Page 13 of 35
DR10.3 | Non-Syphilitic Genital Ulcer Differential Diagnosis — SDL Guide
Learning Objectives
- Describe the clinical features of chancroid and herpes genitalis and distinguish them from syphilis.
- Use the painful-versus-painless framework to triage genital ulcer disease.
- Explain the etiopathogenesis of the principal non-syphilitic genital ulcers.
- Select and interpret the appropriate diagnostic test (Gram stain, Tzanck smear, PCR) for each cause.
- Outline the principles of treatment, including the NACO syndromic kits for genital ulcer disease.
INSTRUCTIONS
Not every genital ulcer is syphilis. Chancroid and herpes genitalis are common, and they differ from syphilis in a feature you can assess in seconds — pain. This module teaches you to use the painful-versus-painless framework to triage a genital ulcer, to recognise the principal non-syphilitic causes, and to confirm them with the right bedside test, so that you treat correctly even before serology returns.
References
- Neena Khanna, Illustrated Synopsis of Dermatology and Sexually Transmitted Diseases, Ch. on Genital Ulcer Disease (textbook)
- IADVL Textbook of Dermatology, Ch. on Chancroid, Herpes Genitalis, and Genital Ulcer Disease (textbook)
- NACO National Guidelines on Prevention, Management and Control of RTI/STI, Ministry of Health & Family Welfare, Government of India (textbook)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
Two men attend the STI clinic on the same morning, each with a genital ulcer. The first has a single, firm sore that does not hurt at all; the second has a cluster of small, exquisitely painful ulcers and can barely tolerate examination. Before any laboratory test, that one difference — painless versus painful — has already split them into different diagnostic worlds: the first toward syphilis, the second toward herpes or chancroid. The genital ulcer is one of the few situations in medicine where a single clinical question, asked at the bedside, reshapes the entire differential. Learning to use it well is the core skill of this module.
WHY THIS MATTERS
Genital ulcers are a daily presentation in STI and dermatology clinics, and getting the differential right matters for several reasons. The treatments diverge completely — herpes needs antivirals, chancroid needs antibacterials, and syphilis needs penicillin — so a wrong label means a wrong drug. Genital ulcers also markedly increase the risk of HIV transmission, so each one is a prevention opportunity. And in the Indian setting, where same-day organism identification is often impossible, the ability to triage by clinical pattern and treat syndromically is what lets you help the patient at the first visit. This SDL equips you to distinguish the non-syphilitic ulcers from each other and from syphilis, and to act on that distinction.
RECALL
Recall the groundwork. From the syphilis SDLs you know the primary chancre is a single, painless, indurated ulcer — the prototype of the painless group. From microbiology you know herpes simplex virus replicates in epithelium and then establishes latency in dorsal root ganglia, which is why genital herpes recurs. You also met the NACO syndromic approach to genital ulcer disease, which splits ulcers into a non-herpetic group (Kit 3, antibacterial) and a herpetic group (Kit 4, antiviral). This module fills in the non-syphilitic causes — chancroid and herpes principally, with lymphogranuloma venereum and donovanosis as supporting differentials — and shows how each fits the painful-versus-painless framework.
The Genital Ulcer — A Clinical Framework for Rapid Triage
Rapid Clinical Triage of Genital Ulcers
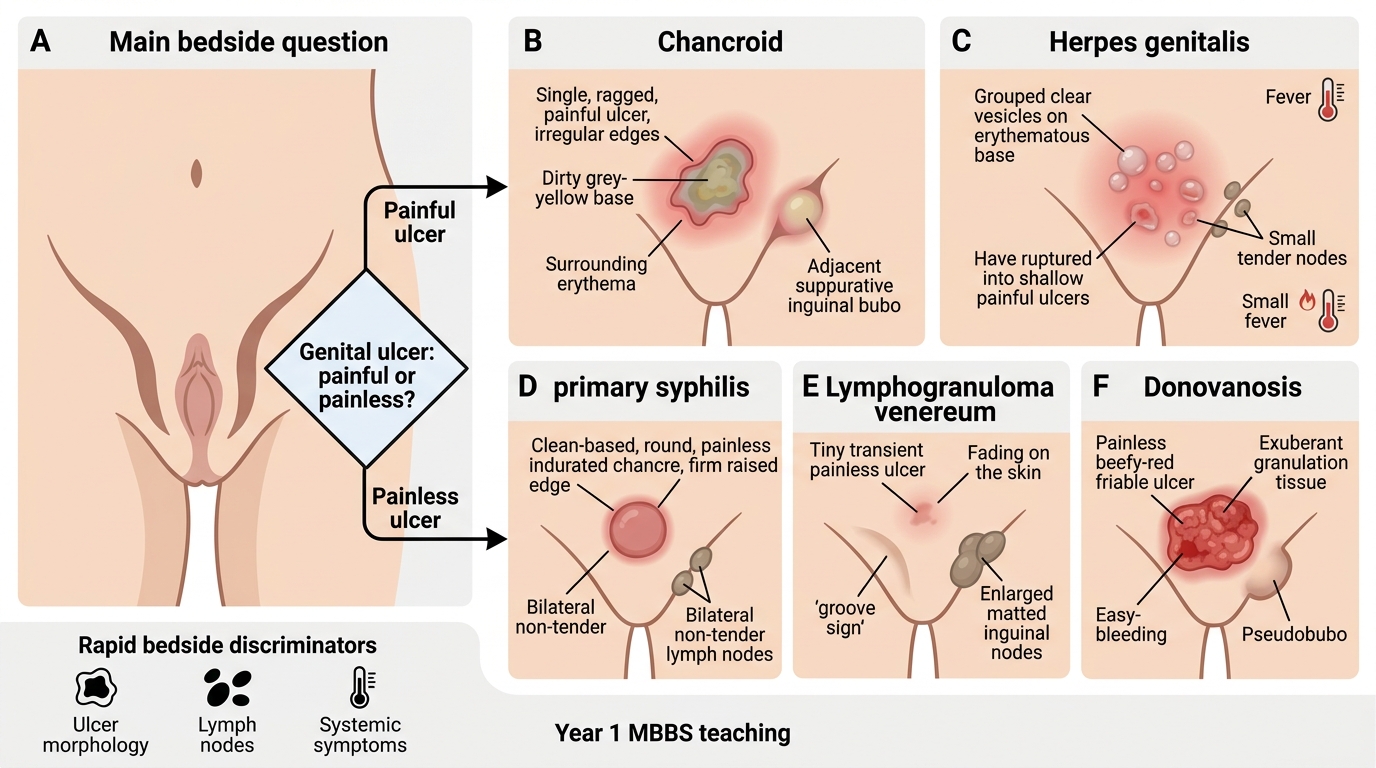
The most useful first move with any genital ulcer is to apply a simple clinical framework built around a single, high-yield question: is the ulcer painful or painless? This one feature carries enormous discriminating power. The painful ulcers are chancroid (a painful, soft, ragged ulcer) and herpes genitalis (painful grouped vesicles that rupture into shallow ulcers). The painless ulcers are the primary chancre of syphilis (painless and indurated), and — at least early — lymphogranuloma venereum (a transient, often-unnoticed ulcer) and donovanosis (a painless, beefy-red, friable ulcer). Layered onto pain are a few other rapidly assessable features: the morphology of the ulcer (indurated and clean-based in syphilis; soft and ragged with a dirty base in chancroid; grouped vesicles in herpes; beefy-red and friable in donovanosis), the lymph nodes (non-tender and bilateral in syphilis; tender and suppurative in chancroid; tender in primary herpes; the matted "groove sign" of LGV; pseudobuboes in donovanosis), and systemic symptoms (prominent in primary herpes, usually absent in the others).
Used together, these features let you reach a working diagnosis at the bedside and decide which confirmatory test to send and which empirical treatment to start. The framework does not replace testing, but it organises the differential so that testing is targeted rather than scattershot — and so that, where testing is unavailable, syndromic treatment can begin immediately.
- Ask first: painful or painless? Painful → chancroid, herpes; painless → syphilis, LGV (early), donovanosis.
- Layer on morphology, lymph node character, and systemic symptoms.
- The framework targets testing and enables immediate syndromic treatment.
Pathogens and Pathogenesis of Non-Syphilitic Genital Ulcers
Pathogenesis of Non-Syphilitic Genital Ulcers
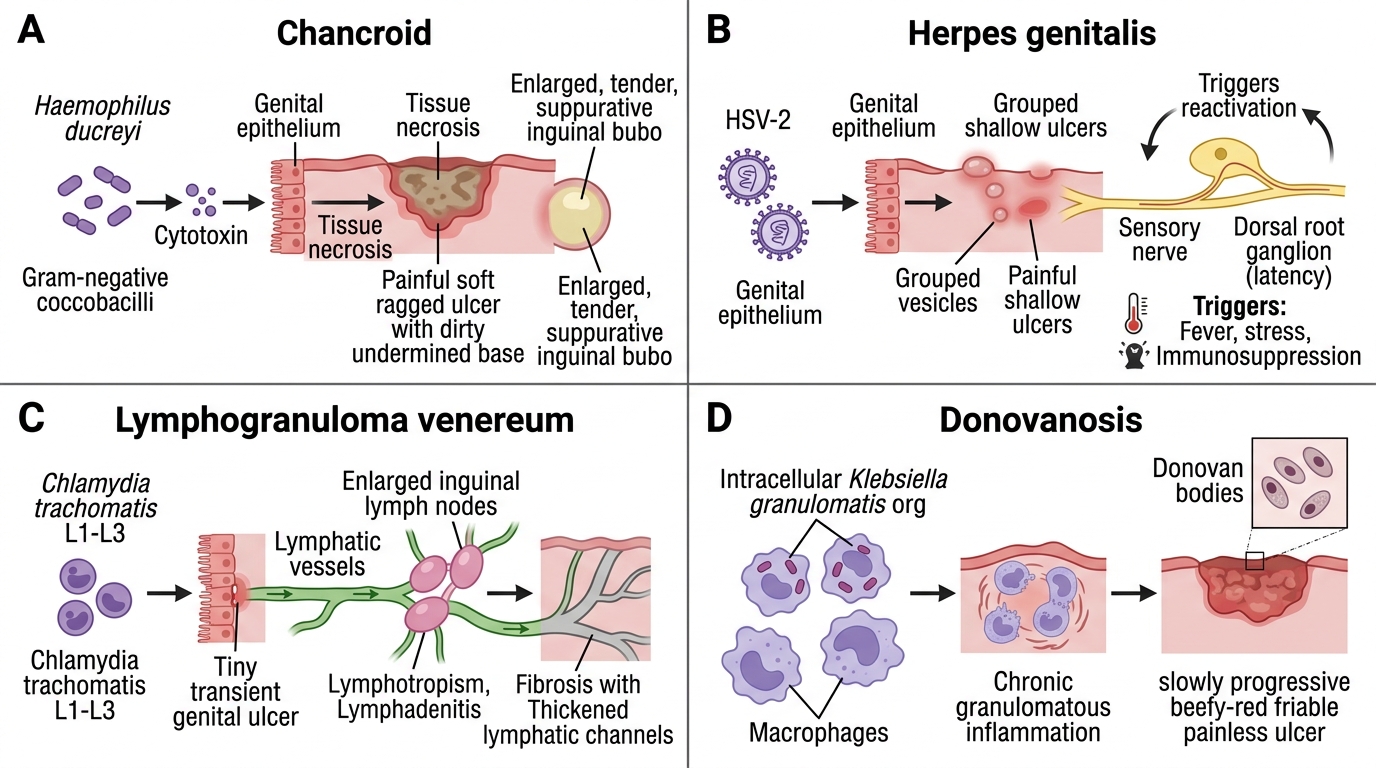
Each non-syphilitic ulcer's clinical behaviour follows directly from its causative organism and how that organism damages tissue. Chancroid is caused by Haemophilus ducreyi, a Gram-negative coccobacillus that produces a cytotoxin; the cytotoxin-mediated tissue necrosis explains the painful, soft, ragged ulcer with its dirty, undermined base, and the organism's tendency to spread to regional nodes explains the tender, suppurative inguinal bubo. Herpes genitalis is caused chiefly by herpes simplex virus type 2 (with HSV-1 increasingly implicated); the virus replicates lytically in genital epithelium to produce the grouped vesicles and painful ulcers, then travels up sensory nerves to establish latency in the dorsal root ganglia — and it is reactivation from this latent reservoir, triggered by fever, stress, or immunosuppression, that causes the characteristic recurrences. Lymphogranuloma venereum (LGV) is caused by the L1–L3 serovars of Chlamydia trachomatis, which are uniquely lymphotropic; this lymphatic tropism is why LGV's hallmark is not the (transient) ulcer but the dramatic inguinal lymphadenitis and later fibrosis. Donovanosis (granuloma inguinale) is caused by Klebsiella granulomatis (formerly Calymmatobacterium granulomatis), an intracellular organism that provokes a chronic granulomatous response, producing the slowly progressive, beefy-red, friable, painless ulcer.
Understanding these mechanisms is not academic: the cytotoxin explains why chancroid hurts, dorsal-root-ganglion latency explains why herpes recurs, lymphotropism explains LGV's nodal disease, and the intracellular Donovan bodies that the granulomatous response harbours are exactly what you will look for on the diagnostic smear.
- Chancroid = H. ducreyi (cytotoxin → painful ragged ulcer + suppurative bubo).
- Herpes = HSV-2 (lytic epithelial replication + dorsal-root-ganglion latency → recurrence).
- LGV = C. trachomatis L1–L3 (lymphotropic → nodal disease); donovanosis = K. granulomatis (granulomatous → beefy-red friable ulcer).
Clinical Features of Chancroid and Herpes Genitalis
Clinical Differentiation of Chancroid and Herpes Genitalis
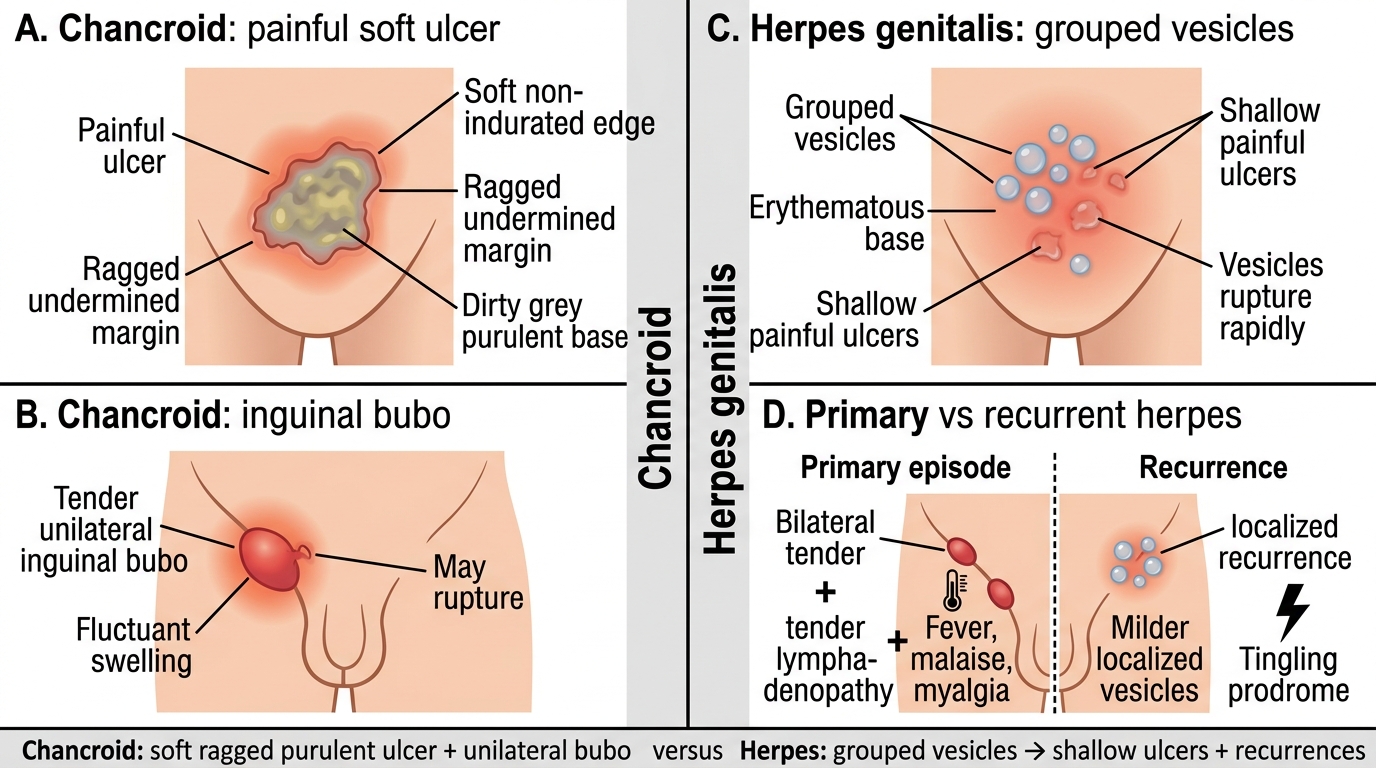
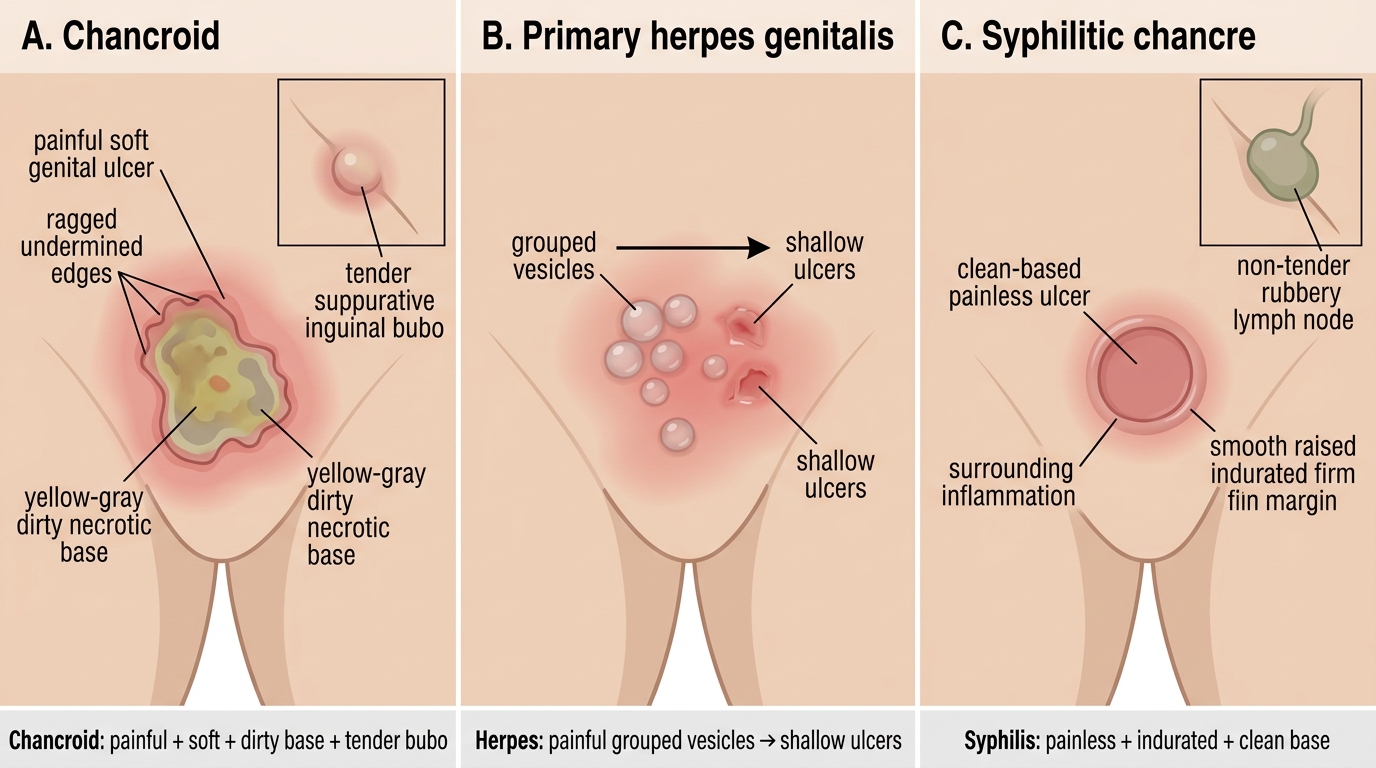
The two principal non-syphilitic ulcers have distinct clinical signatures that, with the painful-versus-painless framework, allow confident bedside differentiation. Chancroid (incubation roughly 3–10 days) presents as one or more painful ulcers that are characteristically soft (non-indurated, in deliberate contrast to the firm syphilitic chancre), with ragged, undermined edges and a dirty grey, often purulent base; about half of patients develop a tender, fluctuant, usually unilateral inguinal bubo that may rupture. Herpes genitalis presents as grouped vesicles on an erythematous base that quickly rupture to leave clusters of shallow, painful ulcers. The first (primary) episode is the most severe, often with bilateral tender inguinal lymphadenopathy and systemic symptoms (fever, malaise, myalgia); subsequent recurrences are milder, more localised, and frequently heralded by a tingling prodrome, reflecting reactivation from latency. The recurrent, grouped, vesicular nature is the giveaway.
The supporting differentials round out the picture. LGV classically gives a small, painless, transient ulcer that is often missed, followed by tender, matted inguinal lymphadenopathy with the "groove sign" (nodes above and below the inguinal ligament), and, if untreated, chronic fibrosis and genital elephantiasis. Donovanosis gives a slowly enlarging, painless, beefy-red, friable ulcer that bleeds easily on contact, characteristically without true lymphadenopathy (subcutaneous granulomas called pseudobuboes may mimic nodes).
Genital Ulcer Disease: Key Clinical Differences
- Chancroid: painful, soft, ragged, undermined ulcer + tender suppurative unilateral bubo.
- Herpes: painful grouped vesicles → shallow ulcers; primary episode systemic; recurrences with prodrome.
- LGV: transient painless ulcer + groove-sign lymphadenopathy; donovanosis: painless beefy-red friable ulcer, no true nodes.
SELF-CHECK
A patient has a single PAINFUL genital ulcer that is soft, has ragged undermined edges and a dirty base, accompanied by a tender, fluctuant inguinal swelling. Which diagnosis is most likely?
A. Primary syphilis
B. Chancroid (Haemophilus ducreyi)
C. Donovanosis (Klebsiella granulomatis)
D. Lymphogranuloma venereum
Reveal Answer
Answer: B. Chancroid (Haemophilus ducreyi)
A painful, soft, ragged, undermined ulcer with a dirty base plus a tender suppurative (fluctuant) inguinal bubo is the classic picture of chancroid (Haemophilus ducreyi). Syphilis is painless and indurated; donovanosis is painless, beefy-red and friable without true nodes; LGV's ulcer is transient and painless with matted groove-sign nodes.