Page 5 of 12
DR15.3 | Pyoderma Surgical Referral Decisions — SDL Guide
Learning Objectives
- Recognise the clinical features of pyoderma that signal a need for surgical, rather than purely medical, management
- Explain the physiological reasons some pyodermas cannot be cured with antibiotics alone
- Identify the clinical features of a fluctuant abscess (furuncle/carbuncle) that indicate incision and drainage
- Recognise necrotising soft-tissue infection as a surgical emergency and distinguish it from cellulitis
- Make and justify the surgical-referral decision, classifying its urgency and communicating it appropriately
INSTRUCTIONS
Most pyoderma is managed entirely by the physician with topical or systemic antibiotics. A small but critically important subset, however, will not resolve — and may rapidly worsen — unless a surgeon intervenes. The clinician who can recognise the fluctuant abscess that needs draining, and above all the necrotising infection that needs emergency debridement, prevents avoidable morbidity and death. This SDL builds the decision layer on top of the diagnostic and prescribing skills of the companion module: it teaches you when antibiotics are not enough, why that is so, and how urgently to act. Recognising the need for surgical referral in pyoderma is the competency, and timely recognition of a surgical emergency is its highest-stakes application.
References
- Sacchidanand S, et al. IADVL Textbook of Dermatology, 4th ed. Ch: Bacterial Infections of the Skin (Pyodermas) (textbook)
- Khanna N. Illustrated Synopsis of Dermatology and Sexually Transmitted Diseases, 6th ed. Ch: Bacterial Infections (textbook)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
A 55-year-old diabetic man is seen with a 'red leg' diagnosed as cellulitis two days ago and started on oral antibiotics. Today he is worse: the redness has marched up his calf, he is febrile and confused, and — most strikingly — he is screaming in pain that seems far out of proportion to the modest skin changes you can see. A junior colleague suggests simply changing the antibiotic. But this is the picture of a necrotising soft-tissue infection, and no antibiotic alone will save this leg or this life — he needs a surgeon, now. Knowing when a skin infection has crossed from 'treat medically' to 'refer for surgery', and how urgently, is the skill this module builds.
WHY THIS MATTERS
For most pyoderma, the right answer is a prescription. But the clinician's most dangerous error is to keep prescribing when the patient has crossed the line into surgical territory. Two situations matter every day in practice: the fluctuant abscess — a furuncle or carbuncle that has collected pus and will not resolve until it is drained — and the necrotising soft-tissue infection, where delay of even a few hours costs tissue and lives. Recognising these, and referring at the right urgency, is a core safety competency for every doctor, not just dermatologists and surgeons. You will meet these patients in casualty, in the ward, and in the clinic, and your speed of recognition will directly determine their outcome. This is why the referral decision deserves a module of its own.
RECALL
Carry forward three things you already know. From the companion SDL on pyoderma presentation: you can now identify a furuncle (a deep follicular abscess with a pus-point), a carbuncle (coalescing furuncles, common in diabetics), and cellulitis (ill-defined, deep, spreading erythema). From Anatomy: the skin overlies subcutaneous fat, which overlies the deep fascia, and infection can track along fascial planes far beyond the visible skin change. From Pathology: the systemic inflammatory response — fever, tachycardia, hypotension, altered mental state — signals that a local infection has become a systemic threat (sepsis). Hold these three threads — the abscess you can drain, the fascial plane along which infection spreads, and the systemic signs of danger — as we work through when a pyoderma needs a surgeon.
When Skin Infection Signals More: The Clinical Presentation That Prompts Surgical Thinking
Clinical Red Flags in Pyoderma Requiring Surgical Thinking
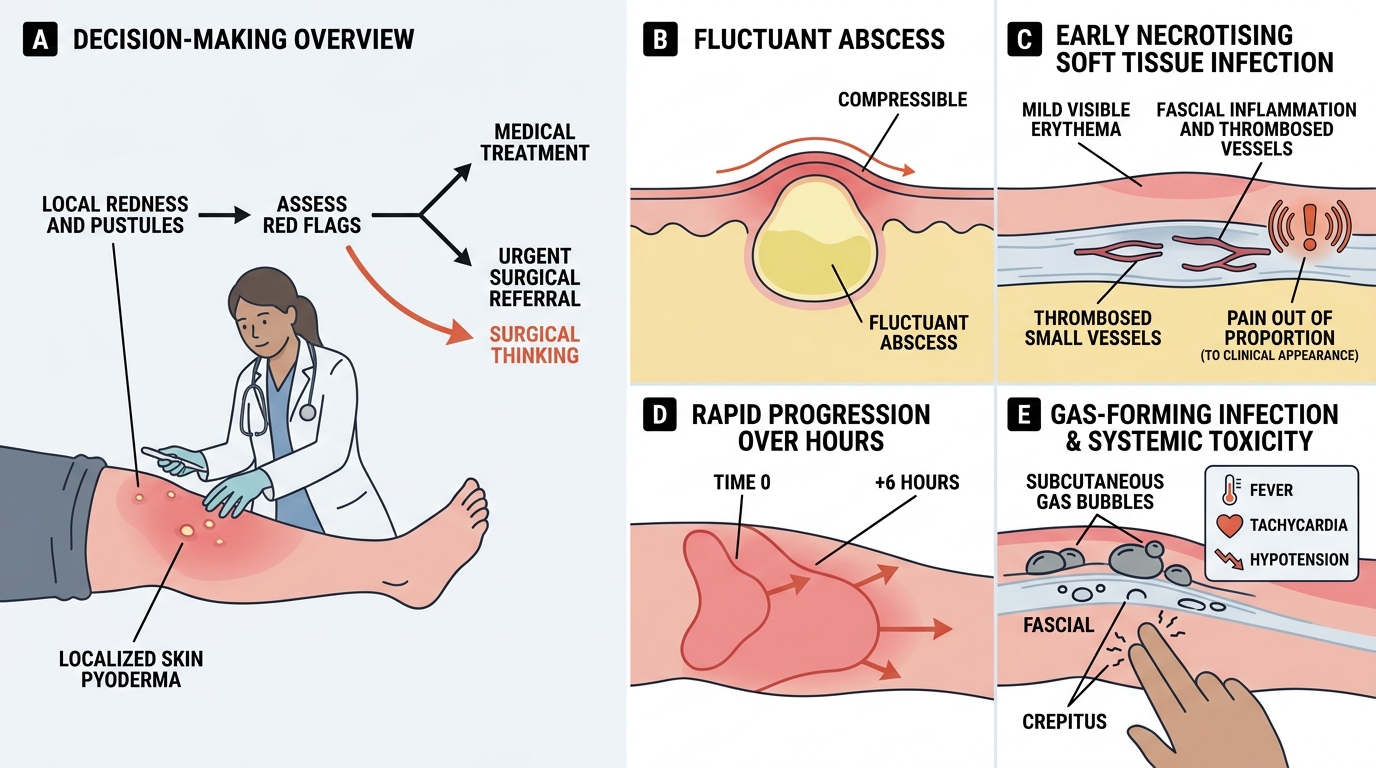
The first skill in surgical referral is recognising, from the clinical presentation alone, the moment a skin infection stops being something you treat with drugs and becomes something a surgeon must see. Most pyoderma announces itself as a localised, medically tractable problem; but a handful of clinical features should make the experienced clinician pause and shift their entire frame of thinking from 'which antibiotic' to 'does this patient need an operation'. Training yourself to notice these features early — before the textbook late signs of skin necrosis appear — is what separates timely, life-saving referral from a fatal delay. The cues are deliberately simple to remember because they must be applied at speed, often by a junior doctor seeing the patient first, and the cost of missing them is measured in lost limbs and lost lives.
The features that should prompt surgical thinking are:
- Fluctuance — a soft, compressible, pus-filled swelling (a collected abscess that will not resolve on antibiotics alone).
- Pain out of proportion to the visible skin signs — a hallmark early warning of necrotising infection.
- Rapid progression of erythema or swelling over hours.
- Crepitus — a crackling sensation under the skin from gas-forming organisms.
- Systemic toxicity — high fever, tachycardia, hypotension, or altered mental state.
Any of these should stop the reflex to simply prescribe, and start the question: does this patient need a surgeon, and how urgently?
Pathophysiology: Why Some Pyodermas Cannot Be Cured with Antibiotics Alone
Why Some Pyodermas Need Source Control
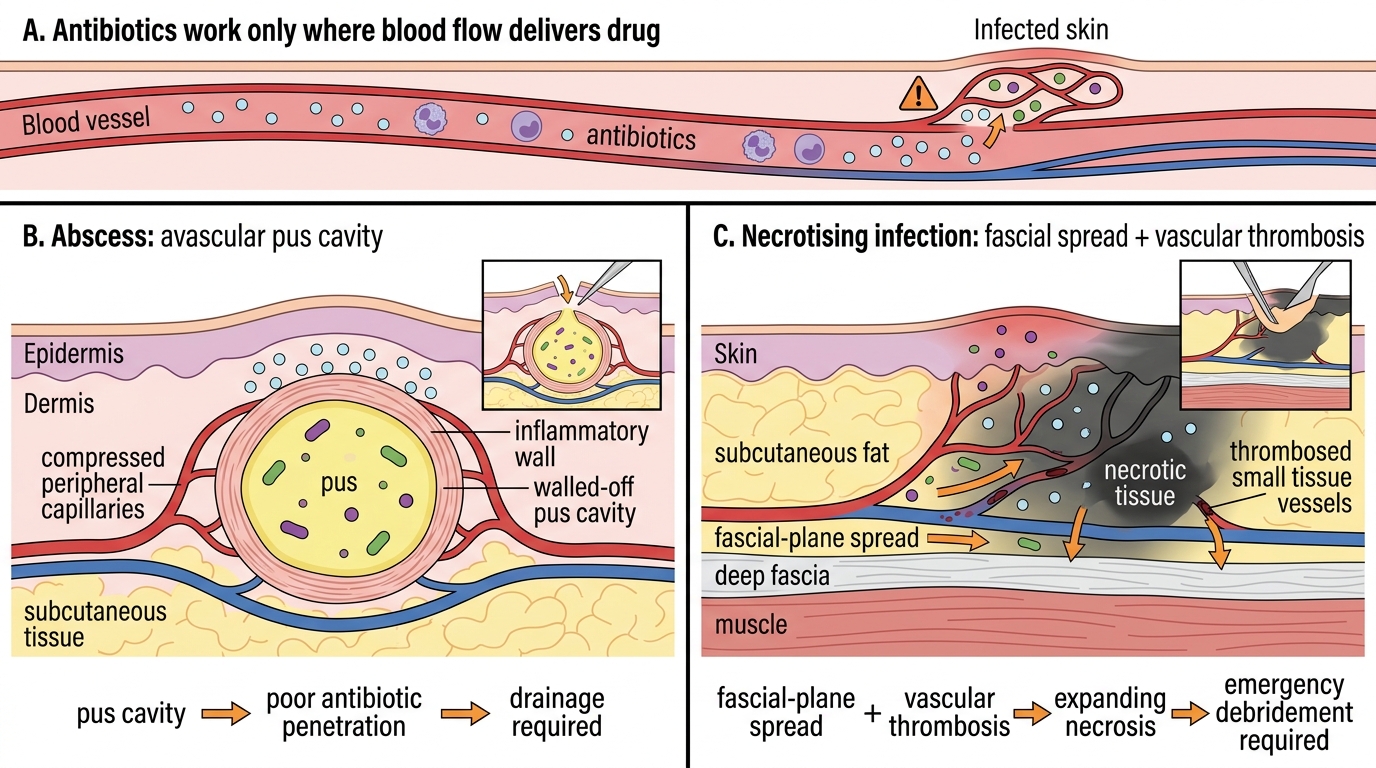
To refer confidently, you must understand why certain pyodermas are physiologically beyond the reach of antibiotics, because that understanding turns a memorised rule into clinical judgement. Antibiotics work only where the drug can reach the bacteria in adequate concentration and where the host's own defences can finish the job. Two situations defeat this. In a fluctuant abscess, pus collects in an avascular cavity walled off from the bloodstream; systemically administered antibiotics simply cannot penetrate the dead, pus-filled core in useful concentration, so the collection persists or enlarges until it is physically drained. In a necrotising soft-tissue infection, the problem is different but equally beyond antibiotics: bacteria spread explosively along fascial planes, thrombosing the small vessels that would have delivered the drug and producing rapidly expanding tissue death that outpaces both the antibiotic and the immune system. Removing the dead tissue surgically is the only way to halt it.
The two mechanisms, side by side:
- Abscess (source control by drainage): avascular pus cavity → poor antibiotic penetration → drainage required to remove the bacterial load.
- Necrotising infection (source control by debridement): fascial-plane spread + vascular thrombosis → expanding necrosis the drug cannot reach → emergency removal of dead tissue required.
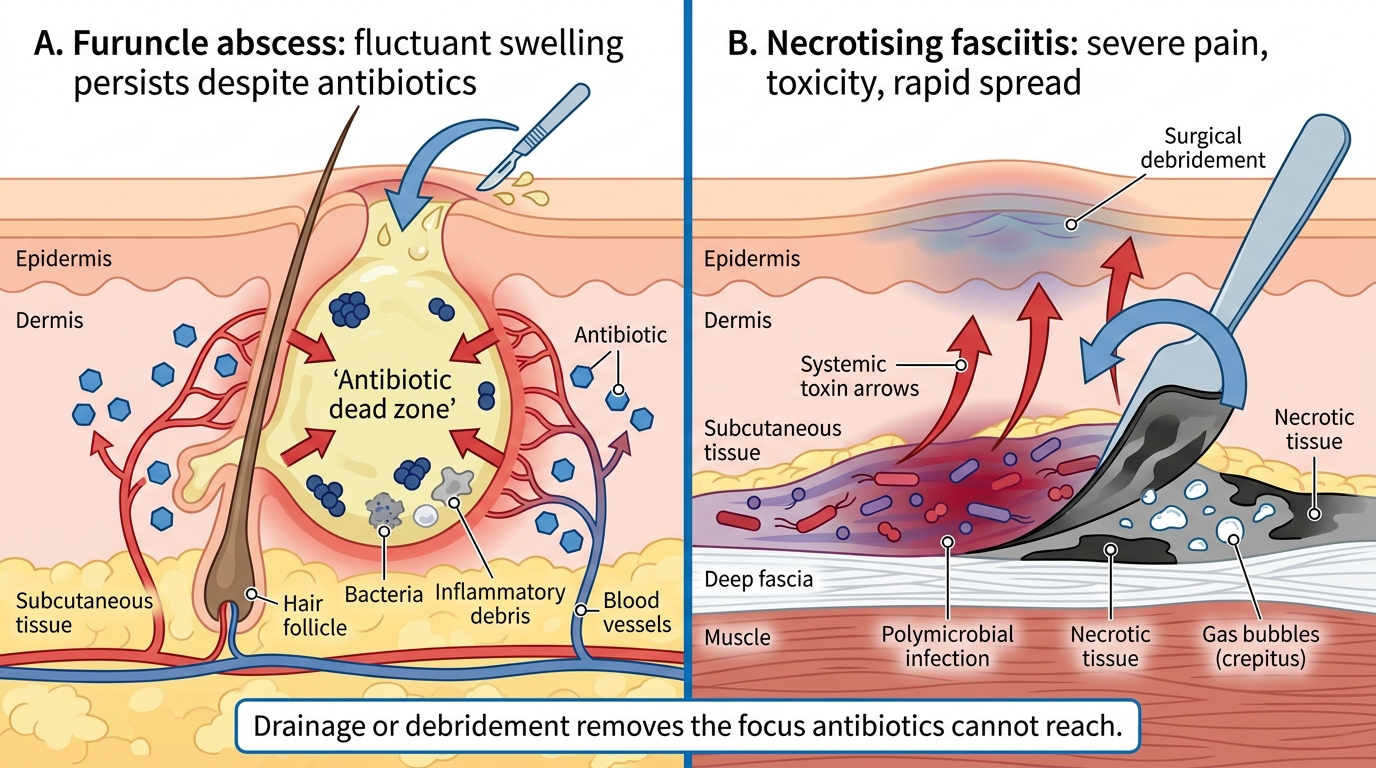
Why Surgery Is Needed in Abscess and Necrotising Fasciitis
In both, the surgical act — drainage or debridement — achieves what no antibiotic can: it removes the focus the drug cannot reach.
SELF-CHECK
A patient has a 3 cm tender, fluctuant swelling on the back that has not improved after 48 hours of appropriate oral antibiotics. Which physiological reason best explains why the antibiotic alone has failed?
A. The organism is intrinsically resistant to all oral antibiotics
B. Pus has collected in an avascular cavity that systemic antibiotics cannot penetrate in adequate concentration, so the collection must be physically drained
C. Oral antibiotics are never effective for any skin infection
D. The patient has not taken the antibiotic for long enough and simply needs more time
Reveal Answer
Answer: B. Pus has collected in an avascular cavity that systemic antibiotics cannot penetrate in adequate concentration, so the collection must be physically drained
A fluctuant swelling indicates a collected abscess. The pus sits in an avascular cavity walled off from the circulation, so a systemically administered antibiotic cannot reach it in useful concentration regardless of the organism's sensitivity. Source control by incision and drainage is required; antibiotics are an adjunct, not a substitute, for draining a fluctuant abscess.
Clinical Features and Diagnosis of Surgically Relevant Pyoderma
Bedside Diagnosis of Surgically Relevant Pyoderma
Having understood why surgery is sometimes necessary, you must be able to diagnose, at the bedside, the two surgically relevant pictures: the fluctuant abscess and the necrotising soft-tissue infection. These two differ enormously in urgency, and conflating them — or, worse, mistaking early necrotising infection for ordinary cellulitis — is the central diagnostic hazard of this topic. The fluctuant abscess is usually obvious and can be managed in a controlled, same-day fashion; the necrotising infection is treacherous precisely because in its early hours it can look deceptively mild on the skin surface while catastrophe unfolds in the deeper tissues. The single most important habit to cultivate is to take seriously a patient whose pain is far greater than the visible skin signs would explain, because that discordance is often the only early clue you will get before the dramatic late signs appear.
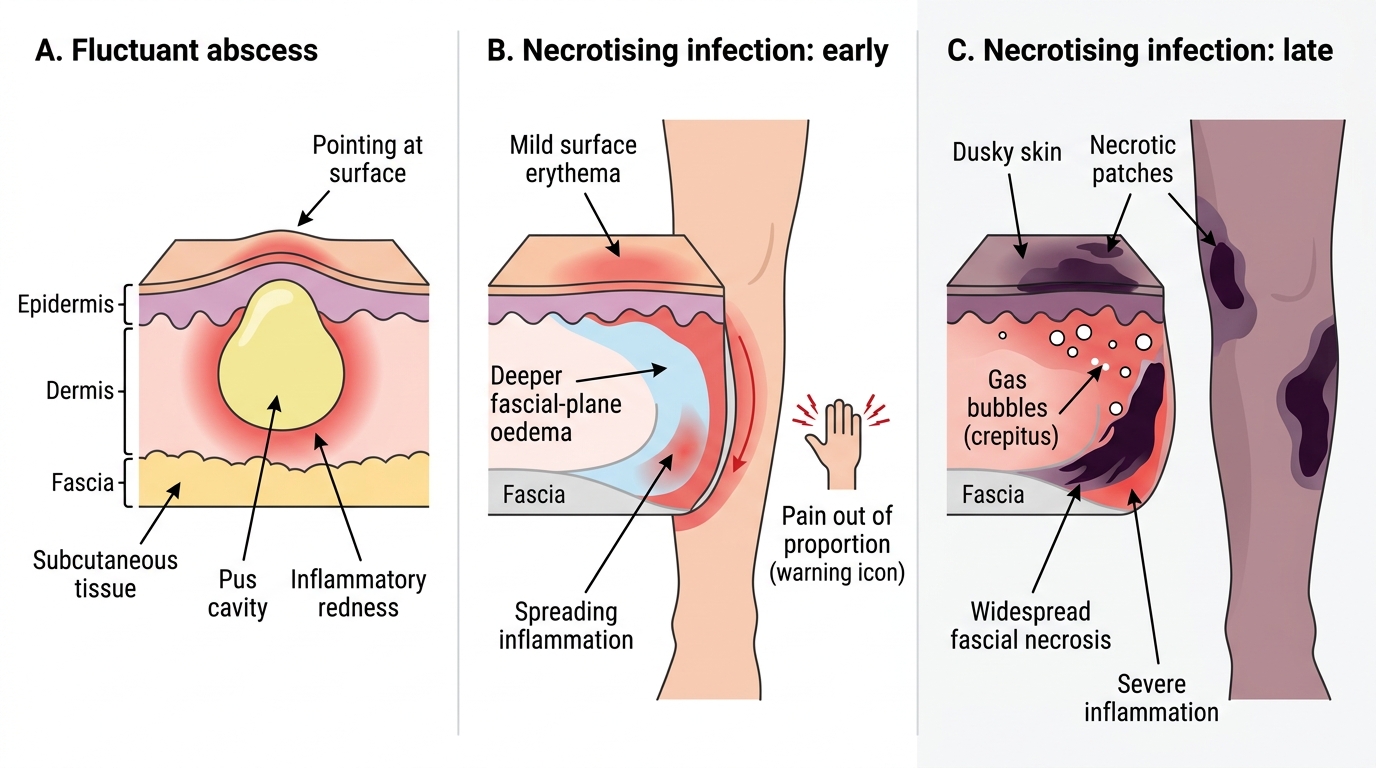
The diagnostic features of each:
- Fluctuant abscess (furuncle / carbuncle): a localised, tender, fluctuant swelling, often pointing with visible pus, sometimes with surrounding cellulitis; the patient is usually not severely toxic.
- Necrotising soft-tissue infection — early: severe pain out of proportion to visible signs; oedema and tenderness extending beyond the area of erythema; the patient may already feel systemically unwell.
- Necrotising soft-tissue infection — late: crepitus, dusky or frankly necrotic skin, haemorrhagic bullae, anaesthesia of the overlying skin, and systemic sepsis (fever, tachycardia, hypotension, confusion).
The early picture, not the late one, is where lives are saved — train yourself to act on the discordant pain before the skin turns dusky.