Page 29 of 35
DR10.11 | Genital Wart Diagnosis Treatment and Education — SDL Guide (Part 2)
Investigations and Oncogenic Risk Assessment
HPV Investigation and Oncogenic Risk Assessment
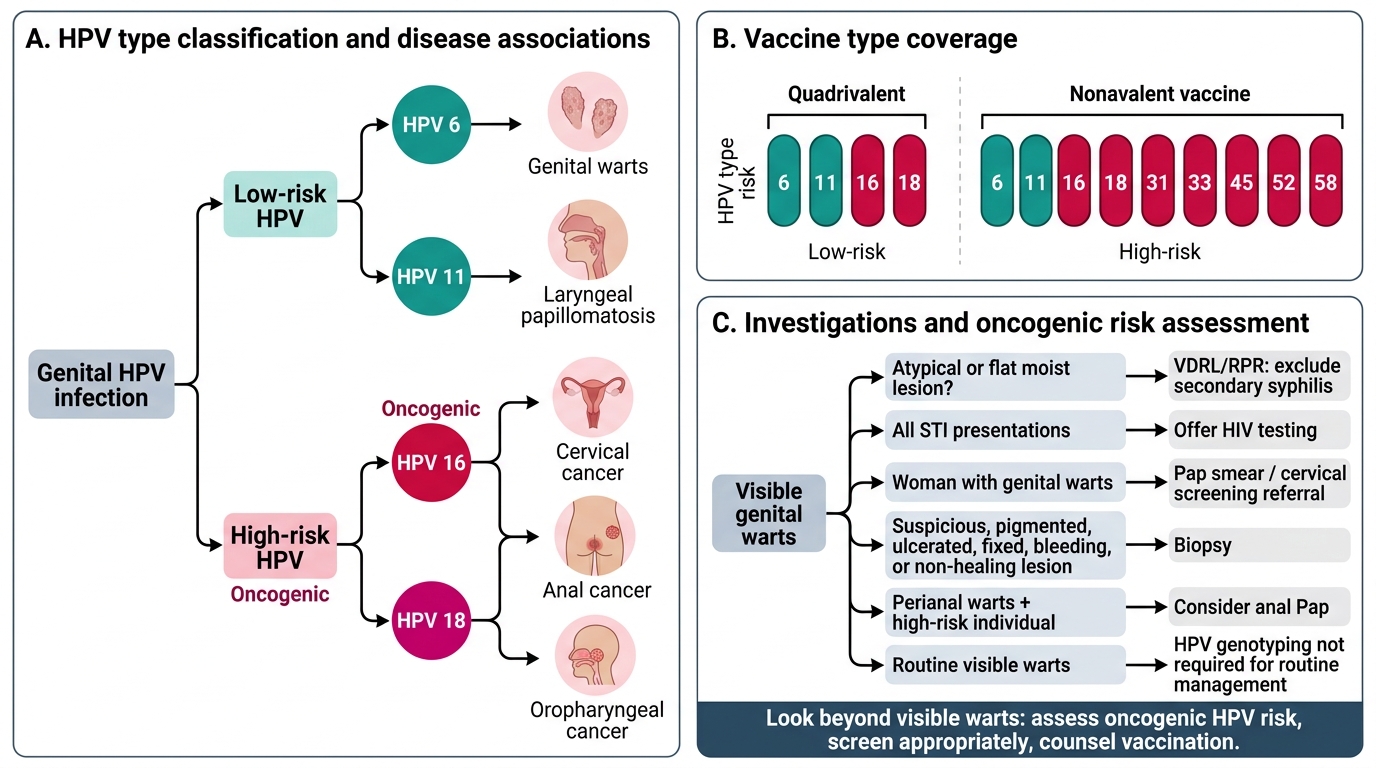
Investigations in genital warts serve two purposes: excluding the dangerous mimics and assessing the broader oncogenic risk that HPV carries. Because condylomata lata can masquerade as warts, VDRL/RPR to exclude secondary syphilis is appropriate whenever the morphology is atypical or flat-and-moist. As with every STI presentation, offer HIV testing. For women with genital warts, arrange cervical screening (Pap smear) referral, since exposure to genital HPV — including possible concurrent high-risk types — raises the relevance of screening for cervical dysplasia. HPV genotyping can identify high-risk types but is not required for routine clinical management of visible warts. A biopsy is reserved for suspicious lesions, and an anal Pap may be considered for perianal warts in high-risk individuals. The point of this step is to look past the warts themselves to the person's overall oncogenic-HPV risk and to act on it through screening and vaccination counselling.

HPV Type Classification and Vaccine Coverage
Investigation pointers:
- VDRL/RPR to exclude condylomata lata (secondary syphilis); offer HIV testing
- Refer women for cervical (Pap) screening
- HPV genotyping optional; biopsy if suspicious; anal Pap for high-risk perianal warts
SELF-CHECK
A patient has flat, moist, broad-based grey lesions in the genital area that you initially suspect are warts. Which single investigation is most important to avoid missing a serious diagnosis, and what would it reveal?
A. A fasting blood glucose, which would reveal diabetes
B. VDRL/RPR serology, which would be positive in condylomata lata of secondary syphilis
C. A urine culture, which would reveal a urinary tract infection
D. No investigation is needed; treat as warts
Reveal Answer
Answer: B. VDRL/RPR serology, which would be positive in condylomata lata of secondary syphilis
Flat, moist, broad-based lesions can be condylomata lata of secondary syphilis rather than HPV warts. VDRL/RPR serology is the key investigation — it is positive in secondary syphilis, which requires entirely different management (penicillin) and signals a systemic infection. Mistaking condylomata lata for warts is a classic and serious error.
Treatment Options and Patient Education
Genital Warts: Treatment Options and Patient Education
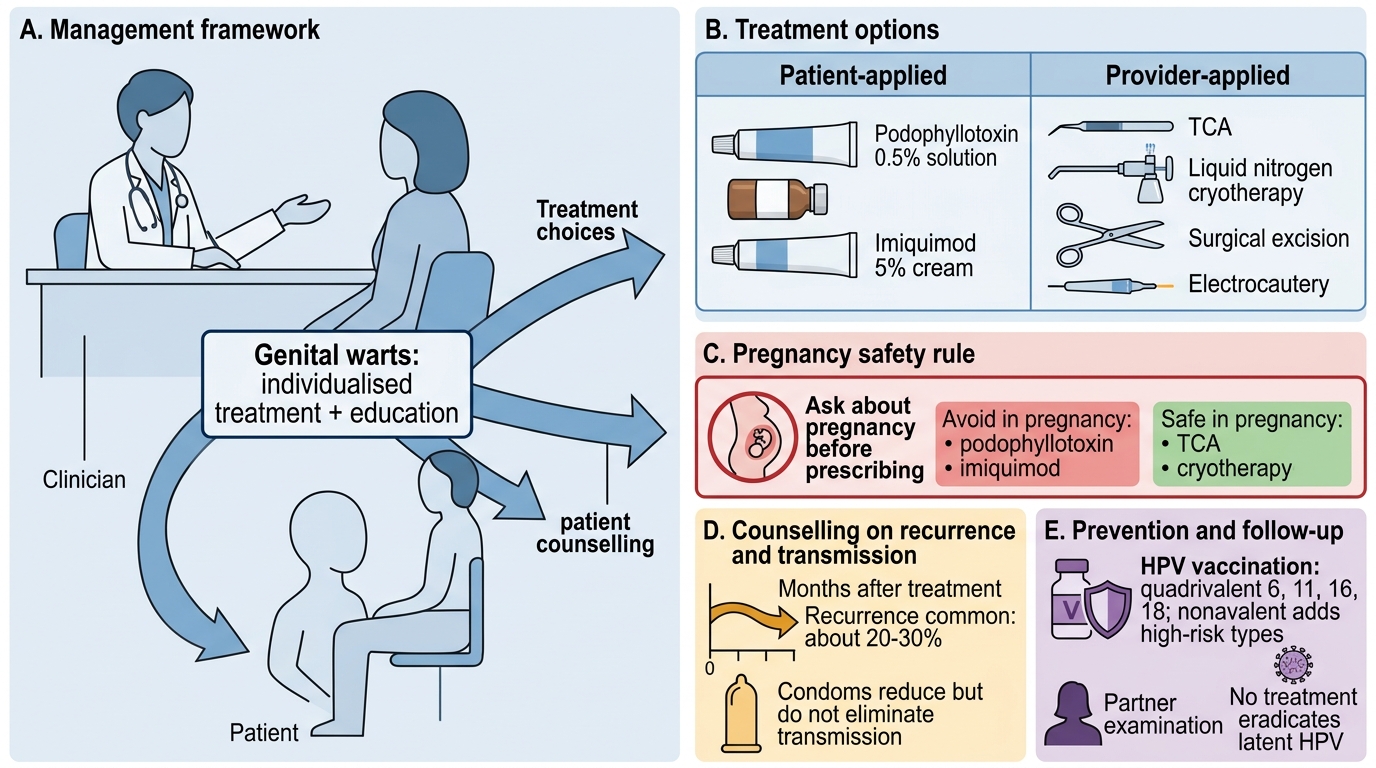
Management of genital warts combines an individualised choice of treatment with the education that gives the consultation its lasting value, and a key safety rule governs the choice. Treatments fall into patient-applied and provider-applied groups. Patient-applied options include podophyllotoxin (0.5% solution, applied in cycles) — effective for accessible warts but contraindicated in pregnancy because it is teratogenic — and imiquimod (5% cream, an immune-response modifier applied over several weeks, also avoided in pregnancy). Provider-applied options include trichloroacetic acid (TCA) and cryotherapy with liquid nitrogen, both of which are safe in pregnancy and suitable for many sites, and surgical excision or electrocautery for large or resistant warts. Always ask about pregnancy before prescribing podophyllotoxin or imiquimod. Counsel the patient that recurrence is common (roughly a fifth to a third within months) so that treatment failure is not interpreted as your error; advise condom use (which reduces but does not eliminate transmission); recommend HPV vaccination for prevention (quadrivalent covers 6, 11, 16, 18; nonavalent adds further high-risk types) — per current national immunisation guidance; arrange cervical screening for women and partner examination; and explain that no treatment eradicates latent HPV.
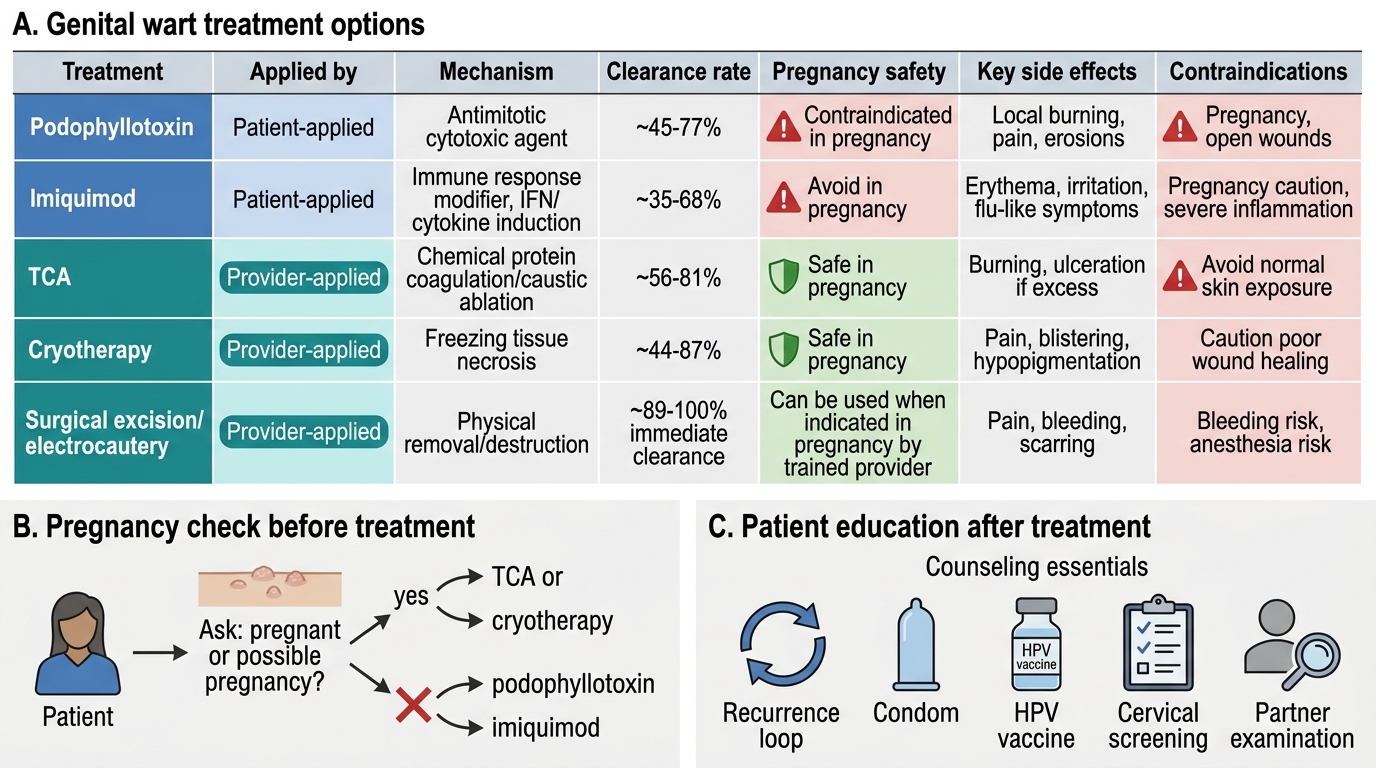
Genital Wart Treatment Options and Pregnancy Safety
Treatment and education essentials:
- Patient-applied: podophyllotoxin (contraindicated in pregnancy), imiquimod (avoid in pregnancy)
- Provider-applied: TCA, cryotherapy (both safe in pregnancy), surgical excision/electrocautery for large/resistant
- Always ask about pregnancy before podophyllotoxin/imiquimod
- Educate: recurrence common, condom use, HPV vaccination, cervical screening, partner examination
SELF-CHECK
A pregnant woman presents with genital warts. Which treatment choice is appropriate, and which must be avoided?
A. Use podophyllotoxin freely; it is safe in pregnancy
B. Avoid podophyllotoxin and imiquimod; use a provider-applied option such as TCA or cryotherapy, which are safe in pregnancy
C. Withhold all treatment until after delivery in every case
D. Use oral antibiotics, which clear HPV warts
Reveal Answer
Answer: B. Avoid podophyllotoxin and imiquimod; use a provider-applied option such as TCA or cryotherapy, which are safe in pregnancy
Podophyllotoxin is contraindicated in pregnancy (teratogenic), and imiquimod is also avoided. Provider-applied options such as trichloroacetic acid (TCA) and cryotherapy are safe in pregnancy and are the appropriate choice. Always ask about pregnancy before prescribing patient-applied podophyllotoxin or imiquimod.
Self-Assessment: Genital Wart Recognition and Management
Genital Wart Recognition and Management Self-Check
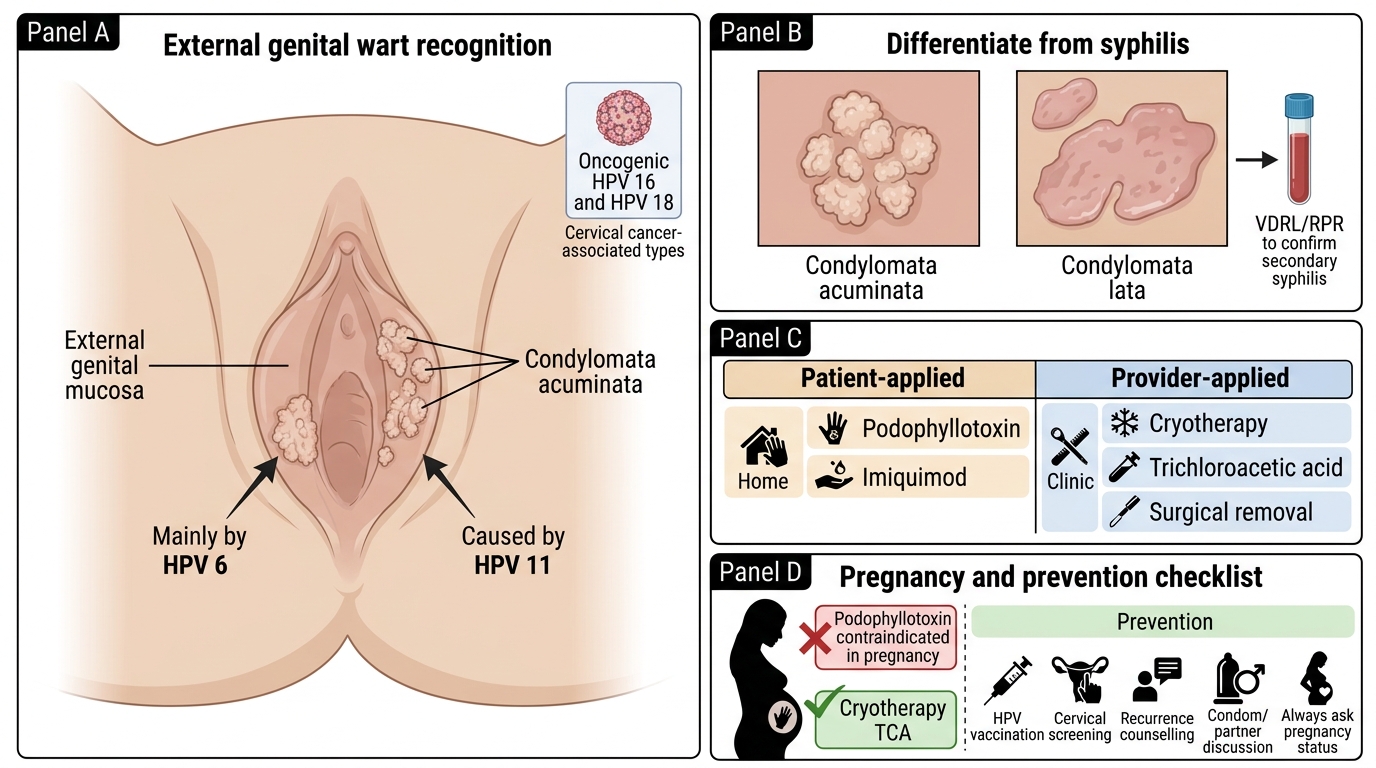
Before you finish, assess your own grasp of this condition, because genital warts is a presentation where the diagnosis is usually easy but the surrounding decisions — excluding syphilis, choosing a pregnancy-safe treatment, and seizing the prevention opportunity — are where care succeeds or fails. Work through the self-check below as if a patient were in front of you, naming the HPV types, the key differential test, the treatment contraindication, and the education points each time. Give particular attention to the two ideas most often dropped under pressure: that flat moist lesions may be condylomata lata of secondary syphilis (do the VDRL), and that podophyllotoxin is contraindicated in pregnancy (always ask). Where any answer feels uncertain, revisit the relevant section and rehearse it until the reasoning is automatic, because in a real consultation you will rely on whatever you have made second nature. Treat each gap as a cue for focused revision rather than a reason for concern.
Self-check questions:
- Which HPV types cause most genital warts, and which are the main oncogenic types?
- How do you differentiate condylomata acuminata from condylomata lata, and what test confirms it?
- Which treatments are patient-applied and which are provider-applied?
- Which treatment is contraindicated in pregnancy, and which are safe?
- What key education points (vaccination, cervical screening, recurrence, partner) belong in this consultation?
CLINICAL PEARL
Two safety reflexes will keep you out of trouble with genital warts. First, whenever a 'wart' looks flat, moist, and broad-based, think condylomata lata and send a VDRL — mistaking secondary syphilis for a benign wart is a classic and consequential error. Second, before you ever hand a patient podophyllotoxin or imiquimod, ask about pregnancy, because podophyllotoxin is teratogenic and the pregnancy-safe choice is a provider-applied agent such as TCA or cryotherapy. And never let a 'minor' wart consultation pass without offering HPV vaccination counselling and cervical screening — the same virus family causes cervical cancer.