Page 19 of 35
DR10.7 | Inguinal Bubo Syndromic Management — SDL Guide
Learning Objectives
- Recognise the clinical presentation of an inguinal bubo and name its two principal sexually transmitted causes — lymphogranuloma venereum (LGV) and donovanosis.
- Describe the etiopathogenesis and distinguishing clinical features of LGV and donovanosis, including the groove sign, pseudobubo, and Donovan bodies.
- Construct a differential diagnosis for inguinal lymphadenopathy and select appropriate investigations in a resource-limited setting.
- Apply NACO syndromic case management (Kit 6) to a patient with an inguinal bubo, including the rule to aspirate rather than incise a fluctuant node.
INSTRUCTIONS
A swollen, tender lump in the groin in a sexually active adult is a syndrome with a short and important differential — and getting it wrong has consequences. Lymphogranuloma venereum and donovanosis are both treatable, both transmissible, and both capable of causing disfiguring late complications if missed. This module teaches you to recognise the inguinal bubo, reason through its causes, and deliver NACO syndromic treatment correctly — including the deceptively simple rule that a fluctuant bubo is aspirated, never incised. By the end you will be able to manage this presentation confidently at a primary or district health facility.
References
- NACO National Guidelines on Prevention, Management and Control of STI/RTI (Syndromic Case Management, Inguinal Bubo) (textbook)
- Neena Khanna, Illustrated Synopsis of Dermatology & Sexually Transmitted Diseases, LGV and Donovanosis sections (textbook)
- IADVL Textbook of Dermatology, chapter on Lymphogranuloma Venereum and Granuloma Inguinale (textbook)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
A 28-year-old truck driver presents with a painful swelling in his right groin that has been enlarging for three weeks. He mentions, almost in passing, that there was a small painless sore on his penis a month ago that healed on its own. On examination you find a tender, matted mass of inguinal nodes, and as you palpate you notice the swelling is divided by a groove where the inguinal ligament crosses it. That single physical sign — the groove sign — has just told you the likely diagnosis is lymphogranuloma venereum, and that the 'sore that healed' was its primary lesion. An inguinal bubo is never just a lump; it is a syndrome with a story, and reading that story correctly is what this module is about.
WHY THIS MATTERS
Inguinal bubo is one of the NACO syndromic categories you will be expected to manage independently as a medical officer. Its two main sexually transmitted causes — LGV and donovanosis — are uncommon enough that they are easy to forget but serious enough that missing them causes real harm: untreated LGV progresses to chronic fibrosis, fistulae, and genital elephantiasis, while untreated donovanosis causes progressive, mutilating ulceration. Both also flag a patient who needs HIV testing, partner treatment, and counselling. Competency DR10.7 asks you to 'recognise a patient with LGV and donovanosis based on clinical findings and provide appropriate therapy using syndromic case management' — a recognition-and-treatment skill that begins with knowing what a bubo is and ends with the correct Kit 6 regimen.
RECALL
Recall from Year-1 Anatomy that the inguinal lymph nodes form superficial and deep groups draining the lower limb, the perineum, the external genitalia, and the lower abdominal wall — so a bubo signals infection somewhere in that drainage territory. Recall from Microbiology the difference between an obligate intracellular bacterium (Chlamydia trachomatis) and an encapsulated Gram-negative rod (Klebsiella). You will also build on the genital examination skills from DR10.4 — consent, chaperone, and systematic inguinal node palpation — which you must perform before reasoning about the bubo in front of you.
Presentation of Inguinal Bubo: The Clinical Picture
Clinical Presentation and Causes of Inguinal Bubo
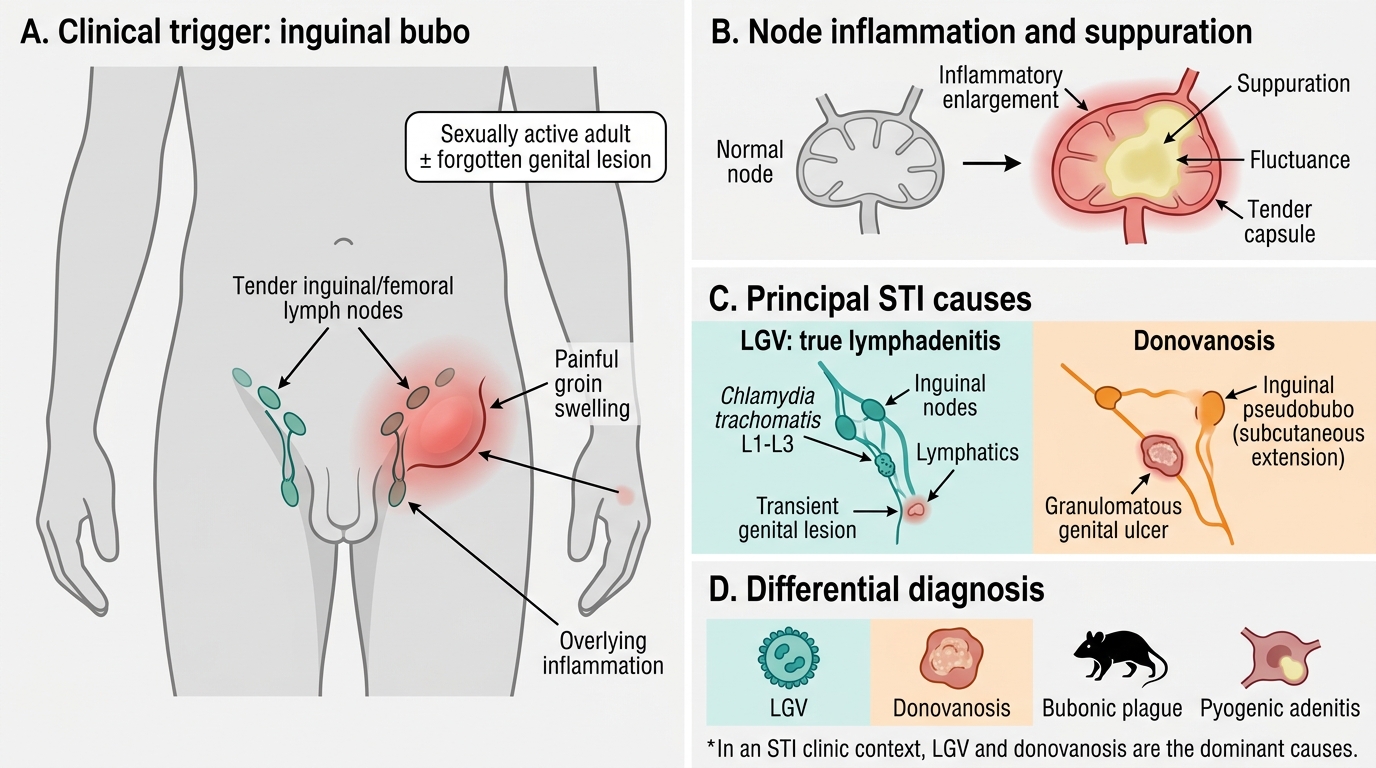
An inguinal bubo is a painful inflammatory enlargement of the inguinal and/or femoral lymph nodes, often with overlying skin changes and sometimes with fluctuance as the node suppurates. The presentation that should trigger this syndrome is a sexually active adult with a tender groin swelling, with or without a preceding genital lesion the patient may not even remember. The two principal sexually transmitted causes you must commit to memory are lymphogranuloma venereum (LGV) and donovanosis (granuloma inguinale); both can present with inguinal involvement, though as you will see, the 'bubo' of donovanosis is often a pseudobubo rather than true lymphadenitis. It is worth briefly contrasting these with non-STI causes of a groin bubo — bubonic plague and pyogenic adenitis — so that you do not anchor prematurely; but in the STI clinic context, LGV and donovanosis dominate the differential.
Key points on presentation:
- A bubo is a tender, inflamed enlargement of inguinal/femoral nodes
- Trigger context: sexually active adult ± preceding genital lesion
- Two main STI causes: LGV and donovanosis
- Non-STI mimics to keep in mind: plague, pyogenic adenitis
LGV Pathogenesis and Donovanosis Biology
LGV Pathogenesis and Donovanosis Biology
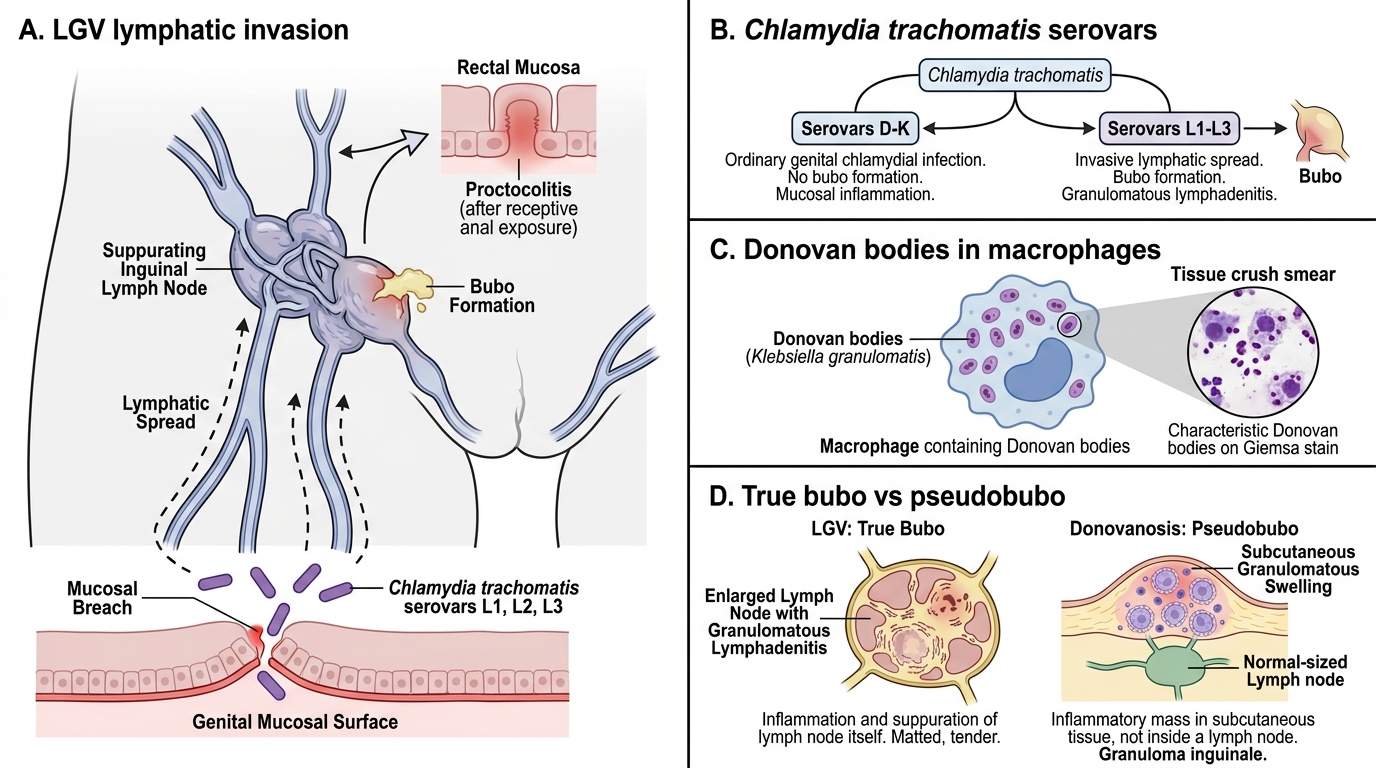
Understanding the two organisms explains every clinical sign that follows. Lymphogranuloma venereum is caused by the invasive serovars L1, L2, and L3 of Chlamydia trachomatis — distinct from serovars D-K, which cause ordinary genital chlamydial infection without bubo formation. These invasive serovars enter through a small mucosal breach, are carried to the regional lymphatics, and provoke a granulomatous lymphadenitis: the nodes enlarge, mat together, and may suppurate, and the infection can extend to the rectum to cause proctocolitis, particularly after receptive anal exposure. Donovanosis, by contrast, is caused by Klebsiella granulomatis (formerly Calymmatobacterium granulomatis), an encapsulated organism that infects and multiplies within macrophages, forming the intracellular Donovan bodies seen on a tissue crush smear. Because donovanosis is primarily a chronic ulcerating disease of the skin and subcutaneous tissue rather than a true lymphadenitis, its 'bubo' is usually a pseudobubo — a subcutaneous granulomatous swelling that mimics, but is not, an enlarged lymph node.
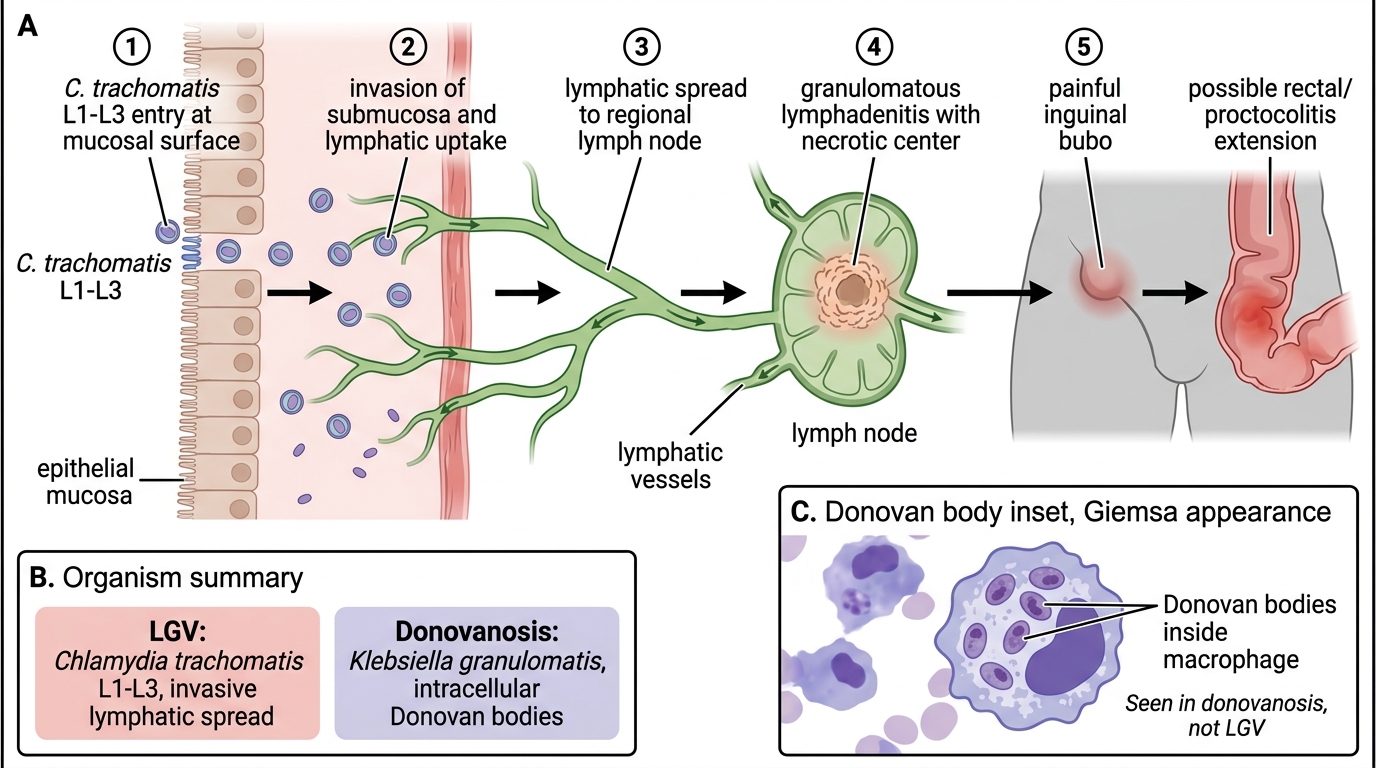
LGV Pathogenesis and Donovan Body Inset
Organism summary:
- LGV: Chlamydia trachomatis serovars L1-L3 → lymphatic invasion → granulomatous lymphadenitis ± proctocolitis
- Donovanosis: Klebsiella granulomatis → intramacrophage Donovan bodies → chronic ulceration, pseudobubo
SELF-CHECK
Which organism and serovars cause lymphogranuloma venereum, and how do they differ from the serovars causing ordinary genital chlamydial infection?
A. Klebsiella granulomatis serovars L1-L3; the same organism causes both
B. Chlamydia trachomatis serovars L1-L3 (invasive), distinct from serovars D-K which cause non-invasive genital infection
C. Chlamydia trachomatis serovars D-K, which also cause bubonic plague
D. Haemophilus ducreyi, which causes both LGV and chancroid
Reveal Answer
Answer: B. Chlamydia trachomatis serovars L1-L3 (invasive), distinct from serovars D-K which cause non-invasive genital infection
LGV is caused by the invasive serovars L1, L2, and L3 of Chlamydia trachomatis, which invade lymphatics and cause granulomatous lymphadenitis and bubo. Serovars D-K cause ordinary, non-invasive genital chlamydial infection without bubo. Klebsiella granulomatis causes donovanosis, and Haemophilus ducreyi causes chancroid.
Clinical Features of LGV and Donovanosis
LGV versus Donovanosis: Key Clinical Features
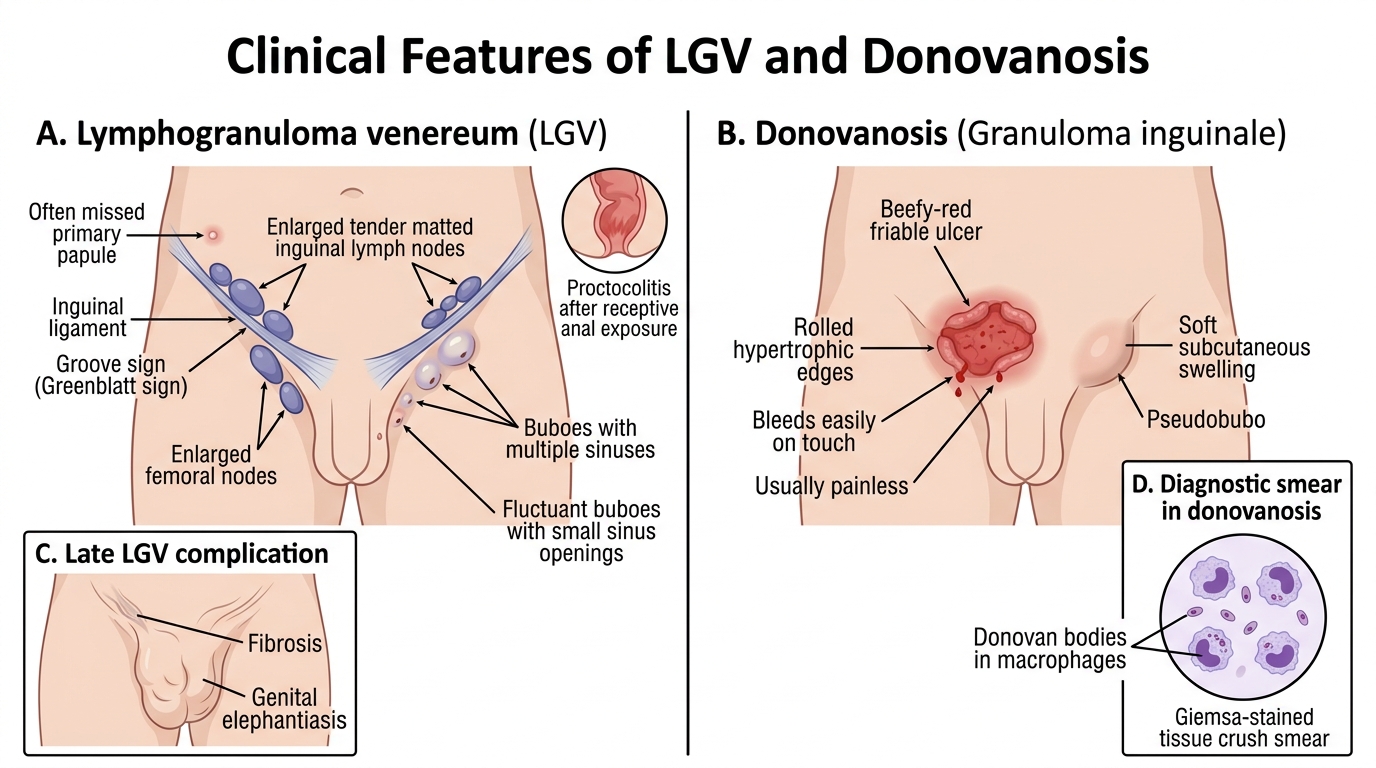
The clinical features flow directly from the biology and allow bedside differentiation. In LGV, an often-missed small primary papule or pustule heals quickly, and the patient presents weeks later in the secondary stage with tender, matted inguinal and femoral nodes; the pathognomonic groove sign (Greenblatt sign) appears when the inguinal ligament bisects the enlarged node masses above and below it. Buboes may become fluctuant and discharge through multiple sinuses, and receptive anal exposure can produce proctocolitis. In donovanosis, the hallmark is a beefy-red, friable ulcer with rolled, hypertrophic edges that bleeds easily on touch; it is usually painless or only mildly tender, spreads slowly by contiguity, and forms a pseudobubo rather than true lymphadenitis. Diagnosis is confirmed by demonstrating Donovan bodies — intracellular organisms within macrophages — on a tissue crush smear stained with Giemsa. Late, untreated disease in either condition causes disfiguring complications: fibrosis and genital elephantiasis in LGV, and progressive mutilating ulceration in donovanosis.
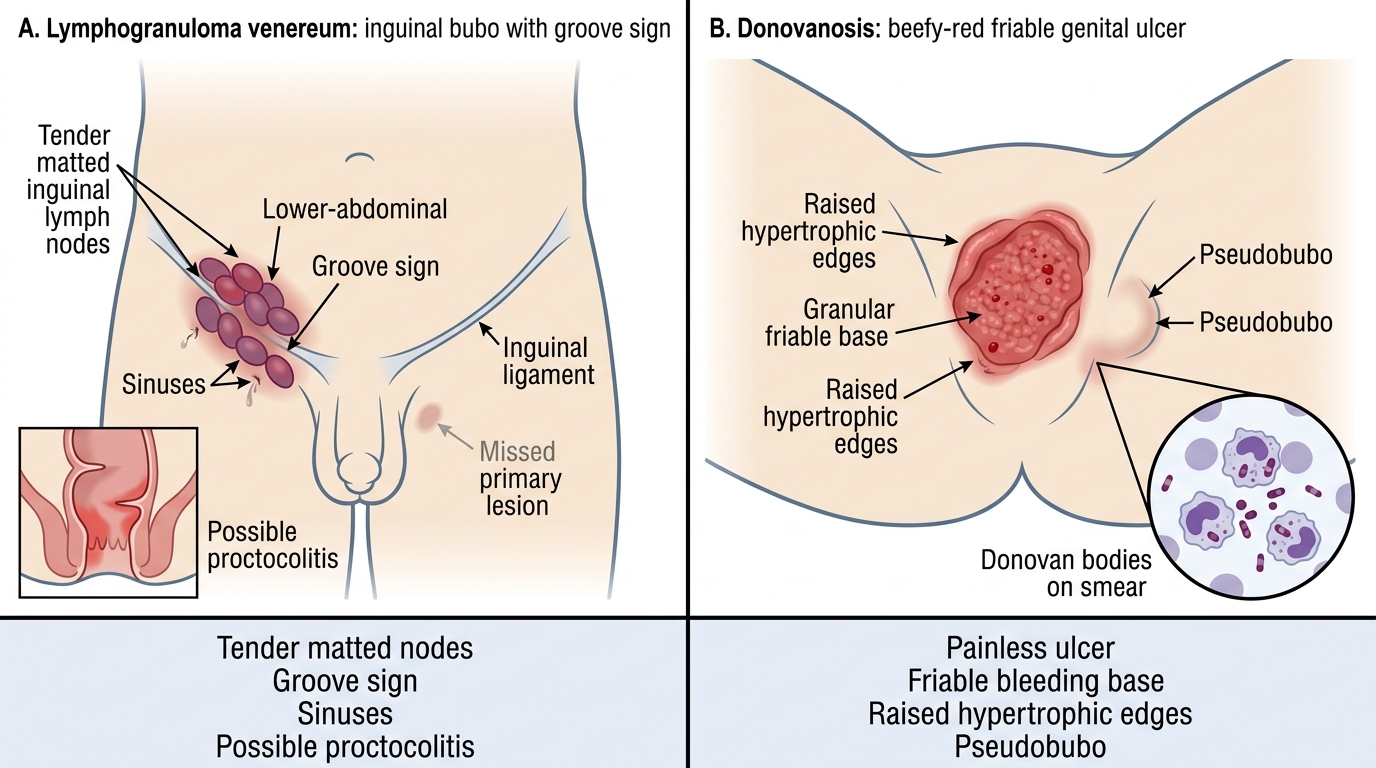
LGV versus Donovanosis: Key Clinical Differences
Distinguishing features:
- LGV: missed primary lesion → tender matted nodes, groove sign, sinuses, possible proctocolitis
- Donovanosis: beefy-red friable bleeding ulcer, painless, pseudobubo, Donovan bodies on smear