Page 5 of 11
DR11.2 | Dermatologic Reactions to ART Drugs — SDL Guide (Part 2)
Differential Diagnosis and Severity Grading
Severity Grading of HIV-Related Cutaneous Reactions
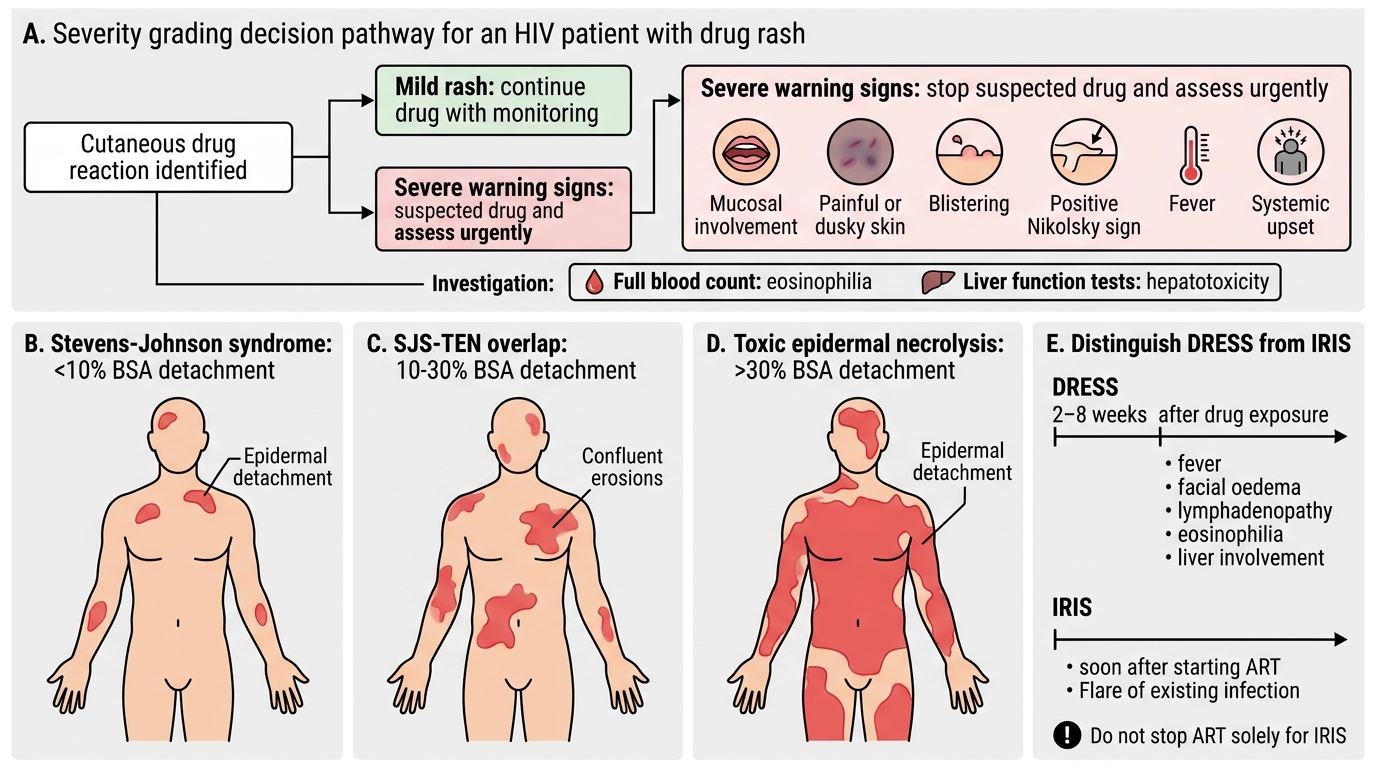
Once a cutaneous reaction is identified, the decisive step is to grade its severity, because this determines whether the drug can be continued or must be stopped. The most important severity framework is the Stevens-Johnson syndrome / toxic epidermal necrolysis spectrum, defined by the body surface area (BSA) of epidermal detachment: Stevens-Johnson syndrome involves less than 10% BSA, the SJS-TEN overlap involves 10–30% BSA, and toxic epidermal necrolysis involves more than 30% BSA. Warning signs that a rash is becoming severe include mucosal involvement, painful or dusky skin, blistering, a positive Nikolsky sign (epidermis shears with lateral pressure), fever, and systemic upset. A second severe reaction to distinguish is DRESS, which presents with a latency of roughly two to eight weeks, fever, facial oedema, lymphadenopathy, eosinophilia, and internal organ involvement (especially the liver). Crucially, both must be separated from IRIS, which is timed to the start of ART and represents a flare of existing infection rather than a drug allergy, and therefore does not call for stopping ART. Investigations support the grading: a full blood count detects the eosinophilia of DRESS, and liver function tests detect the hepatotoxicity that may accompany a nevirapine reaction.
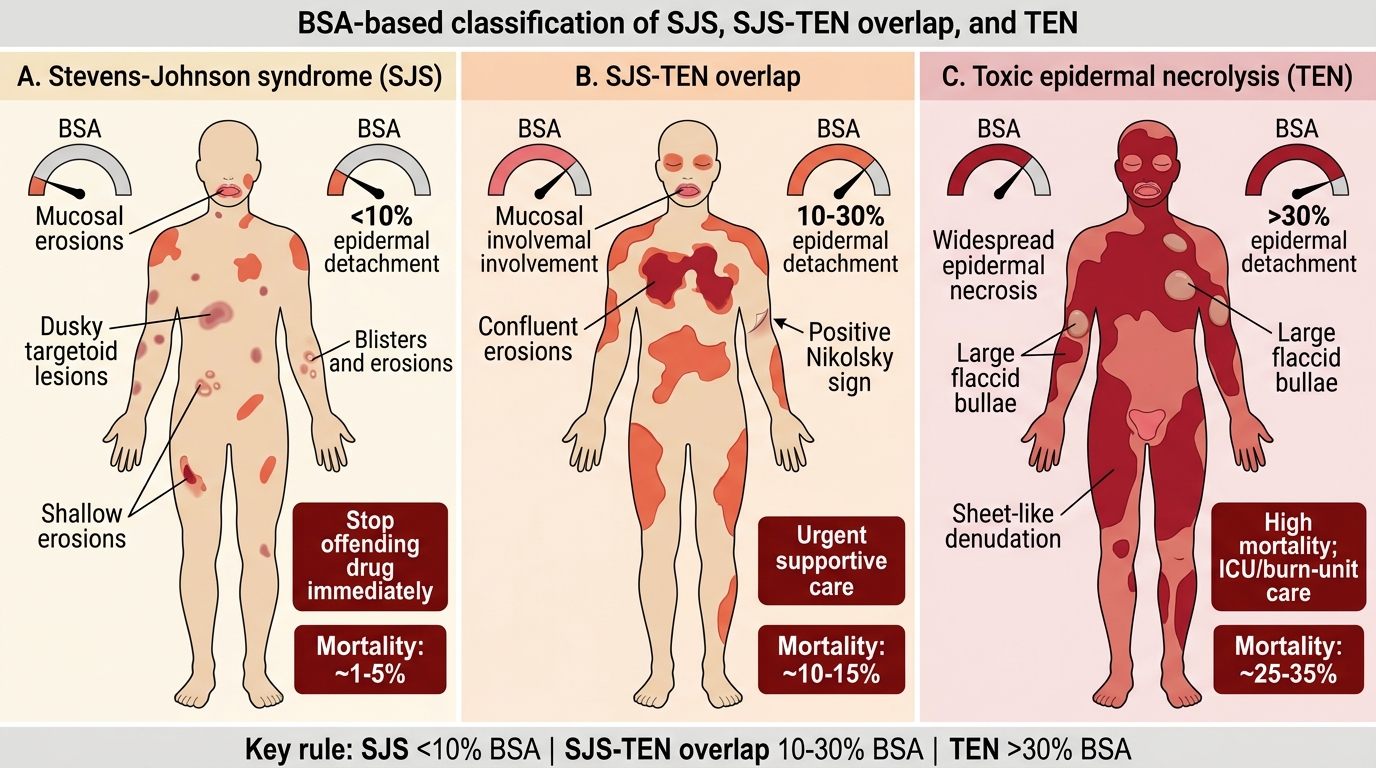
SJS-TEN Spectrum: BSA-Based Classification
SELF-CHECK
A patient on nevirapine has epidermal detachment affecting an estimated 8% of body surface area with mucosal erosions. According to the BSA-based classification, what is this, and what does it imply?
A. Toxic epidermal necrolysis (>30% BSA); a benign self-limiting reaction
B. Stevens-Johnson syndrome (<10% BSA); a severe reaction requiring immediate nevirapine withdrawal
C. A simple morbilliform rash; continue nevirapine with antihistamines
D. DRESS; continue the drug and add an antihistamine
Reveal Answer
Answer: B. Stevens-Johnson syndrome (<10% BSA); a severe reaction requiring immediate nevirapine withdrawal
Epidermal detachment of less than 10% BSA with mucosal involvement defines Stevens-Johnson syndrome. (The SJS-TEN overlap is 10–30% and TEN is greater than 30% BSA.) This is a severe cutaneous adverse reaction: nevirapine must be stopped immediately and never rechallenged, and the patient needs urgent supportive care.
Primary Management and Drug Decisions
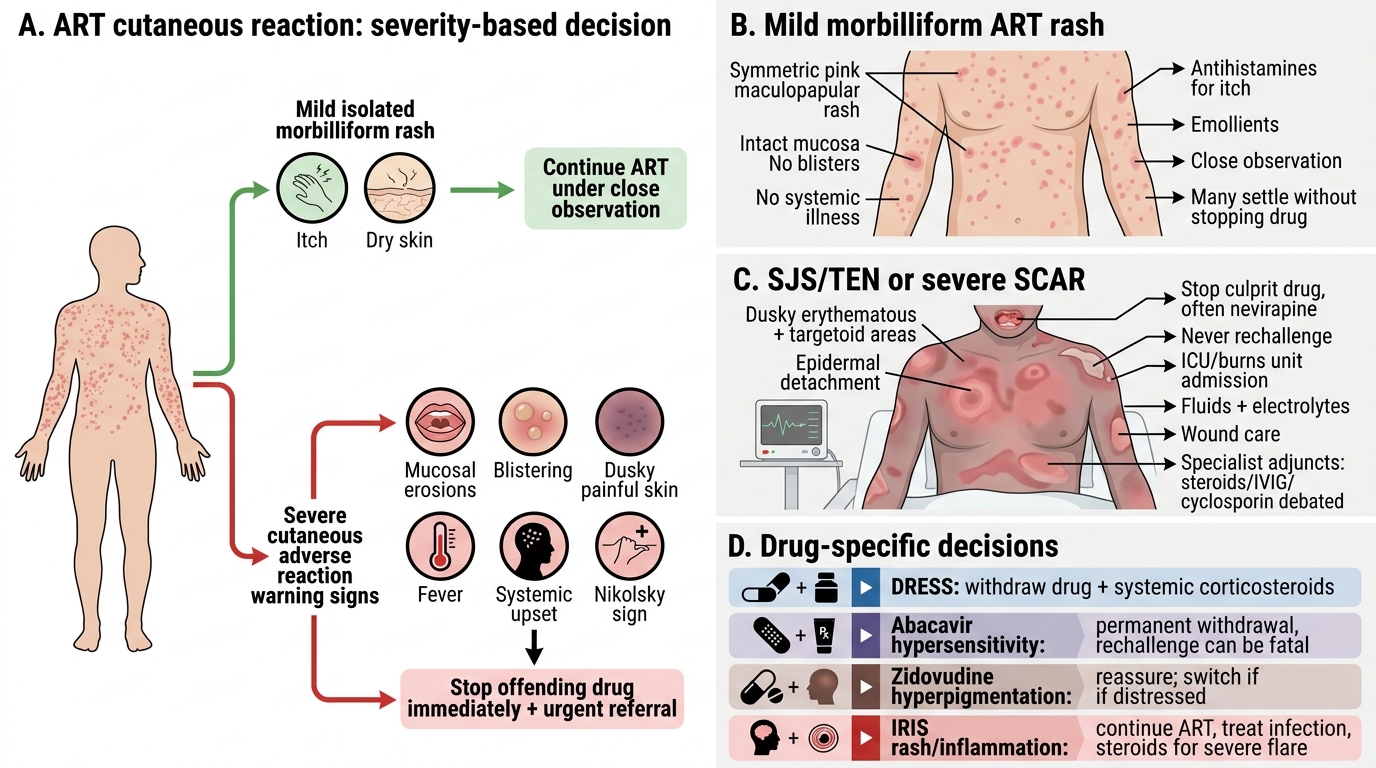
Management of ART-Related Cutaneous Reactions
The management of an ART cutaneous reaction follows directly from its severity grade, and the single most important judgement is whether to continue or to stop the offending drug. A mild, isolated morbilliform rash without systemic features or mucosal involvement can often be managed by continuing the drug under close observation, with antihistamines for itch and emollients — many such rashes settle. By contrast, any reaction with mucosal involvement, blistering, dusky or painful skin, a positive Nikolsky sign, fever, or systemic upset signals a severe cutaneous adverse reaction: the offending drug — most often nevirapine — must be stopped immediately and never rechallenged, and the patient referred urgently. Stevens-Johnson syndrome and toxic epidermal necrolysis require management akin to a burn — admission to an intensive care or burns unit, meticulous fluid and electrolyte support, wound care, and supportive treatment (the role of adjuncts such as systemic corticosteroids, IVIG, or cyclosporin is debated and is a specialist decision). DRESS requires drug withdrawal and systemic corticosteroids. Abacavir hypersensitivity mandates permanent withdrawal, because rechallenge can be fatal. Zidovudine hyperpigmentation needs only reassurance, with a switch if the patient is distressed. IRIS is managed by continuing ART, treating the underlying infection, and adding corticosteroids for severe flares — it is not a reason to stop ART. When nevirapine is stopped for a reaction, an alternative agent such as efavirenz or a protease inhibitor is substituted under specialist guidance (confirm current substitution choices against NACO guidance).
Key management points:
- Mild morbilliform rash, no systemic/mucosal signs: continue under observation + antihistamines
- Severe signs (mucosa, blistering, Nikolsky+, fever): STOP the drug (usually nevirapine) immediately, never rechallenge, refer urgently
- SJS/TEN: ICU/burns-unit-level supportive care (fluids, wound care); adjuncts are a specialist decision
- DRESS: withdraw drug + systemic corticosteroids
- Abacavir hypersensitivity: permanent withdrawal — rechallenge can be fatal
- Zidovudine hyperpigmentation: reassure; switch only if distressing
- IRIS: continue ART, treat the infection, add steroids for severe flares
Self-Assessment: ART Drug Reactions
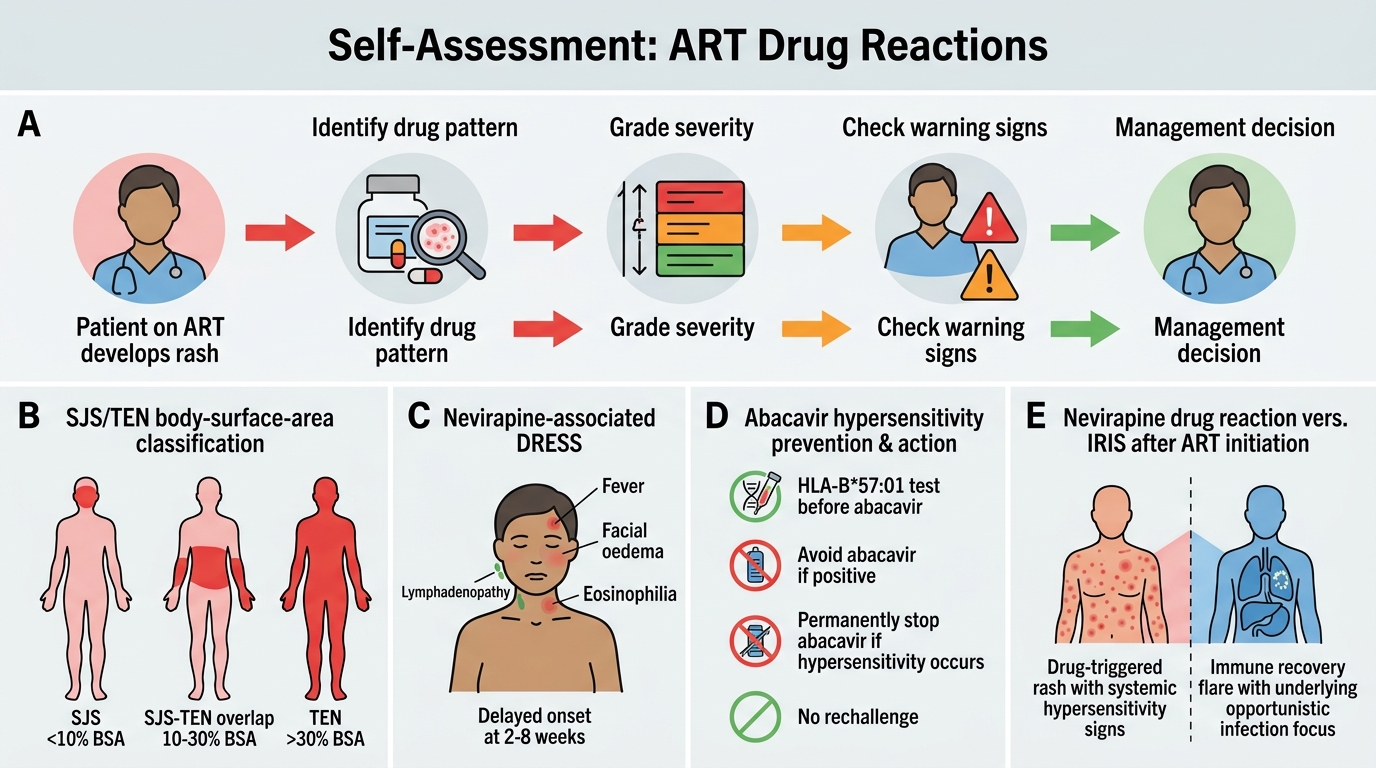
Clinical Self-Assessment of ART Drug Reactions
Having mapped the spectrum of ART cutaneous reactions, their mechanisms, drug-specific patterns, severity grading, and management, it is time to consolidate the decision-making that ties them together. The central competency you should now hold is the ability to take a patient on a known ART regimen, identify the likely offending drug from the reaction pattern, grade the severity using body-surface-area cut-offs and warning signs, and decide whether to reassure and continue or to stop the drug permanently and refer. Reason through the prompts below as clinical decisions rather than as recall items, and where a prompt concerns drug substitution or thresholds, remember to confirm specifics against current NACO antiretroviral therapy guidance. If any answer is unclear, return to the relevant section above and re-trace the link from mechanism to severity to management decision.
Work through these self-check questions:
- State the body-surface-area cut-offs that separate Stevens-Johnson syndrome, SJS-TEN overlap, and toxic epidermal necrolysis.
- A patient develops fever, facial oedema, lymphadenopathy, and eosinophilia six weeks after starting nevirapine — name the reaction and outline its management.
- Explain the significance of HLA-B*57:01 testing before starting abacavir, and the action required if hypersensitivity occurs.
- Differentiate a nevirapine drug reaction from IRIS occurring after ART initiation, and state how the management differs.
- For a mild morbilliform rash with no systemic features, justify why the drug may be continued under observation.
CLINICAL PEARL
For ART rashes, the decision rule is simple: look for the red flags, and if any are present, stop and never rechallenge. The red flags that turn a benign rash into an emergency are mucosal involvement, blistering, dusky or painful skin, a positive Nikolsky sign, fever, and systemic upset. Nevirapine is the ART drug most likely to cause Stevens-Johnson syndrome, toxic epidermal necrolysis, and DRESS, and abacavir hypersensitivity (HLA-B*57:01) is the reaction where rechallenge can kill. Conversely, do not over-react: a mild morbilliform rash without red flags, or zidovudine hyperpigmentation, does not warrant abandoning a working regimen. Knowing which way to jump — continue or stop forever — is the whole of DR11.2.