Page 17 of 23
DR9.5 | Leprosy Management Under National Guidelines — SDL Guide (Part 2)
ADRs, Monitoring, and Special Situations
⚑ AI image — pending faculty review (auto-QA score 6/10; best of 3 attempts)
ADRs and Special Situations in Leprosy MDT
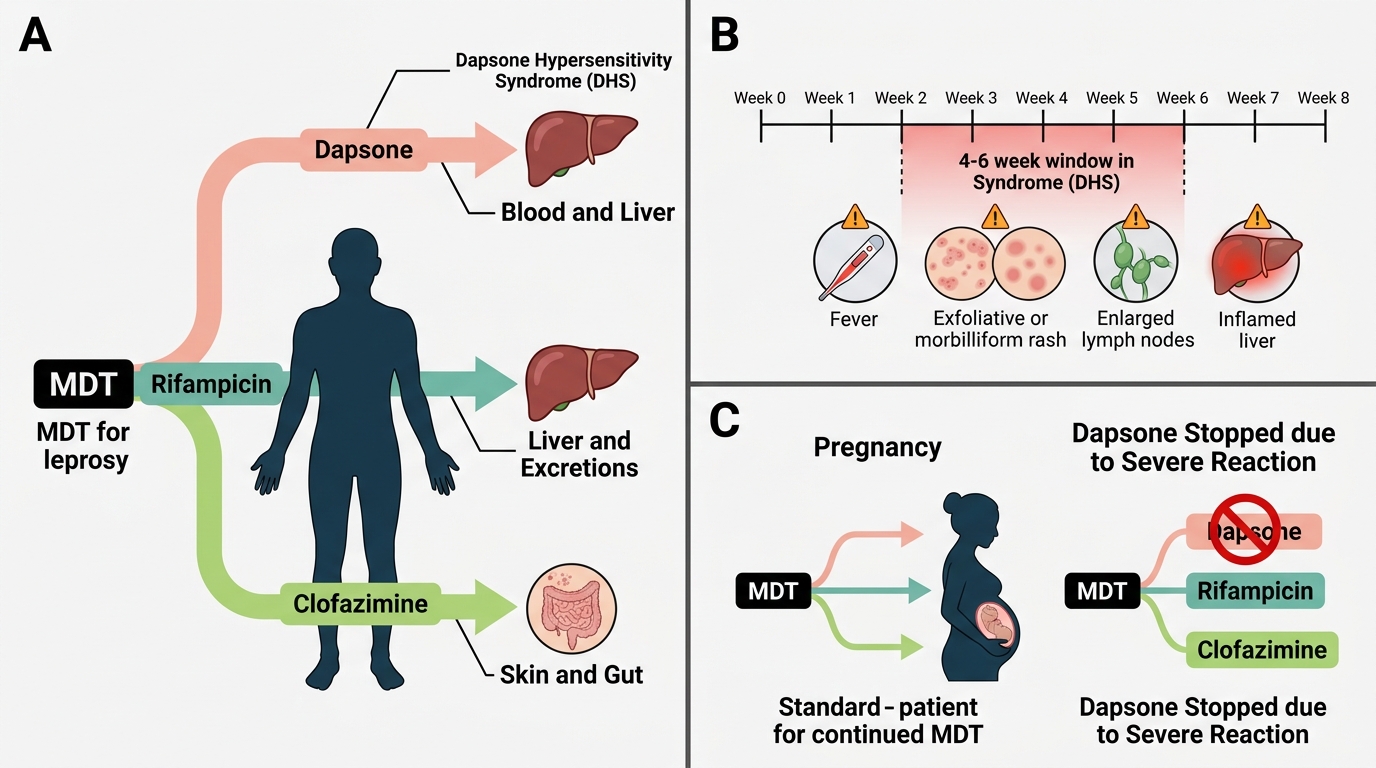
Managing leprosy well means anticipating the adverse effects of the three drugs so that you neither stop treatment unnecessarily nor miss a dangerous reaction, and so that you can reassure patients about the harmless effects. Dapsone can cause dose-related haemolytic anaemia (especially in G6PD deficiency) and methaemoglobinaemia, and — most seriously — the dapsone hypersensitivity syndrome, a potentially fatal reaction typically appearing around 4-6 weeks into treatment with fever, an exfoliative or morbilliform rash, lymphadenopathy, and hepatitis; it demands immediate cessation of dapsone. Rifampicin causes hepatotoxicity, a harmless orange-red discolouration of urine, sweat, and tears (warn the patient in advance), and important enzyme-inducing drug interactions that reduce the efficacy of oral contraceptives, warfarin, and antiretrovirals. Clofazimine causes a characteristic dose-dependent reddish-brown to black skin pigmentation and ichthyosis (dryness) that are reversible after stopping, plus gastrointestinal upset.
Special situations require judgement rather than reflexive drug withdrawal. In pregnancy, standard MDT is considered safe and should NOT be withheld — leprosy itself, and untreated reactions, pose greater risks; clofazimine may cause harmless reversible pigmentation of the neonatal skin. When dapsone must be stopped (for hypersensitivity or severe haemolysis), it can be omitted and the remaining drugs continued, or substituted per programme guidance. Monitoring is largely clinical — looking for drug toxicity, nerve-function impairment, and reactions at each visit — supplemented by relevant tests (e.g., liver function if hepatotoxicity is suspected).
Key adverse-effect points:
- Dapsone: haemolysis (G6PD), methaemoglobinaemia, and dapsone hypersensitivity syndrome (~4-6 weeks; fever, rash, hepatitis — stop dapsone immediately).
- Rifampicin: hepatotoxicity, harmless orange-red secretions (warn the patient), enzyme-inducing interactions (OCP, warfarin, ART).
- Clofazimine: reversible reddish-brown/black skin pigmentation, dryness, GI upset.
- Pregnancy: continue standard MDT — do not withhold it.
NLEP Framework — Notification, Surveillance, and Post-MDT Monitoring
NLEP Framework for Leprosy Care and Surveillance
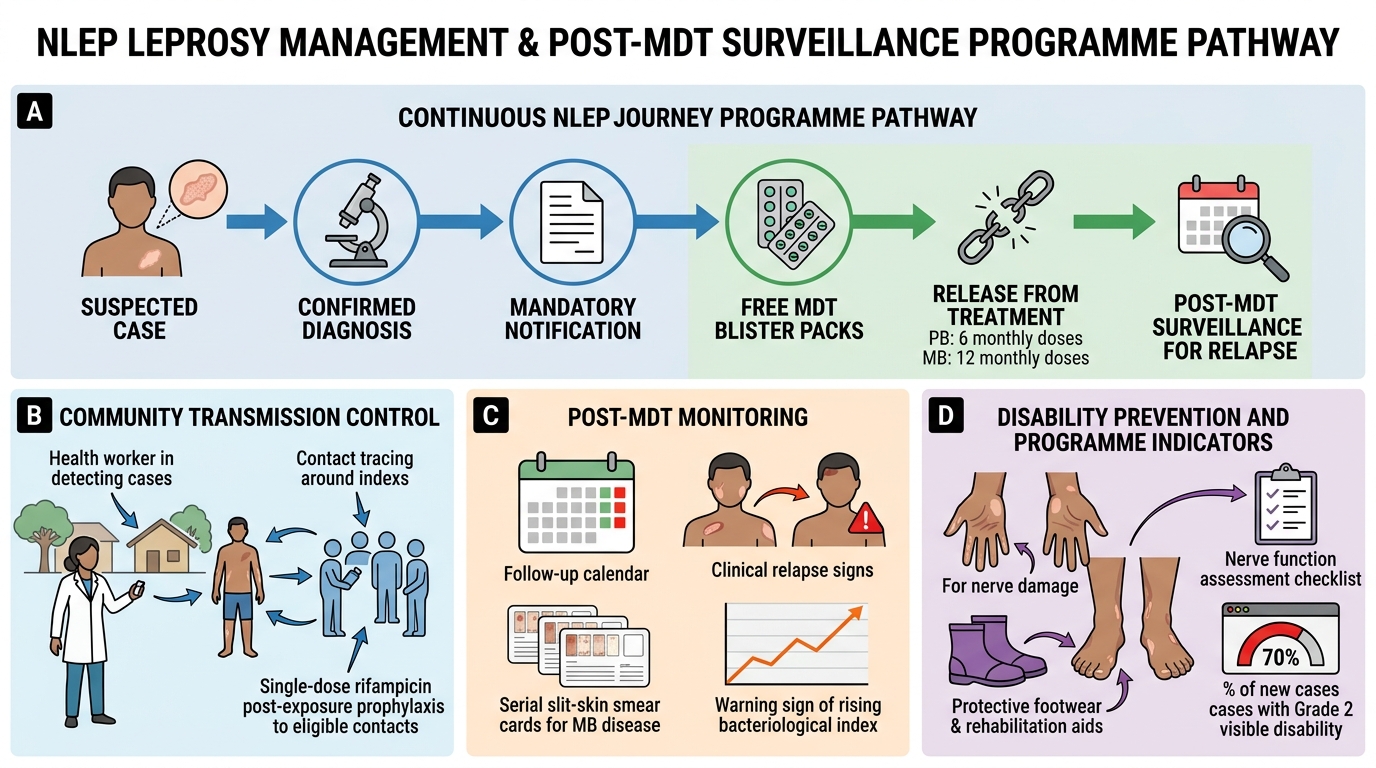
Managing a case of leprosy means operating within the National Leprosy Eradication Programme, because leprosy care in India is a programmatic activity, not just an individual prescription. NLEP integrates leprosy services into general health care, supplies MDT free in blister packs, and treats leprosy as a notifiable condition so that every case is recorded and the programme can monitor the disease burden. On completing the prescribed course the patient is formally released from treatment (RFT) — after 6 monthly doses for PB or 12 for MB — and entered into a period of surveillance to detect relapse, which is signalled clinically and, in MB patients, by a rising bacteriological index on serial smears.
Beyond treating the index patient, NLEP pursues transmission control and disability prevention at the population level. This includes active case-detection campaigns to find hidden cases early (before disability develops), contact tracing of household and close contacts, and single-dose rifampicin post-exposure prophylaxis (SDR-PEP) offered to eligible contacts to reduce their risk of developing disease. The programme also runs Disability Prevention and Medical Rehabilitation (DPMR) services for patients who already have nerve damage, and it tracks indicators such as the proportion of new patients presenting with Grade 2 (visible) disability, which is a marker of how early cases are being detected.
Programme essentials:
- Leprosy is notifiable; MDT is free in blister packs; care is integrated into general health services.
- Release from treatment (RFT) after the completed course; then relapse surveillance (rising BI in MB).
- Population measures: active case detection, contact tracing, and single-dose rifampicin prophylaxis (SDR-PEP) for contacts; DPMR for disability.
SELF-CHECK
A patient on MDT develops fever, a widespread exfoliative rash, lymphadenopathy, and deranged liver function about 5 weeks after starting treatment. Which drug is the most likely cause and what is the immediate action?
A. Clofazimine — reassure the patient that the skin changes are harmless and continue treatment
B. Dapsone — this is dapsone hypersensitivity syndrome; stop dapsone immediately
C. Rifampicin — this is the expected orange discolouration; no action needed
D. Dapsone — reduce the dose by half and continue without further monitoring
Reveal Answer
Answer: B. Dapsone — this is dapsone hypersensitivity syndrome; stop dapsone immediately
Fever, exfoliative rash, lymphadenopathy, and hepatitis appearing around 4-6 weeks into treatment is the dapsone hypersensitivity syndrome — a potentially fatal reaction to dapsone. The immediate action is to STOP dapsone at once (not merely reduce it) and provide supportive care; the other MDT drugs can be continued or the regimen adjusted per programme guidance. Clofazimine's skin pigmentation and rifampicin's orange secretions are harmless and would not cause this picture; this is a drug emergency, not a benign effect.
Self-Assessment — Leprosy Management
Consolidate this module by prescribing and problem-solving through realistic cases, because the management competency is tested precisely on getting the drugs, doses, and duration exactly right. For each scenario, reason in a fixed order: classify the patient (PB or MB, remembering that a positive smear always means MB), select the correct regimen with exact drugs and duration, adjust for age or special situations such as pregnancy, and then handle any adverse-drug-reaction or surveillance question on its own merits. Keep the two regimens cleanly separated in your mind — PB is two drugs for six months with no clofazimine; MB is three drugs for twelve months — and never drop clofazimine from MB or shorten its course.
Work through these checkpoints:
- A patient with 7 lesions and a positive ear-lobe smear (BI 3+): state the full regimen with drugs, doses, and duration.
- A 12-year-old child with paucibacillary disease: give the adjusted regimen.
- A patient develops jaundice on MDT: which drug is the likely culprit, and how do you proceed?
- A pregnant woman is newly diagnosed with MB leprosy: should MDT be started, and is it safe?
- A patient completed MB-MDT two years ago and now has a rising BI on serial smears: what does this indicate within the NLEP framework?
If you can classify, prescribe the exact correct regimen, adjust for special cases, and manage drug toxicity and surveillance for each, you have met the core objective of this module.
CLINICAL PEARL
Lock the two regimens in memory exactly: PB-MDT = rifampicin + dapsone for 6 months (no clofazimine); MB-MDT = rifampicin + dapsone + clofazimine for 12 months — and a positive smear at any site always means MB. The two most damaging prescribing errors are dropping clofazimine from an MB regimen and giving the 6-month PB course to a smear-positive patient; both lead to relapse. Warn every patient that rifampicin turns urine, sweat, and tears orange (harmless) and that clofazimine darkens the skin (reversible), so they do not stop their tablets in alarm. Stay alert for the one true drug emergency — dapsone hypersensitivity syndrome at 4-6 weeks (fever, exfoliative rash, hepatitis) — and stop dapsone at once. Finally, never withhold MDT in pregnancy, and remember rifampicin's enzyme induction makes oral contraceptives unreliable.