Page 11 of 23
DR9.4 | Lepra Reaction Treatment — SDL Guide (Part 2)
Investigations and Triggers
Investigations and Triggers in Lepra Reactions
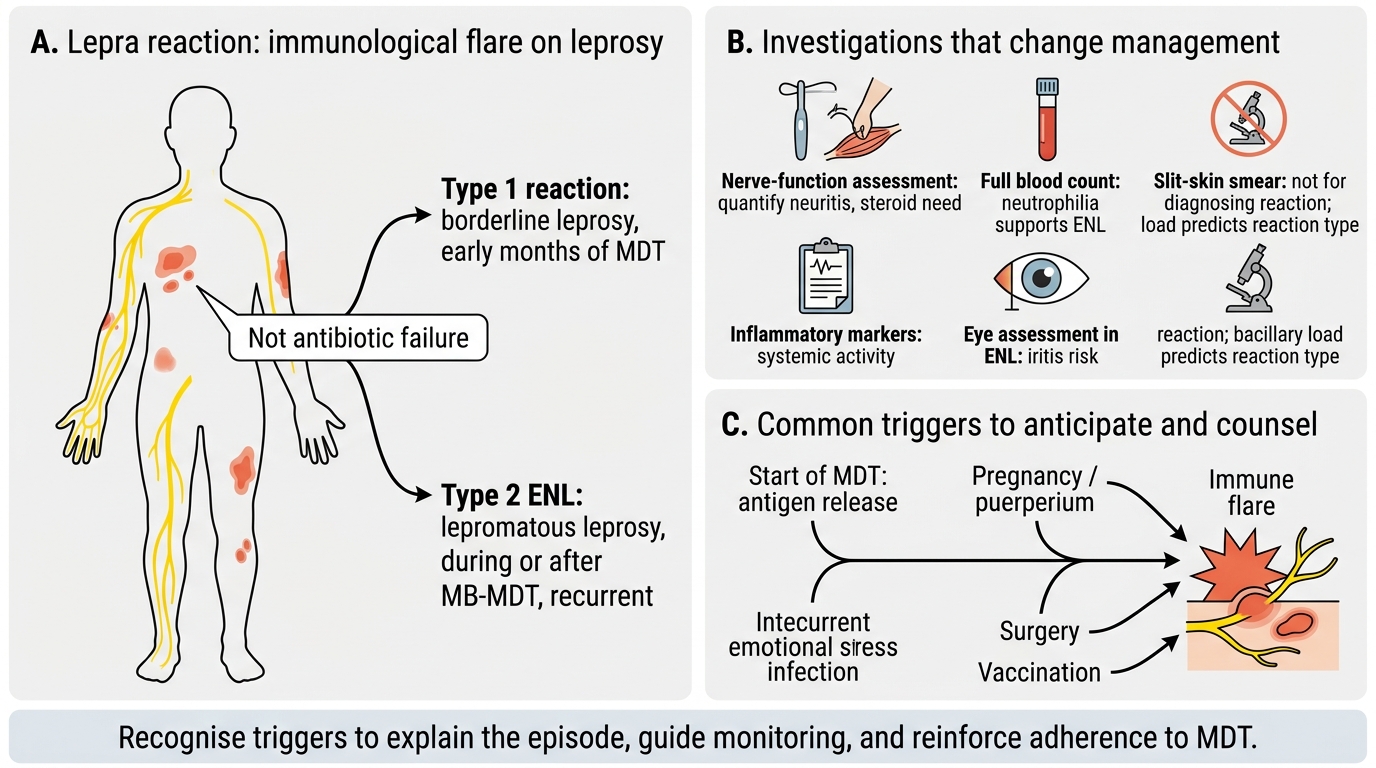
Confirming a lepra reaction and identifying its triggers refines management, because although the diagnosis is largely clinical, certain investigations and a search for precipitants change what you do next. Useful investigations include a nerve-function assessment (essential in every suspected reaction to detect and quantify neuritis and the need for steroids), a full blood count (neutrophilia supports Type 2 ENL), markers of systemic inflammation, and an eye assessment in ENL to detect sight-threatening iritis. A slit-skin smear is not used to diagnose a reaction but the patient's known classification (and bacillary load) tells you which reaction to expect. The fundamental point is that a reaction is an immunological event superimposed on leprosy — it is not evidence that the antibiotics have failed.
Known triggers help you anticipate and counsel. Reactions are commonly precipitated by the initiation of multidrug therapy itself (as bacilli are killed and antigen is released), by pregnancy and the puerperium, by intercurrent infections, by physical and emotional stress, by surgery, and by vaccination. Type 1 reactions cluster in the first months of treatment in borderline patients, while ENL often appears during or after MB therapy in lepromatous patients and is notoriously recurrent. Recognising a trigger does not change the immediate treatment but helps explain the episode to the patient, guides monitoring, and reinforces the message that the appearance of a reaction is expected and manageable, not a reason to abandon therapy.
Investigations and triggers to remember:
- Investigate: nerve-function assessment (always), FBC (neutrophilia in ENL), eye exam in ENL.
- Triggers: starting MDT, pregnancy/puerperium, infection, stress, surgery, vaccination.
- A reaction is an immune event, not antibiotic failure — MDT continues.
Treatment Regimens — Corticosteroids, Clofazimine, and Thalidomide
Treatment of Lepra Reactions: Steroids, Clofazimine, and Thalidomide
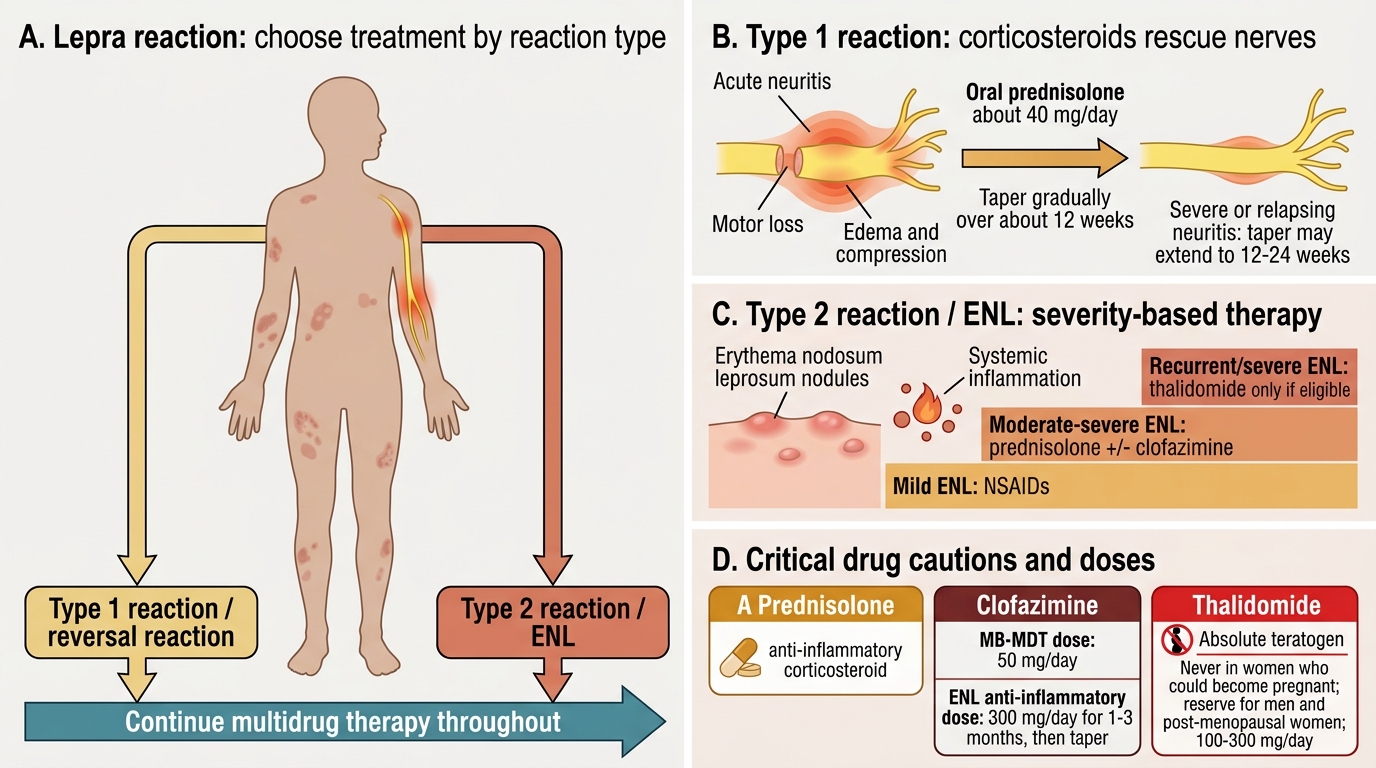
Treating a lepra reaction correctly means matching the drug to the reaction type while observing two unbreakable rules: continue multidrug therapy throughout, and never give thalidomide to a woman who could become pregnant. For a Type 1 (reversal) reaction, the mainstay is a corticosteroid — typically oral prednisolone, started at around 40 mg/day and tapered gradually over roughly 12 weeks (often up to 12-24 weeks for severe or relapsing neuritis), the aim being to suppress the inflammation rapidly and rescue nerve function. Mild reactions without neuritis may be managed with rest and analgesics, but any acute neuritis or motor loss mandates corticosteroids urgently.
For a Type 2 reaction (ENL), treatment depends on severity but the principal agents are corticosteroids, clofazimine, and thalidomide. Mild ENL may respond to NSAIDs; moderate-to-severe ENL is treated with prednisolone and/or clofazimine in an anti-inflammatory dose. It is essential to distinguish clofazimine's two doses: as part of MB-MDT it is given at 50 mg/day, but for its anti-inflammatory effect in ENL it is used at a much higher 300 mg/day (for one to three months, then tapered). Thalidomide is the most effective drug for severe or recurrent ENL but is an absolute teratogen — it is contraindicated in all women of childbearing potential and reserved for men and post-menopausal women, used at around 100-300 mg/day. Recurrent ENL may require long-term low-dose clofazimine to reduce the frequency of episodes.
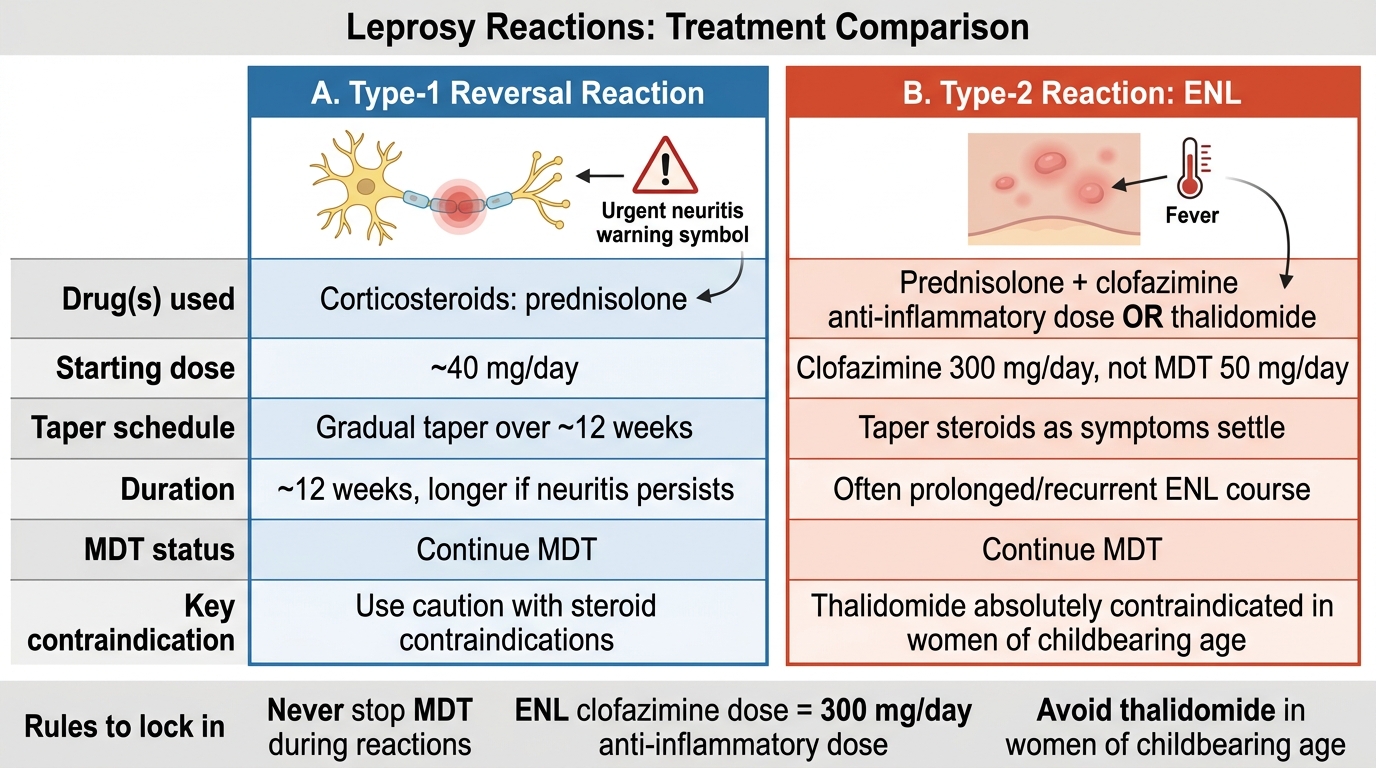
Treatment of Leprosy Reactions: Type-1 vs Type-2 ENL
Treatment rules to lock in:
- Type 1 → corticosteroids (prednisolone ~40 mg/day, taper over ~12 weeks); urgent if neuritis.
- Type 2 (ENL) → corticosteroids + clofazimine (anti-inflammatory dose 300 mg/day, NOT the 50 mg/day MDT dose) or thalidomide.
- Thalidomide is absolutely contraindicated in women of childbearing age (teratogen).
- Continue MDT through every reaction — never stop it.
SELF-CHECK
A 25-year-old woman with lepromatous leprosy on multidrug therapy develops severe, recurrent erythema nodosum leprosum (ENL) with fever and tender nodules. Which treatment plan is correct?
A. Start thalidomide as first choice because it is the most effective drug for ENL
B. Treat with corticosteroids and/or clofazimine at an anti-inflammatory dose (300 mg/day); avoid thalidomide because she is of childbearing age; continue MDT
C. Stop MDT immediately and give clofazimine 50 mg/day
D. Give corticosteroids and reduce the MDT clofazimine to treat the ENL
Reveal Answer
Answer: B. Treat with corticosteroids and/or clofazimine at an anti-inflammatory dose (300 mg/day); avoid thalidomide because she is of childbearing age; continue MDT
This is a severe Type 2 reaction (ENL). Appropriate treatment is corticosteroids (prednisolone) and/or clofazimine at the anti-inflammatory dose of 300 mg/day (distinct from the 50 mg/day MDT dose). Thalidomide, although highly effective for ENL, is an ABSOLUTE teratogen and is contraindicated in women of childbearing age — so it must be avoided here despite its efficacy. Multidrug therapy is CONTINUED throughout the reaction, never stopped, because the reaction is an immunological event, not antibiotic failure.
Self-Assessment — Lepra Reaction Treatment
Consolidate this module by reasoning from presentation to a precise treatment plan, because in a real reaction you must decide the type and the drug quickly and correctly. For each scenario, run the same chain: identify the reaction type from the skin pattern and the patient's place on the spectrum, name the immunological mechanism, decide the drug(s) and dose, check for the thalidomide contraindication, and confirm that multidrug therapy continues. Hold two facts immovably in mind: that Type 1 is treated with corticosteroids while Type 2 may additionally need clofazimine (at the 300 mg/day anti-inflammatory dose, not the 50 mg/day MDT dose) or thalidomide, and that thalidomide is absolutely forbidden in any woman who could become pregnant.
Test yourself on these:
- A BT patient two months into MDT with inflamed existing patches and a tender ulnar nerve losing power — name the reaction, the mechanism, and the regimen, and state whether to stop MDT.
- A young woman with LL leprosy and severe recurrent ENL — which drugs are appropriate, which is contraindicated and why?
- Explain the difference between clofazimine's MDT dose and its anti-ENL dose, and when each is used.
- A post-menopausal man with severe ENL not controlled by steroids — what additional drug is now an option that would be forbidden in a younger woman?
If you can move from the clinical picture to the correct reaction type and a safe, correct regimen for each, while never stopping MDT, you have met the objective of this high-stakes module.
CLINICAL PEARL
Acute neuritis in a Type 1 reaction is a corticosteroid emergency — start prednisolone the same day to save the nerve — and never stop multidrug therapy during any reaction. Keep the two reactions firmly separated: Type 1 (reversal) is T-cell-mediated, hits BORDERLINE patients, inflames EXISTING lesions, threatens nerves, and is treated with corticosteroids; Type 2 (ENL) is immune-complex-mediated, hits LEPROMATOUS patients, erupts as crops of NEW tender nodules with systemic features, and is treated with corticosteroids plus clofazimine or thalidomide. Two dose traps catch the unwary: clofazimine for ENL is the high anti-inflammatory dose of 300 mg/day, not the 50 mg/day MDT dose; and thalidomide, the most effective ENL drug, is an absolute teratogen forbidden in any woman of childbearing age. Get the type right, pick the right drug, watch the dose, protect against pregnancy, and keep the antibiotics running.