Page 16 of 35
DR10.4 | Genital Ulcer Examination With Privacy and Chaperone — SDL Guide
Learning Objectives
- Identify the clinical indications for performing a genital examination in a patient presenting with genital ulcer disease (GUD).
- Demonstrate the patient-rights framework — informed consent, privacy, confidentiality, and a documented chaperone — before and during genital examination.
- Perform a systematic genital and regional lymph-node examination with correct technique and infection-control practice.
- Interpret ulcer morphology and lymph-node findings to triage the patient into the appropriate NACO syndromic category.
INSTRUCTIONS
A genital ulcer is one of the most emotionally charged complaints a patient can bring to a clinic, and the way you conduct the examination determines whether the patient trusts you, returns for follow-up, and discloses their sexual history honestly. This skills module teaches you to examine a patient with genital ulcer disease the right way — with consent, privacy, a chaperone, and a systematic technique — so that you neither miss a treatable, transmissible infection nor humiliate a vulnerable person. Mastering this examination is the foundation on which every syndromic-management decision in the rest of this cluster rests.
References
- NACO National Guidelines on Prevention, Management and Control of STI/RTI (Syndromic Case Management) (textbook)
- Neena Khanna, Illustrated Synopsis of Dermatology & Sexually Transmitted Diseases, STD section (textbook)
- IADVL Textbook of Dermatology, chapter on Sexually Transmitted Infections (textbook)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
A 24-year-old labourer comes to the skin OPD, sits at the edge of the chair, and will not make eye contact. After ten minutes he whispers that he has a sore on his private parts. The corridor outside is full, the examination cubicle has no curtain, and a junior nurse keeps walking in and out. You have two choices: rush the examination in a half-open room and send him away, or pause, secure privacy, call a chaperone, take consent, and examine him properly. The first path means he will never come back — and a single painless indurated ulcer that was actually primary syphilis will go untreated and onward-transmitted. The second path is the entire content of this module. How you examine a genital ulcer is as clinically decisive as what you find.
WHY THIS MATTERS
Genital ulcer disease is a syndromic gateway: behind every ulcer sits a treatable, transmissible, and sometimes HIV-facilitating infection — syphilis, chancroid, herpes, lymphogranuloma venereum, or donovanosis. As an intern and later as a medical officer at a primary health centre, you will be the first and often only clinician these patients meet. A genital examination conducted without consent or a chaperone is both an ethical breach and a medico-legal liability; one conducted carelessly misses the morphological clues that drive correct syndromic treatment. The competency DR10.4 explicitly demands that you examine 'ensuring privacy, confidentiality in presence of a chaperone' — this is not optional courtesy, it is the standard of care.
RECALL
Before this session, recall from Year-1 Anatomy the surface anatomy of the external genitalia in both sexes and the lymphatic drainage of the perineum and genitalia into the superficial and deep inguinal lymph node groups — these are the nodes you will palpate. Recall also from your foundation course on professional ethics the four principles of informed consent (capacity, disclosure, understanding, voluntariness) and the doctor's duty of confidentiality. You will combine this anatomical and ethical knowledge with the syndromic-management framework introduced later in this cluster.
Patient Rights, Consent, Privacy, and Chaperone Policy
Patient Rights and Privacy Framework Before Genital Examination
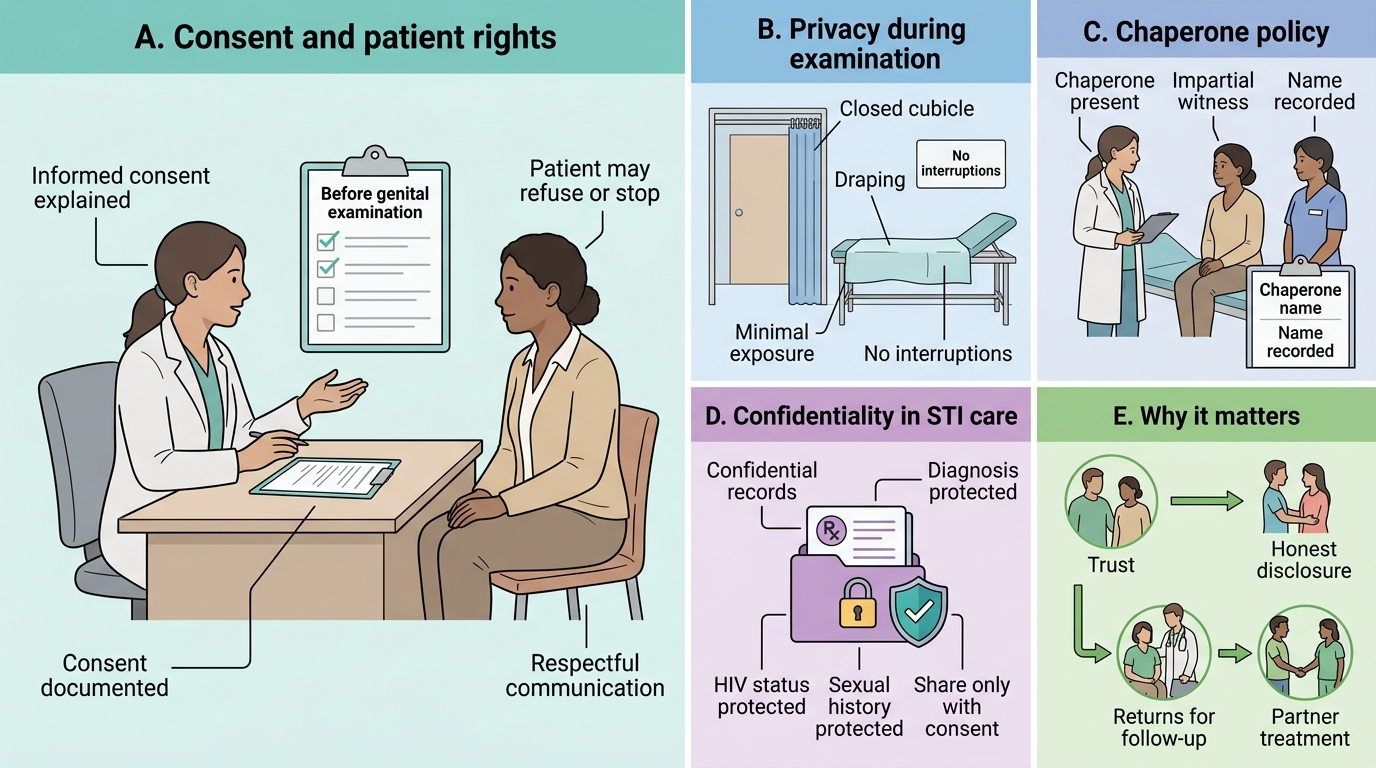
The single most important determinant of a successful genital examination is established before you touch the patient: a framework of rights that protects the patient and the examiner equally. Begin by obtaining informed consent — explain in language the patient understands what you need to examine, why, and what it will involve, and document that consent was given. The patient retains the right to refuse or to stop at any point. A chaperone — ideally a same-sex nurse or health worker acting as an impartial witness — must be present for every genital examination; record the chaperone's name. Privacy means a curtained or closed cubicle, draping that exposes only the area being examined, and no interruptions. Confidentiality means that nothing the patient discloses — diagnosis, sexual history, or HIV status — is shared without their consent; this is the cornerstone of trust in STI care. These four elements are not bureaucratic add-ons: a patient who feels respected discloses honestly, returns for follow-up, and brings their partner for treatment.
Key elements to secure before examination:
- Informed consent, explained and documented
- A chaperone present and named in the record
- Privacy: closed cubicle, draping, minimal exposure, no interruptions
- Confidentiality: no disclosure without the patient's consent
- The patient's right to refuse or stop at any stage
Materials, Positioning, and Pre-Examination Infection Control
Preparedness and Infection Control for Genital Examination
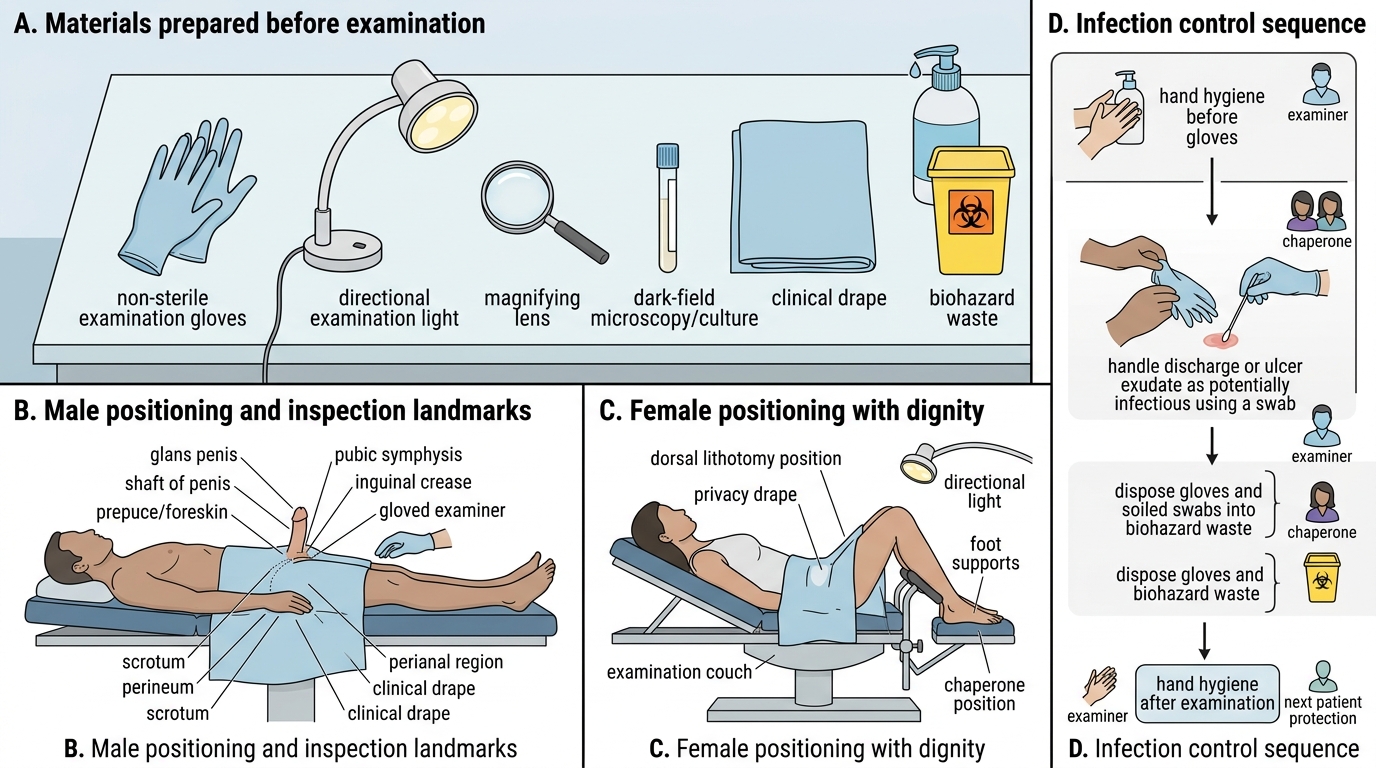
With rights secured, the principle that governs the next step is preparedness: a genital examination interrupted to fetch gloves or a light loses both efficiency and the patient's confidence. Assemble your materials before you begin — non-sterile examination gloves, a good directional light source, a magnifying lens if available, and swabs for dark-field microscopy or culture where the facility supports it. Position the patient comfortably and with dignity: a male patient is usually examined supine or standing, while a female patient is positioned in the dorsal lithotomy position with appropriate draping. Infection control frames the entire encounter — perform hand hygiene before donning gloves and again after the examination (the WHO 'five moments' apply), handle any discharge or ulcer exudate as potentially infectious, and dispose of gloves and soiled swabs into the correct biohazard waste stream. These steps protect you, the chaperone, and the next patient.
Systematic Male Genital Examination
Materials and infection-control checklist:
- Non-sterile gloves, directional light, magnifying lens
- Swabs for dark-field/culture where available
- Patient positioned with dignity and draped
- Hand hygiene before and after; soiled material into biohazard waste
SELF-CHECK
During a genital examination of a male patient with a genital ulcer, who should be present in the cubicle as an impartial witness, and what must be done about it?
A. No one — the doctor-patient relationship is private and a third party breaches confidentiality
B. A chaperone (ideally a same-sex nurse or health worker), whose name is documented in the record
C. A senior consultant, who must personally re-examine the patient
D. Any available person from the corridor, no documentation needed
Reveal Answer
Answer: B. A chaperone (ideally a same-sex nurse or health worker), whose name is documented in the record
A chaperone — an impartial witness, ideally a same-sex nurse or health worker — must be present for every genital examination, and their name must be documented. This protects both patient and examiner and is explicitly required by competency DR10.4. Confidentiality is preserved because the chaperone is bound by the same duty; it does not require absence of a witness.
Systematic Genital Examination Technique
Systematic Genital Examination Technique
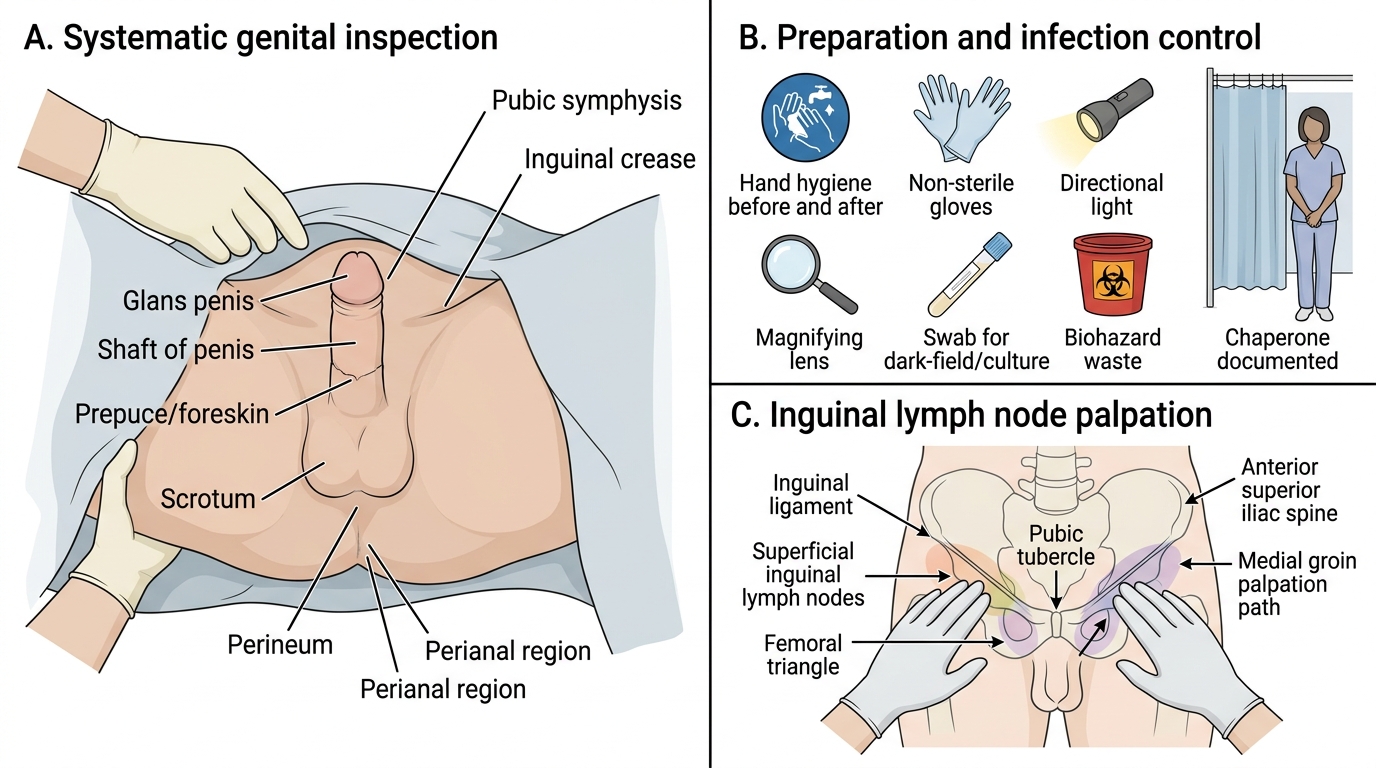
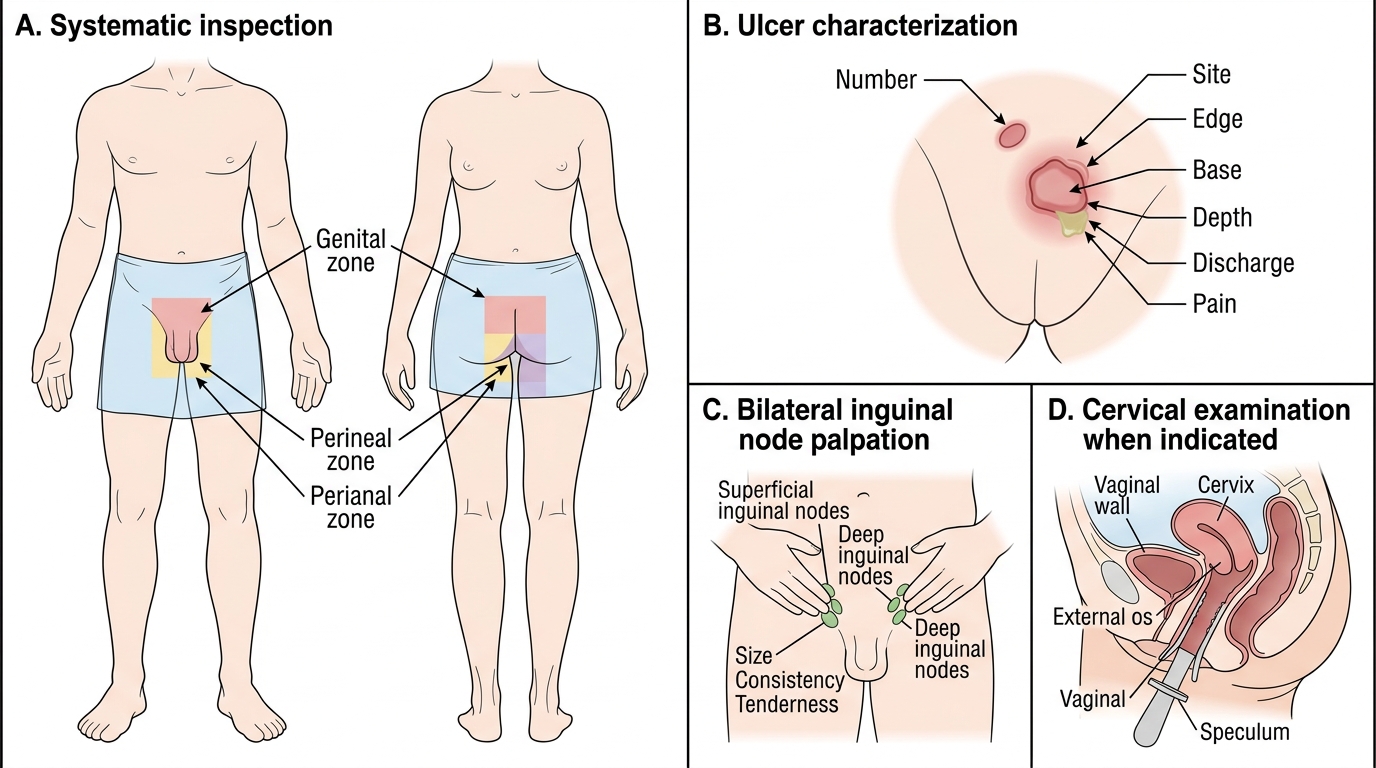
A systematic technique ensures that no lesion is missed and that the findings you record are reproducible and clinically interpretable. Expose the minimum area necessary and inspect the entire genital region — in the male this means the glans, prepuce (retracted gently), coronal sulcus, shaft, scrotum, and the perineum and perianal area; in the female it means the vulva, labia, vaginal introitus, perineum, and perianal region, with a per-speculum examination of the cervix where indicated. For every ulcer you find, characterise it methodically: number (single or multiple), site, edge (indurated, undermined, or clean), base (clean, purulent, or beefy-red), depth, presence of discharge, and crucially whether it is painful or painless. Then palpate the regional inguinal lymph nodes bilaterally, noting their size, consistency, tenderness, matting, and any fluctuance. Throughout, narrate gently to the patient what you are doing, and stop if they ask you to.
Systematic sequence:
1. Inspect the whole genital, perineal, and perianal region — minimum exposure
2. For each ulcer: number, site, edge, base, depth, discharge, pain
3. Palpate both inguinal node groups: size, consistency, tenderness, matting, fluctuance
4. Per-speculum cervical examination in females where indicated