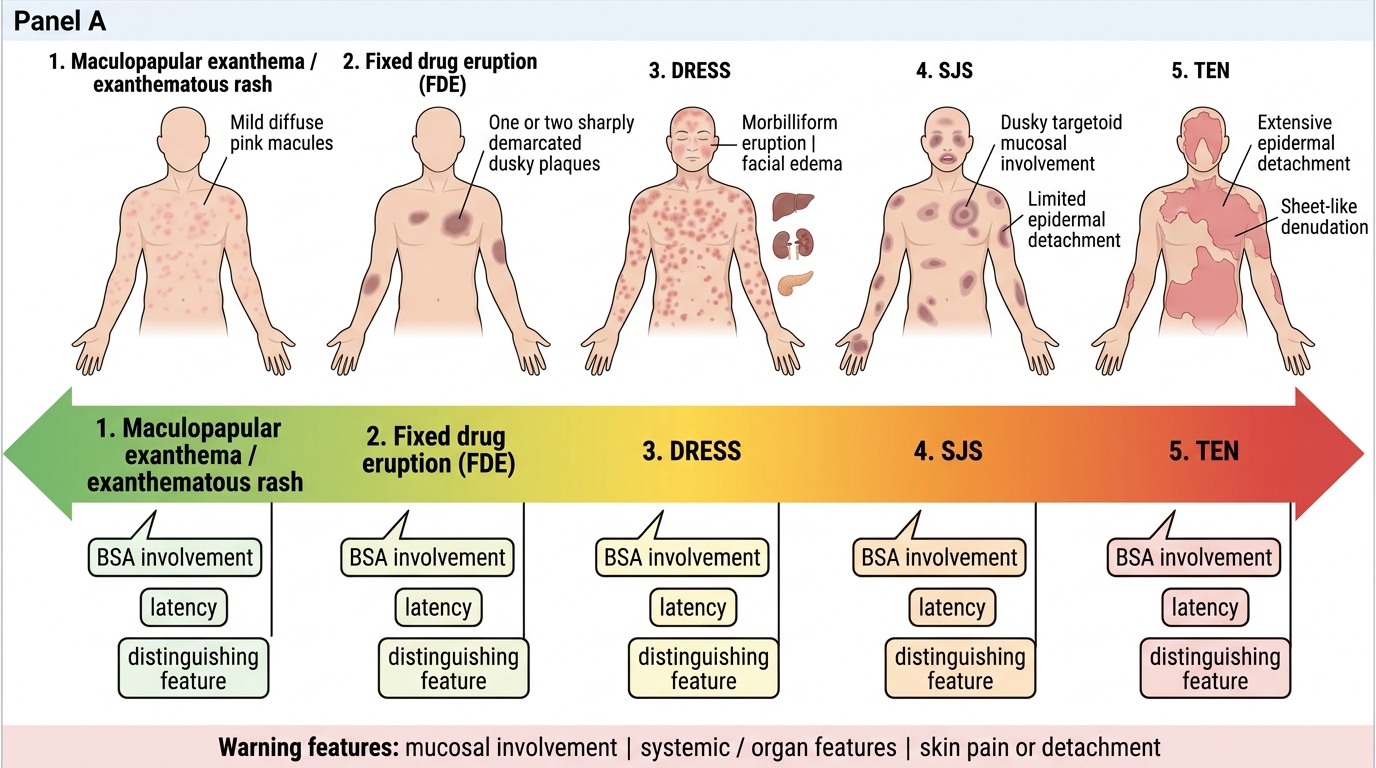
Cutaneous adverse drug reactions form a spectrum from trivial to fatal, and orienting yourself along this spectrum is the first diagnostic act. At the benign end is the maculopapular (exanthematous) rash, a widespread measles-like eruption that is the commonest drug reaction and usually settles when the drug is stopped. In the middle sit the fixed drug eruption — one or a few well-defined plaques that recur at the same site — and urticaria. At the dangerous end lie the severe cutaneous adverse reactions: DRESS (a multiorgan hypersensitivity syndrome), and the Stevens-Johnson syndrome (SJS) to toxic epidermal necrolysis (TEN) spectrum, in which the epidermis dies and detaches. This module concentrates on the three you must never miss: fixed drug eruption, DRESS, and SJS/TEN.
The value of holding the whole spectrum in mind is that it tells you, from the first look, how worried to be. Three features distinguish the severe end from the benign: involvement of mucous membranes (eyes, mouth, genitals), systemic features (fever, organ dysfunction), and skin pain or detachment rather than mere itch. Any rash with these warning features is treated as potentially severe until proven otherwise. Recognising where a reaction sits on this spectrum is what triggers the appropriate urgency.
Severity Spectrum of Cutaneous Adverse Drug Reactions
- Benign: maculopapular/exanthematous rash (commonest); urticaria.
- Intermediate: fixed drug eruption — recurs at the same site.
- Severe (never miss): DRESS; SJS/TEN spectrum.
- Warning features of severe disease: mucosal involvement, systemic/organ features, skin pain or detachment.
Mechanisms Behind Severe Cutaneous Reactions
Mechanisms Behind Severe Cutaneous Drug Reactions
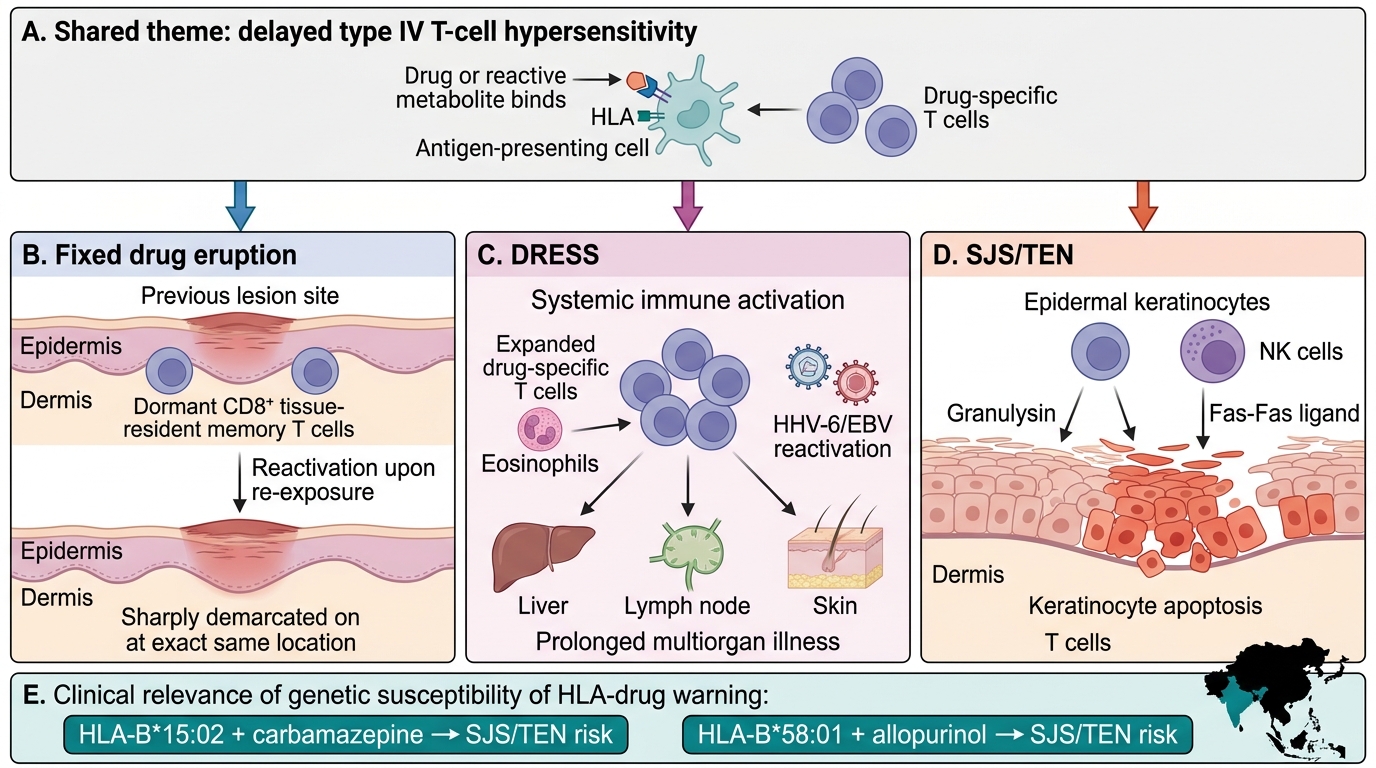
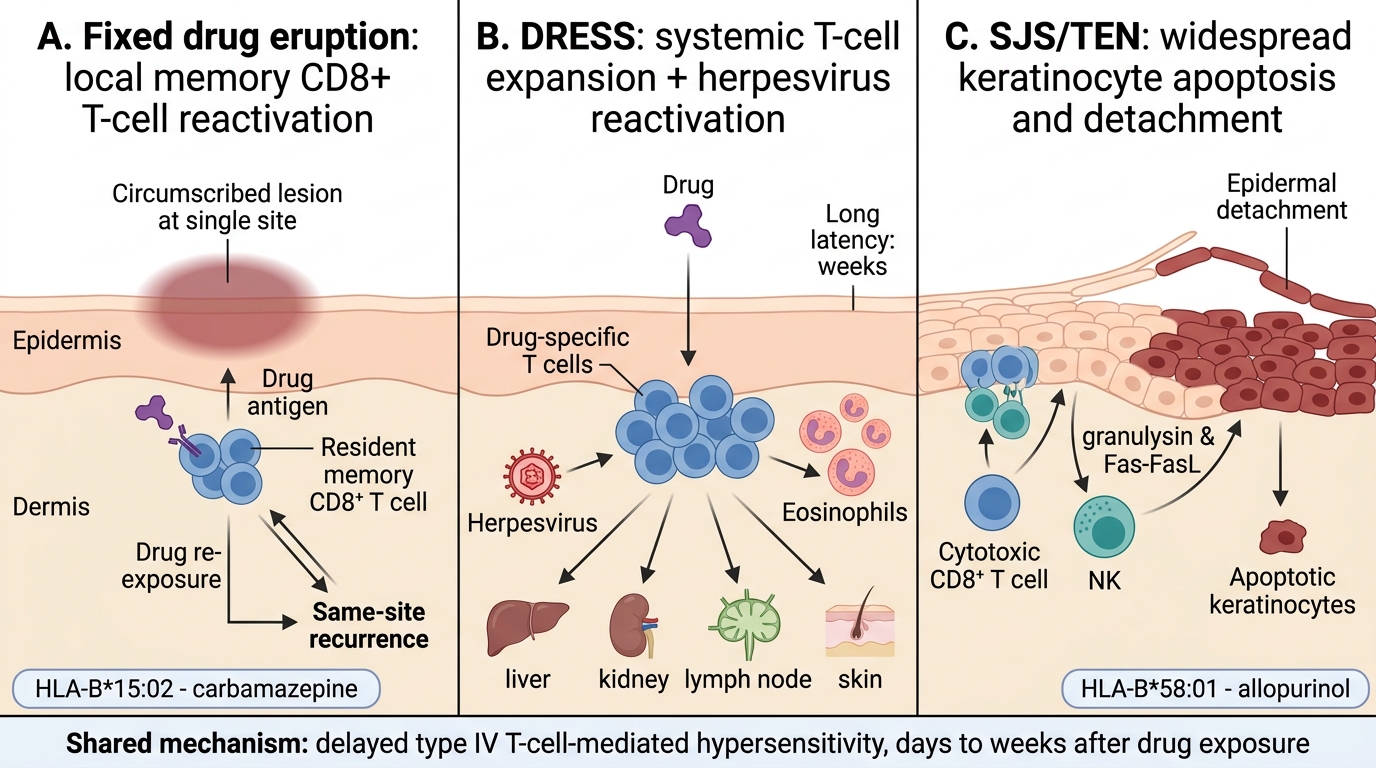
The three reactions of interest share a common immunological theme — type IV, T-cell-mediated hypersensitivity to the drug — but differ in which effector pathway dominates, and this explains their distinct clinical signatures and time-courses. In fixed drug eruption, drug-specific CD8+ tissue-resident memory T cells lie dormant in the skin at the site of a previous reaction; on re-exposure they reactivate locally, releasing inflammatory mediators that reproduce the lesion at exactly the same spot — the basis of its hallmark recurrence. In DRESS, there is a broad expansion of drug-specific T cells, often accompanied by reactivation of latent herpesviruses (such as HHV-6 and EBV), which drives the prolonged, multiorgan illness and explains both the long latency and the eosinophilia.
In SJS/TEN, cytotoxic CD8+ T cells and natural killer cells mount a massive attack on epidermal keratinocytes, triggering widespread apoptosis through mediators such as granulysin and the Fas-Fas-ligand pathway, so that the epidermis dies and separates from the dermis. Genetic susceptibility is striking and clinically useful: certain HLA alleles strongly predispose to SJS/TEN with specific drugs — HLA-B15:02 with carbamazepine and HLA-B58:01 with allopurinol, both important in South and East Asian populations including India. Understanding that all three are delayed T-cell reactions explains why none appears within minutes, and why the culprit drug may have been started days to weeks earlier.
Mechanisms of Severe Cutaneous Drug Reactions
- Fixed drug eruption: local reactivation of resident memory CD8+ T cells → same-site recurrence.
- DRESS: broad drug-specific T-cell expansion + herpesvirus reactivation → multiorgan disease, eosinophilia, long latency.
- SJS/TEN: cytotoxic CD8+ T cells + NK cells → keratinocyte apoptosis (granulysin, Fas-FasL) → epidermal detachment.
- HLA links: HLA-B15:02–carbamazepine; HLA-B58:01–allopurinol (relevant in Indian/Asian populations).
SELF-CHECK
Why do fixed drug eruption, DRESS and SJS/TEN typically appear days to weeks after a drug rather than within minutes?
A. They are IgE-mediated immediate (type I) hypersensitivity reactions
B. They are delayed, T-cell-mediated (type IV) hypersensitivity reactions
C. They are caused by direct toxic overdose of the drug
D. They are complement-mediated (type III) immune-complex reactions
Reveal Answer
Answer: B. They are delayed, T-cell-mediated (type IV) hypersensitivity reactions
Fixed drug eruption, DRESS and SJS/TEN are all predominantly DELAYED type IV (T-cell-mediated) hypersensitivity reactions, which is why they take days to weeks to appear — unlike immediate IgE-mediated (type I) reactions such as urticaria and anaphylaxis that occur within minutes.
Fixed Drug Eruption: Recognising the Recurring Plaque
Fixed Drug Eruption: Same-Site Recurrence
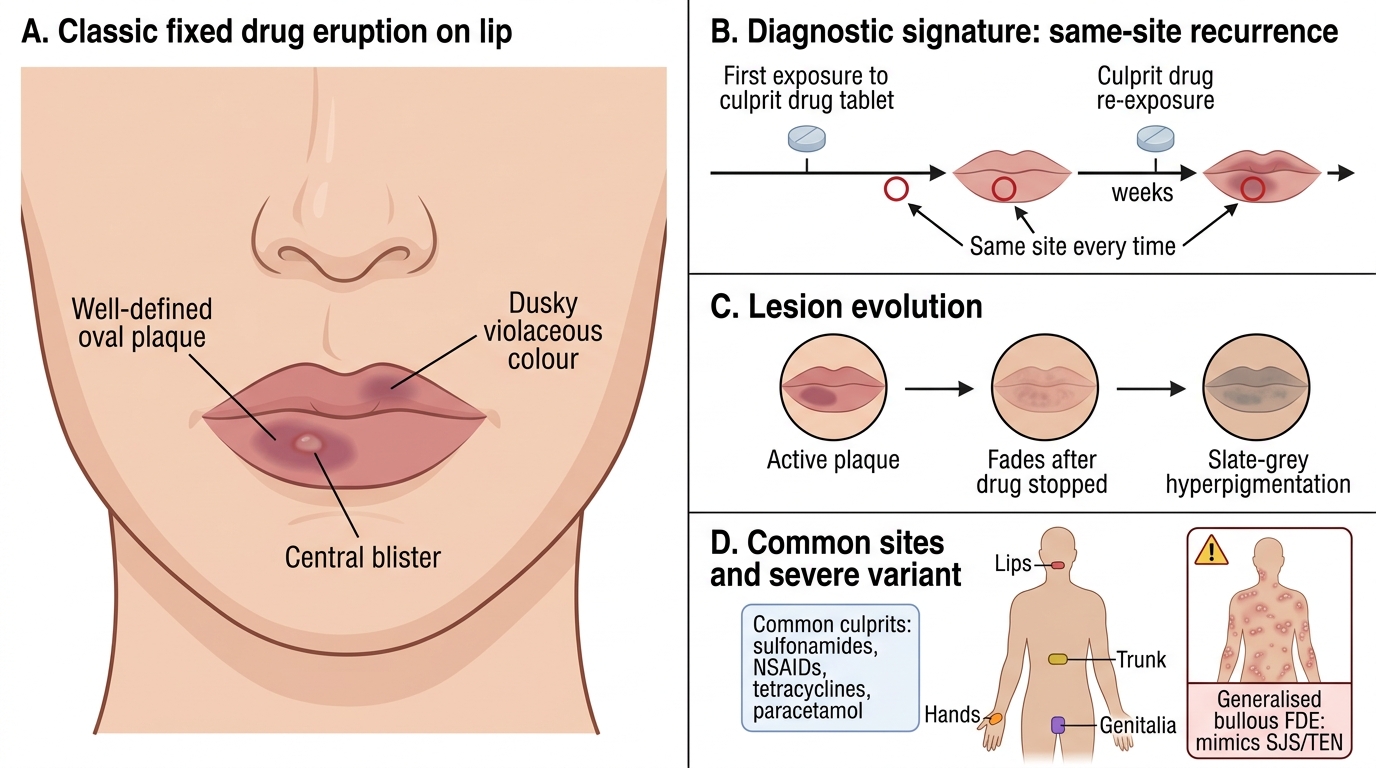
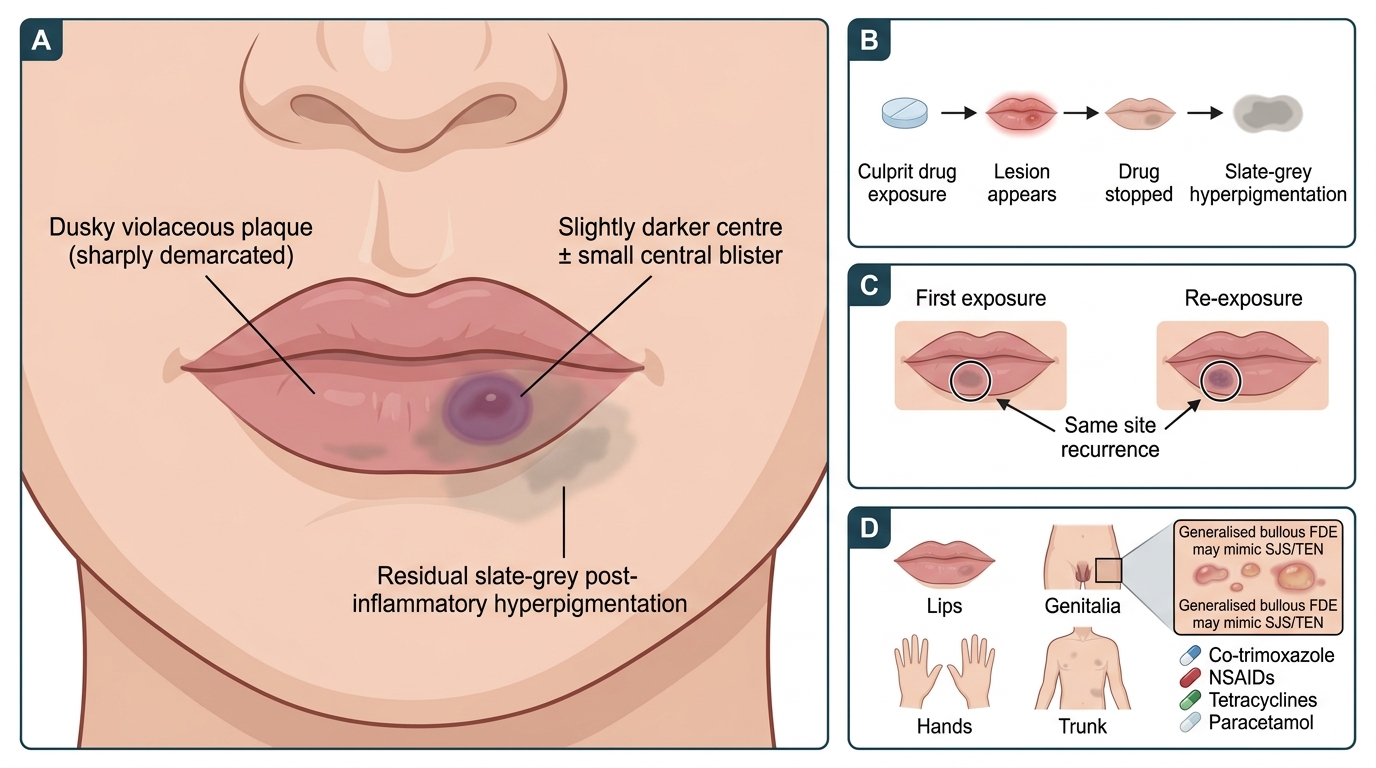
Fixed drug eruption is the most recognisable cutaneous drug reaction once its single defining feature is known: it recurs at exactly the same site every time the culprit drug is taken. The typical lesion is a solitary, or one of a few, well-defined round or oval plaques, dusky red to violaceous in colour, sometimes blistering centrally, and characteristically appearing on the lips, genitalia, hands or trunk. When the drug is stopped the lesion fades but leaves a residual patch of slate-grey post-inflammatory hyperpigmentation, and on every re-exposure the lesion flares again at the same spot — and sometimes at additional new sites. This same-site recurrence is the diagnostic signature that distinguishes it from every other drug reaction.
The common culprits are drugs in everyday use: sulfonamides (including co-trimoxazole), NSAIDs, tetracyclines, and paracetamol, among others. Most fixed drug eruptions are benign and need only identification and avoidance of the drug, but a severe variant — generalised bullous fixed drug eruption — produces widespread blistering that can mimic SJS/TEN and is treated as a severe reaction. The key clinical skill is to ask, when faced with a recurring, well-demarcated pigmented patch, 'does this come back in the same place when you take a particular medicine?' — the answer usually makes the diagnosis.
Fixed Drug Eruption: Same-Site Recurrence
- Hallmark: recurrence at the SAME site on each re-exposure to the culprit drug.
- Lesion: solitary or few well-defined dusky/violaceous plaques; may blister centrally; leaves slate-grey hyperpigmentation.
- Common sites: lips, genitalia, hands, trunk.
- Common culprits: sulfonamides (co-trimoxazole), NSAIDs, tetracyclines, paracetamol.
- Severe variant: generalised bullous fixed drug eruption, which mimics SJS/TEN.