Page 1 of 12
DR15.1-2 | Pyoderma Presentation and Antimicrobial Treatment — SDL Guide
Learning Objectives
- Identify and classify the clinical presentation of the common types of cutaneous bacterial infection (impetigo, ecthyma, folliculitis, furuncle, carbuncle, cellulitis, erysipelas, SSSS) by morphology and depth
- Describe the microbial pathogenesis that explains why each pyoderma type looks the way it does
- Distinguish pyoderma types from one another and from key clinical mimics, and recognise when bacteriological investigation is warranted
- Enumerate the indications and adverse reactions of the topical drugs (mupirocin, fusidic acid) used to treat pyoderma
- Enumerate the indications and adverse reactions of the systemic antimicrobials (anti-staphylococcal beta-lactams, macrolides, and MRSA-active agents) used to treat pyoderma
INSTRUCTIONS
Pyoderma is among the most common reasons a patient presents to the general practitioner, the paediatrician, and the dermatology outpatient clinic in India. The clinician who can read the skin lesion accurately — distinguishing a honey-crusted impetigo from a punched-out ecthyma, a localised furuncle from a spreading cellulitis — chooses the right drug, the right route, and the right duration the first time. With antimicrobial resistance rising, especially community-acquired MRSA and increasing topical mupirocin resistance, rational antibiotic selection in pyoderma is no longer routine. This SDL builds the bridge from what you see on the skin to what you prescribe, equipping you to treat the common bacterial skin infections you will meet every day of your clinical career.
References
- Sacchidanand S, et al. IADVL Textbook of Dermatology, 4th ed. Ch: Bacterial Infections of the Skin (Pyodermas) (textbook)
- Khanna N. Illustrated Synopsis of Dermatology and Sexually Transmitted Diseases, 6th ed. Ch: Bacterial Infections (textbook)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
A 4-year-old is brought to the clinic with golden-yellow crusted sores clustered around the nose and mouth that appeared over three days and are spreading to the cheeks. In the next cubicle, a 50-year-old diabetic man has a tender red swelling on the back of his neck with several pus-points, and he feels feverish. Both have a pyoderma — a pyogenic bacterial skin infection — yet they need very different treatment. The child's localised honey-crusted lesions may clear with a topical antibiotic; the man's deep, multi-headed lesion will need a systemic anti-staphylococcal drug and possibly more. Knowing which lesion is which, and which drug each one needs, is the everyday skill this module builds.
WHY THIS MATTERS
Bacterial skin infections are one of the highest-volume presentations in Indian primary care, paediatric practice, and dermatology outpatient departments. Getting them right matters for three reasons. First, the right diagnosis selects the right therapy: a topical antibiotic wastes time on a deep abscess, while a systemic drug over-treats a trivial localised impetigo and drives resistance. Second, recognising the organism pattern — Staphylococcus aureus versus Streptococcus pyogenes — guides empiric choice and warns you when MRSA must be covered. Third, a missed spreading infection (cellulitis, erysipelas) can progress to systemic sepsis. Every prescription you write for a skin infection is also an antibiotic-stewardship decision, so reading the lesion accurately is both a clinical and a public-health responsibility.
RECALL
Before we begin, recall three foundations from your earlier years. From Microbiology: Staphylococcus aureus is a coagulase-positive, Gram-positive cluster-forming coccus that produces exotoxins (including exfoliative toxins); Streptococcus pyogenes is a Group A, beta-haemolytic, Gram-positive chain-forming coccus that spreads through tissue using hyaluronidase and streptolysins. From Anatomy: the skin is layered into epidermis, dermis, and subcutaneous tissue, and hair follicles are invaginations that descend into the dermis — depth determines what we call the infection. From Pharmacology: beta-lactam antibiotics kill bacteria by inhibiting cell-wall transpeptidases (penicillin-binding proteins), and resistance arises when bacteria produce beta-lactamase or alter the target protein (as in MRSA). Hold these three threads — organism, depth, and drug mechanism — as we work through the spectrum of pyoderma.
Morphological Spectrum of Pyoderma: What You See on the Skin
Morphological Spectrum of Pyoderma
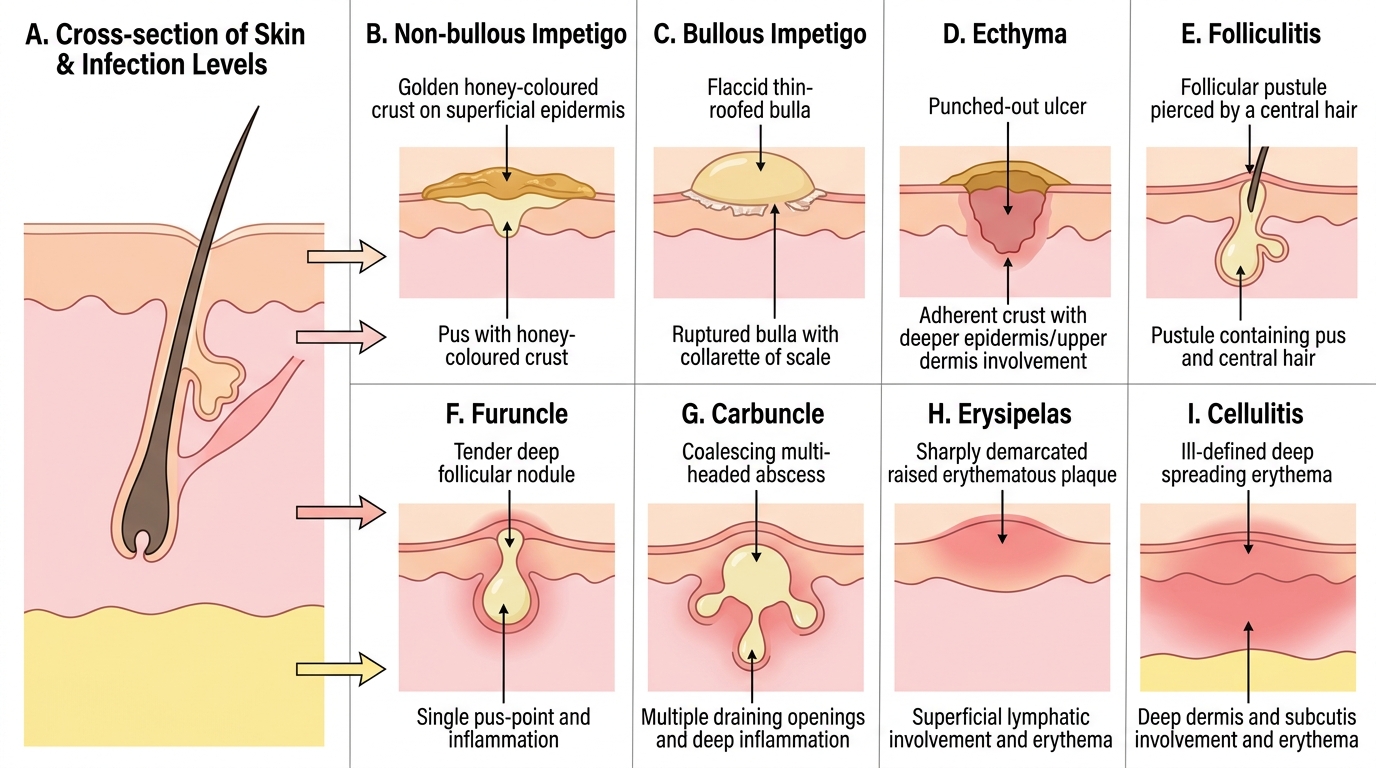
Pyoderma is best understood first through what you see and where it sits in the skin, because depth and primary lesion together name the condition before any culture is taken. The skin can be infected at three broad levels: the superficial epidermis (where you see crusts and flaccid bullae), the hair follicle (where you see pustules and tender nodules), and the deeper dermis and subcutis (where you see diffuse spreading erythema). A clinician trained to read the primary lesion — crust, bulla, ulcer, pustule, nodule, or ill-defined plaque — and to judge its depth on palpation can pattern-recognise the pyoderma type at the bedside, then confirm the likely organism from that pattern.
The morphological vocabulary maps onto the named types as follows:
- Crust (honey-coloured) at the surface → impetigo (non-bullous)
- Flaccid bulla that ruptures to leave a collarette → bullous impetigo
- Punched-out ulcer with an adherent crust → ecthyma (a deeper, ulcerative infection)
- Follicular pustule pierced by a hair → folliculitis
- Tender deep nodule with a single pus-point → furuncle (boil)
- Coalescing multi-headed abscess → carbuncle
- Sharply-demarcated raised red plaque → erysipelas
- Ill-defined, deep, spreading erythema → cellulitis
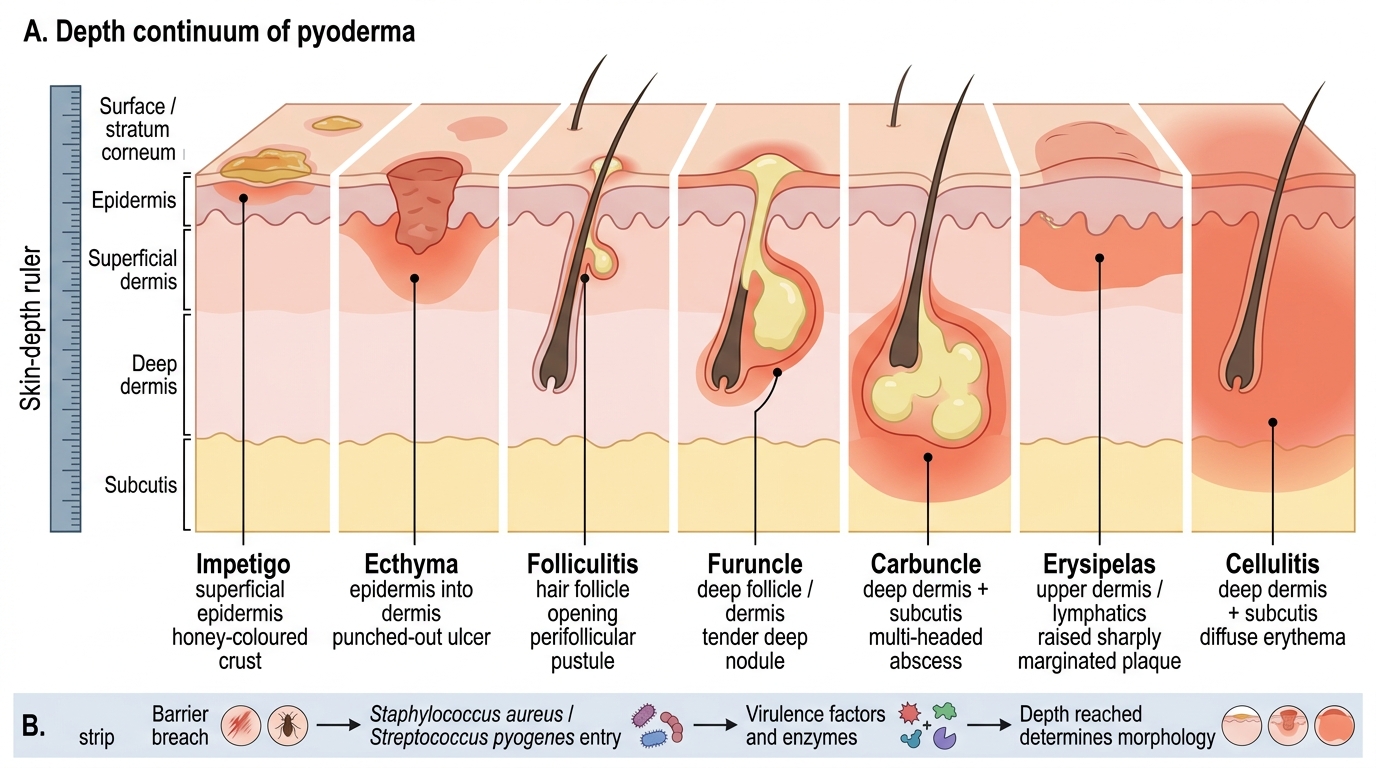
Depth Continuum of Pyoderma
Reading depth and primary lesion first is the habit that keeps your subsequent diagnosis and drug choice on track.
Pathogenesis: How Bacteria Invade and Damage Skin
Pathogenesis of Pyoderma Lesions
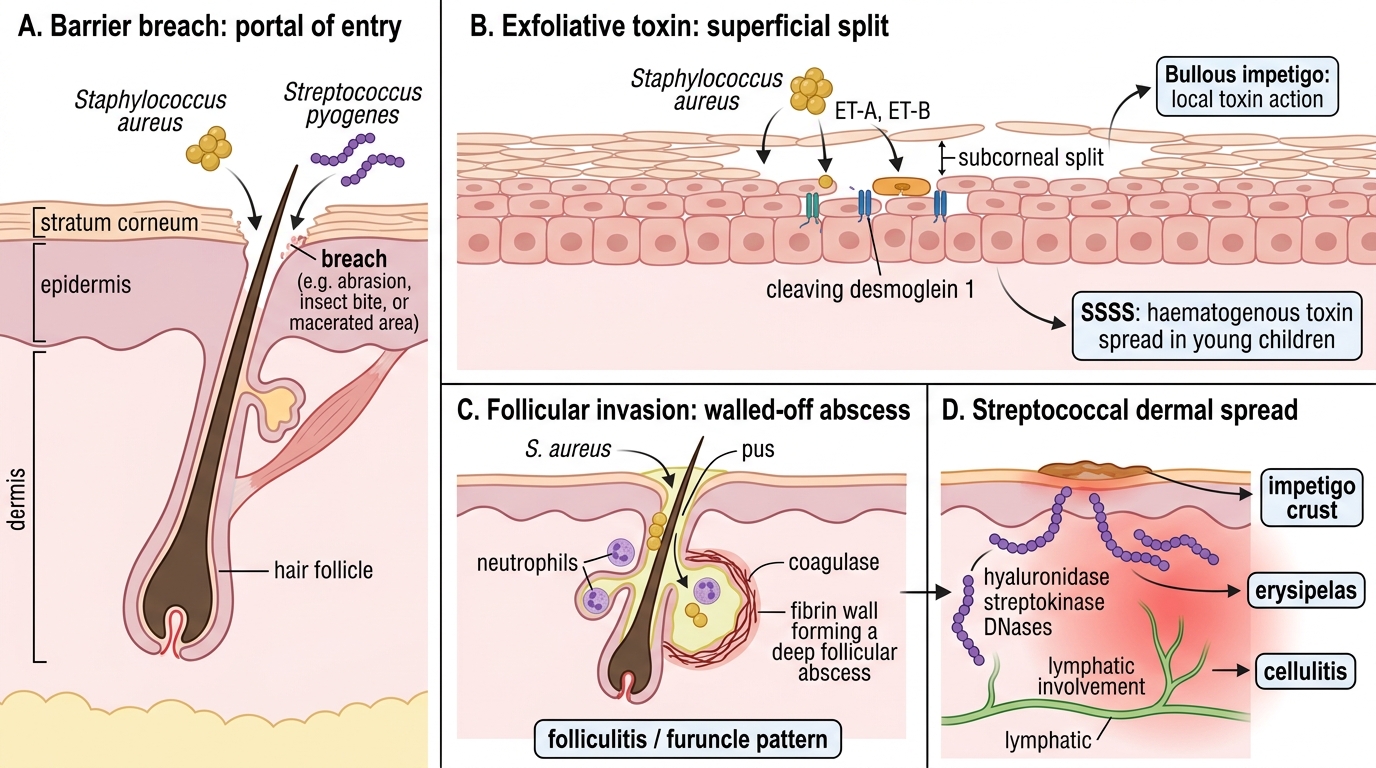
The clinical appearance of each pyoderma is the visible footprint of a specific microbial mechanism, so understanding pathogenesis explains why the lesions differ from one another. Two organisms dominate the picture: Staphylococcus aureus and Streptococcus pyogenes. Both must first breach the skin barrier — through a minor abrasion, an insect bite, maceration, or an existing dermatosis such as eczema or scabies — because intact, healthy skin resists colonisation by these organisms. Once the barrier is breached and the organism has entered, its particular set of virulence factors determines whether the result is a surface crust, a flaccid blister, a deep follicular abscess, or a rapidly spreading dermal infection. This is precisely why the same two bacteria, depending on which toxins and enzymes they deploy and how deep they reach, can produce such strikingly different-looking diseases on the skin. Mapping each mechanism to its lesion is therefore the key to remembering the spectrum.
The key mechanisms are:
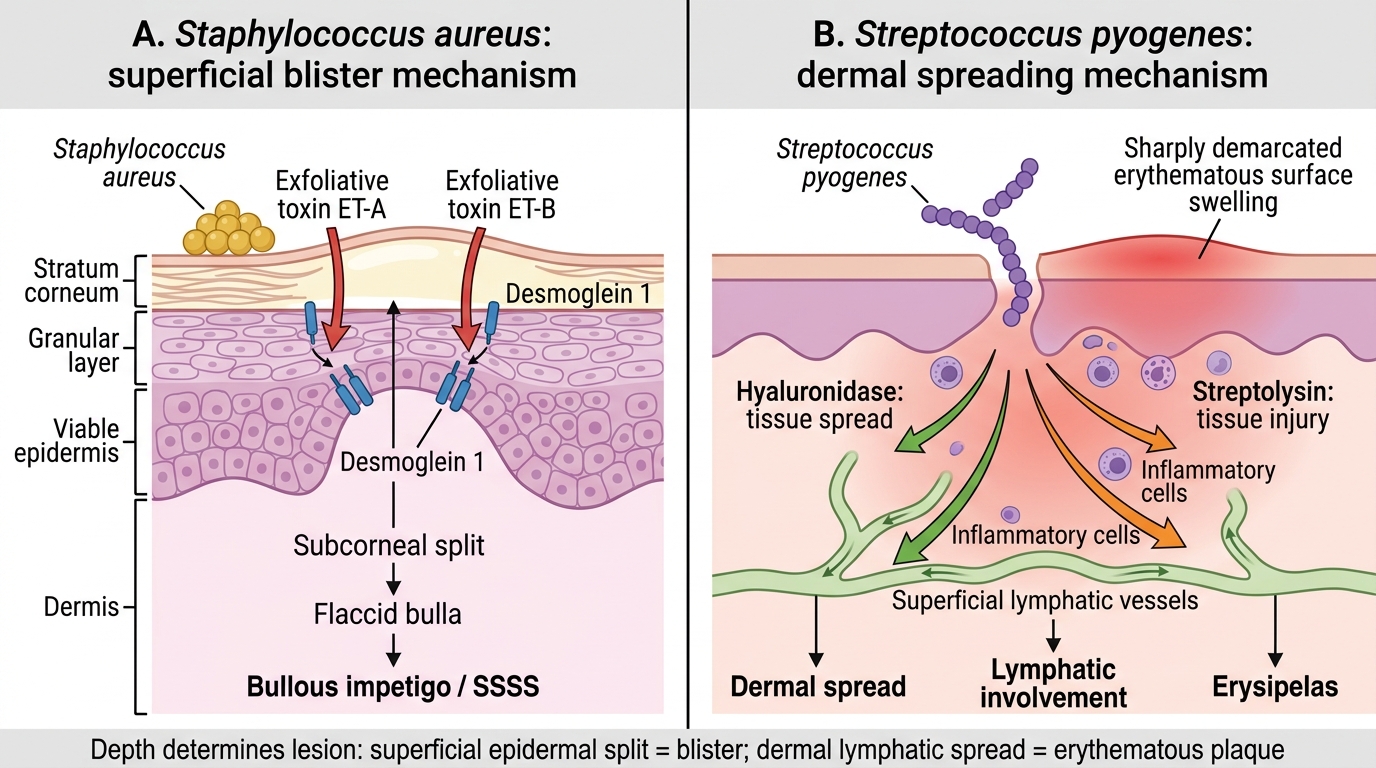
- Exfoliative toxins (ET-A, ET-B) of Staphylococcus aureus cleave desmoglein 1, a desmosomal adhesion protein in the upper epidermis, producing a subcorneal split. Localised toxin action gives bullous impetigo; widespread haematogenous toxin spread in young children gives staphylococcal scalded skin syndrome (SSSS).
- Follicular invasion by Staphylococcus aureus, with coagulase walling off an abscess, produces folliculitis, and when infection extends deeper, the furuncle and (by coalescence) the carbuncle.
- Spreading enzymes of Streptococcus pyogenes — hyaluronidase and streptolysins — let the organism move rapidly through the dermis and lymphatics, producing the sharply-marginated plaque of erysipelas and contributing to cellulitis.
Bacterial Skin Lesions: Toxin Mechanisms and Depth of Spread
The organism plus the host breach plus the depth of invasion together produce the lesion you finally see.
SELF-CHECK
A 5-year-old develops several thin-walled flaccid blisters on the trunk that rupture easily to leave a thin collarette of scale; there is no surrounding erythema and the child is systemically well. Which organism and mechanism best explain this presentation?
A. Streptococcus pyogenes spreading through the dermis via hyaluronidase
B. Staphylococcus aureus producing exfoliative toxin that cleaves desmoglein 1 in the upper epidermis
C. Staphylococcus aureus coagulase walling off a deep follicular abscess
D. Mixed anaerobic invasion of the subcutaneous tissue
Reveal Answer
Answer: B. Staphylococcus aureus producing exfoliative toxin that cleaves desmoglein 1 in the upper epidermis
Flaccid bullae arising in the superficial epidermis are the hallmark of bullous impetigo, caused by Staphylococcus aureus exfoliative toxins (ET-A/ET-B) that cleave desmoglein 1 and produce a subcorneal split. Streptococcal spread produces deeper, spreading erythema (erysipelas/cellulitis), not surface blisters; coagulase-walled abscesses are deep follicular lesions (furuncle), not flaccid bullae.
Clinical Features by Type: Distinguishing Impetigo, Folliculitis, Furuncle, Carbuncle, Erysipelas, Cellulitis, and SSSS
Clinical Patterns of Pyoderma by Depth and Morphology
With morphology and mechanism now established, we can describe each pyoderma type as you will actually meet it in the clinic, attending carefully to the primary lesion, its distribution, the affected age-group, and any systemic features. Diagnosis in pyoderma is overwhelmingly clinical: the combination of the primary lesion, its anatomical site, the patient's age, and the presence or absence of fever and toxicity usually names the disease confidently without needing a swab or any laboratory test. The descriptions below move deliberately from the most superficial conditions to the deepest and most spreading ones, mirroring the depth continuum you have already learned, so that each new type slots neatly into a mental frame you already hold rather than arriving as an isolated fact. As you read, keep asking which organism and which depth each description implies, because that linkage is what makes the list memorable and clinically usable.
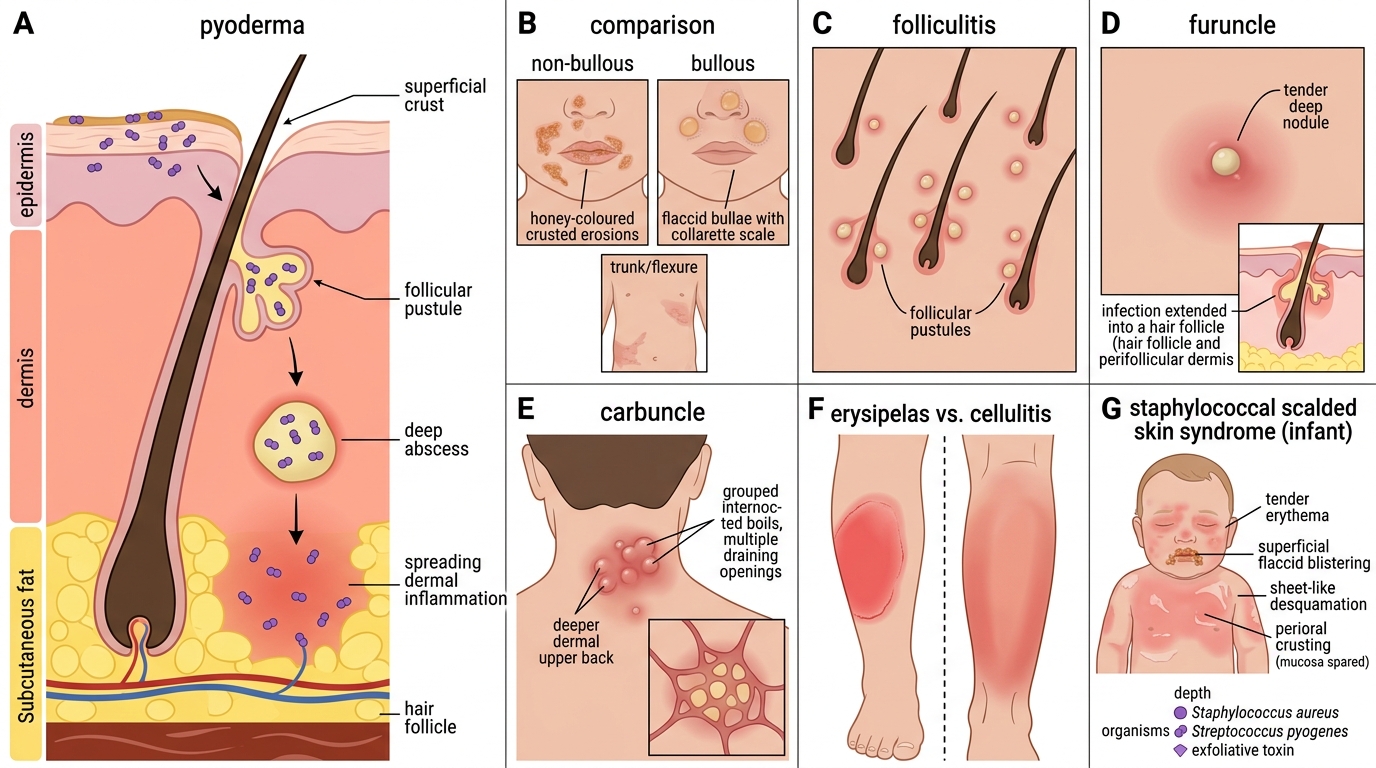
- Impetigo, non-bullous: the commonest pyoderma; honey-coloured crusted erosions, classically peri-oral and peri-nasal in children; caused by Staphylococcus aureus, sometimes with Streptococcus pyogenes; highly contagious; systemically well.
- Impetigo, bullous: flaccid bullae that rupture to a collarette; Staphylococcus aureus exfoliative toxin; trunk and flexures.
- Ecthyma: a deeper, ulcerative impetigo with a thick adherent crust over a punched-out ulcer; heals with scarring; legs of children and debilitated adults.
- Folliculitis: small follicular pustules pierced by a hair; superficial and self-limiting.
- Furuncle (boil): a tender deep follicular nodule with a single pus-point; hair-bearing, friction-prone sites.
- Carbuncle: coalescence of adjacent furuncles into a multi-headed abscess; nape of neck, back; common in diabetics; often with fever and malaise.
- Erysipelas: Streptococcus pyogenes infection of the upper dermis and lymphatics; a sharply-demarcated, raised, red, hot plaque on the face or leg, with fever.
- Cellulitis: deeper infection of the dermis and subcutis; ill-defined, non-raised spreading erythema, warmth, tenderness, often with fever.
- Staphylococcal scalded skin syndrome (SSSS): predominantly in young children; widespread tender erythema with superficial peeling from haematogenous exfoliative toxin; the child is unwell and needs admission.
The single most useful bedside discriminator between the two spreading infections is the margin: erysipelas is sharply demarcated and raised, whereas cellulitis is ill-defined and flat.