Page 4 of 35
DR10.5 | Sexual History Safe Behaviour Counselling and HIV Pretest Counselling — SDL Guide
Learning Objectives
- Take a structured, non-judgmental sexual history using the 5 Ps framework.
- Provide patient education on safe sexual behaviours and risk reduction.
- Conduct HIV pre-test counselling, including informed consent and explanation of the window period.
- Stratify a patient's risk and tailor risk-reduction advice accordingly.
- Handle sensitive disclosures and referral pathways professionally and confidentially.
INSTRUCTIONS
A sexual history is one of the most clinically valuable yet most frequently skipped parts of a consultation. Asked well, it uncovers infections that would otherwise be missed, opens the door to prevention, and is the gateway to HIV testing. Asked badly — or not at all — it leaves the patient unprotected and the clinician blind. This module gives you a structured, respectful way to take that history and to counsel a patient before an HIV test, so that testing is informed, consensual, and useful.
References
- NACO Operational Guidelines for Integrated Counselling and Testing Centres (ICTC), Ministry of Health & Family Welfare, Government of India (textbook)
- Neena Khanna, Illustrated Synopsis of Dermatology and Sexually Transmitted Diseases, Ch. on STD counselling and HIV (textbook)
- IADVL Textbook of Dermatology, Ch. on Sexually Transmitted Infections and Counselling (textbook)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
A 22-year-old woman attends with recurrent vaginal discharge that has not settled despite two previous courses of treatment. The temptation is to write another prescription and move on. But a few careful, non-judgmental questions reveal she has a new partner, uses no protection, and has never been tested for HIV or syphilis. In two minutes you have moved from treating a symptom to addressing the actual driver of her risk — and you have created the opening to offer her testing she did not know she needed. The sexual history is not an awkward formality; it is often the single most informative part of the consultation, and the gateway to prevention.
WHY THIS MATTERS
As a clinician you will see patients whose presenting complaint is the tip of a larger risk picture, and patients who will never volunteer a sexual concern unless you make it safe to do so. The ability to take a sexual history and to counsel before an HIV test is an examinable CBME competency and, more importantly, a daily clinical necessity in antenatal clinics, STI clinics, family planning, and general practice. Under the National AIDS Control Programme, pre-test counselling is a defined step before HIV testing at every Integrated Counselling and Testing Centre. Doing it well protects your patient's autonomy, improves the yield of testing, and turns a clinic visit into an opportunity for genuine prevention.
RECALL
Recall what you already know that this skill builds on. From microbiology and your STI reading you know that HIV is transmitted sexually, vertically, and through blood, and that a person can be infected and infectious while feeling entirely well. From immunology you know that after infection there is a delay before the body produces detectable antibodies — and that modern tests can detect viral antigen earlier than antibody. You also know, from communication-skills teaching, that open-ended questions elicit more than closed ones, and that confidentiality is a cornerstone of the doctor–patient relationship. The sexual history and pre-test counselling weave these threads together into a single, structured conversation.
Why Sexual History-Taking Is a Clinical Core Competency
Sexual History-Taking as a Core Clinical Competency
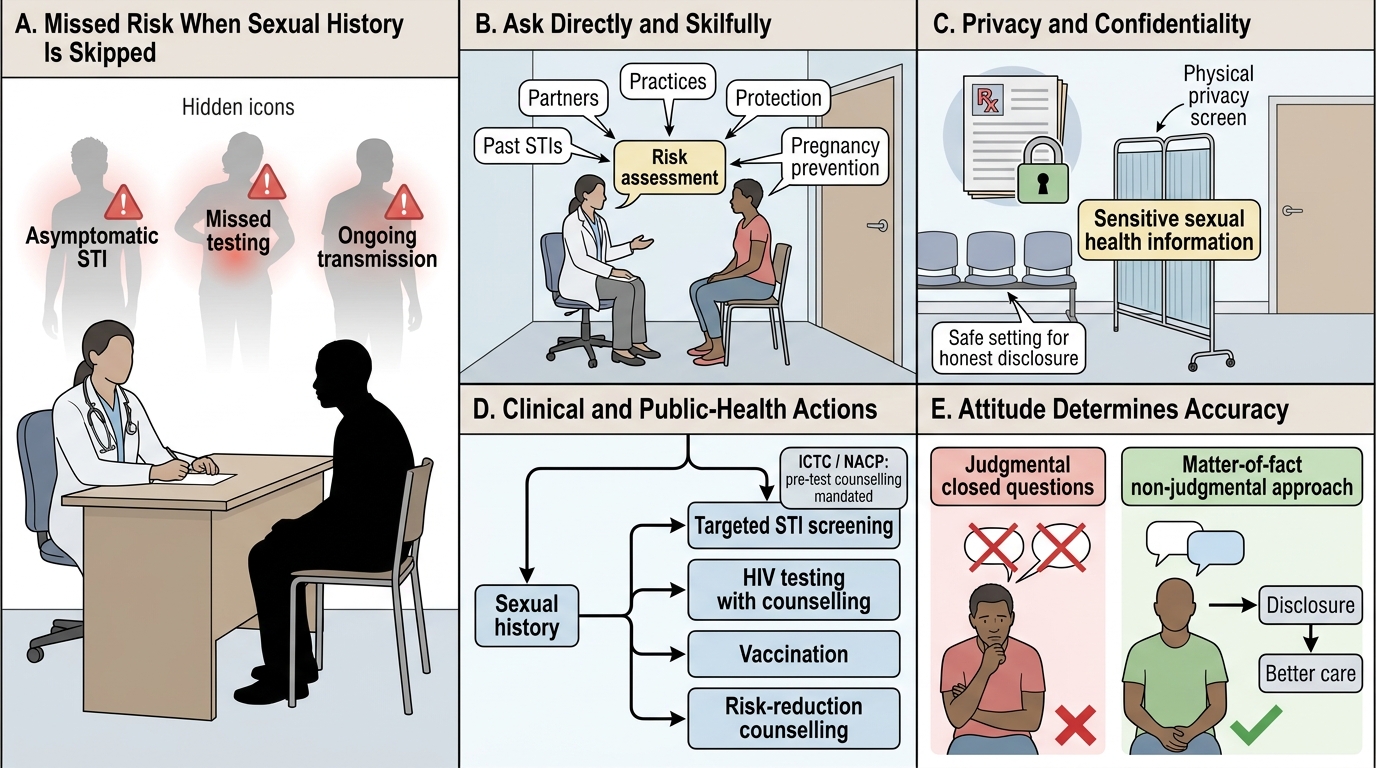
Sexual history-taking is a clinical core competency because the cost of skipping it is measured in missed diagnoses, missed prevention, and missed testing. Many sexually transmitted infections are asymptomatic or minimally symptomatic — particularly in women — so the only way to surface the risk is to ask about it directly and skilfully. A patient who is never asked about partners, practices, or protection cannot be offered the targeted screening, vaccination, or counselling they need; the infection continues silently and may be transmitted onward. There is also a clear ethical and legal frame: the patient's sexual health information is among the most sensitive a clinician handles, and it must be elicited with explicit attention to privacy and confidentiality, in a setting where the patient feels safe to speak honestly. Under the National AIDS Control Programme, structured counselling before HIV testing is not optional but a mandated component of care at every Integrated Counselling and Testing Centre, reflecting how central this conversation is to the public-health response.
The barrier is rarely the patient and usually the clinician's own discomfort. Students often fear giving offence, so they either skip the history or rush it with closed, judgmental questions that shut the patient down. The skill, therefore, is partly technical — a structure to follow — and partly attitudinal: a calm, matter-of-fact, non-judgmental manner that signals these questions are routine and the answers will be held in confidence.
- Many STIs are asymptomatic — only a sexual history surfaces the risk.
- Sexual health information demands explicit privacy and confidentiality.
- Pre-test counselling is a mandated NACP step at every ICTC.
The 5 Ps Framework and Principles of Non-Judgmental Enquiry
The 5 Ps Framework for Non-Judgmental Sexual History Taking
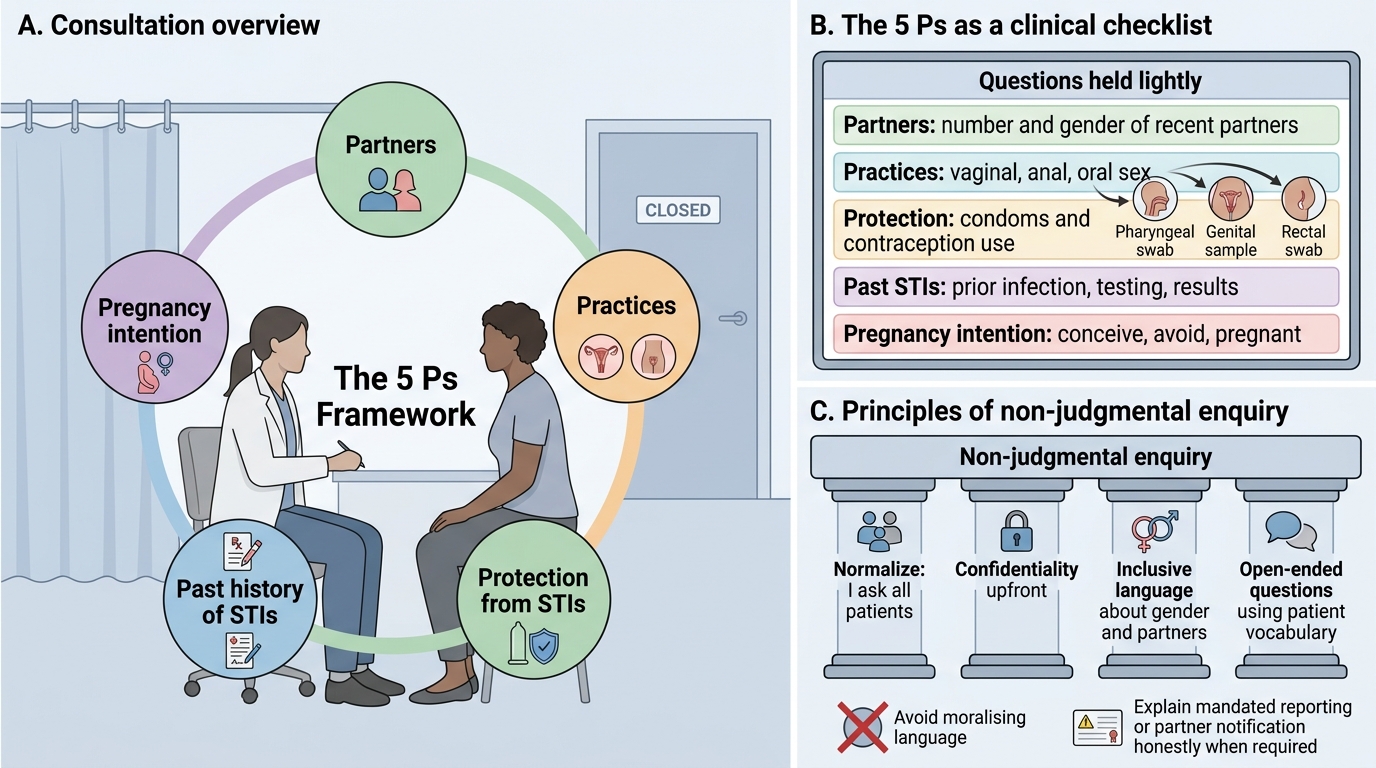
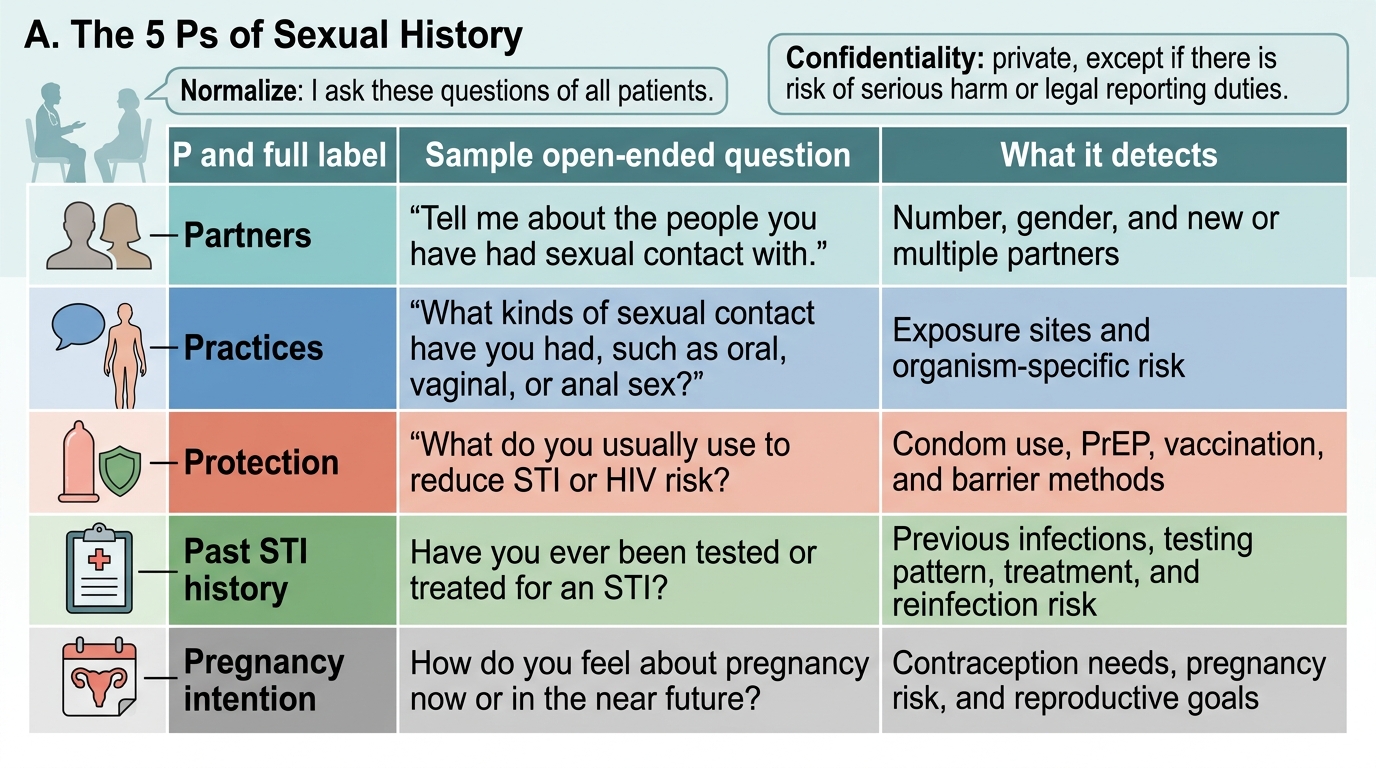
A structured framework prevents both omission and awkwardness, and the most widely taught is the 5 Ps: Partners, Practices, Protection from STIs, Past history of STIs, and Pregnancy intention. Partners asks about the number and gender of recent partners and whether they have other partners. Practices asks, non-judgmentally, what kinds of sex the patient has (vaginal, anal, oral), because this determines which sites are at risk and which to examine or sample. Protection from STIs asks about condom use and contraception — consistently, sometimes, never — and about the patient's understanding of how to reduce risk. Past history asks about previous STIs, previous testing, and results. Pregnancy intention asks whether the patient is trying to conceive, avoid pregnancy, or is currently pregnant, which shapes contraceptive and screening advice. Used as a checklist held lightly, the 5 Ps ensure nothing important is missed while the conversation still flows naturally.
The principles underlying delivery matter as much as the content. Use open-ended questions and the patient's own vocabulary; adopt inclusive, non-assumptive language about gender and partners; normalise the questions ("I ask all my patients about this"); and be explicit about confidentiality up front. Avoid moralising language, and separate the clinical fact-finding from any value judgement. Where the law mandates partner notification or reporting, be honest about its limits at the outset rather than after a disclosure.
The 5 Ps of Sexual History
- The 5 Ps: Partners, Practices, Protection, Past STI history, Pregnancy intention.
- Use open-ended, inclusive, non-judgmental language and normalise the questions.
- State confidentiality — and its limits — up front.
Conducting the Sexual History and HIV Pre-Test Counselling Session
Provided image
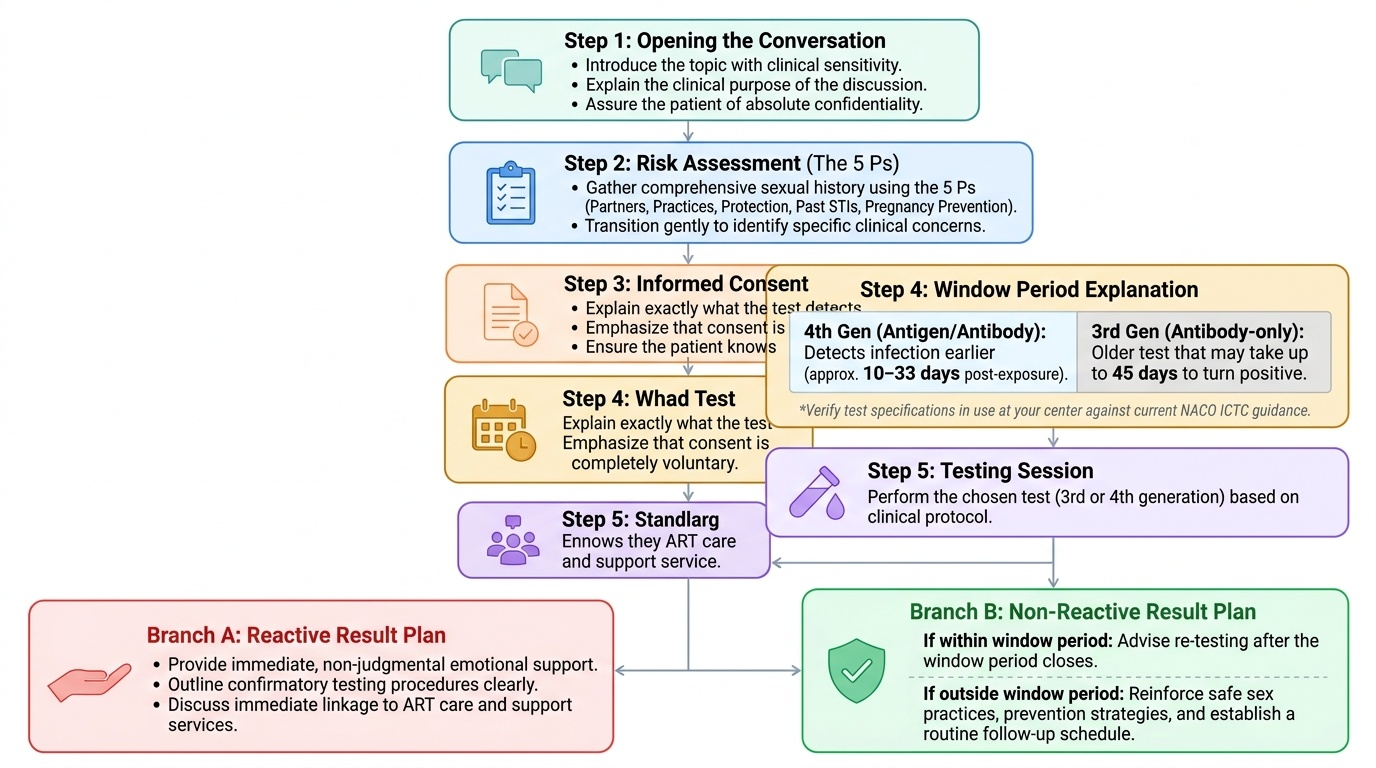
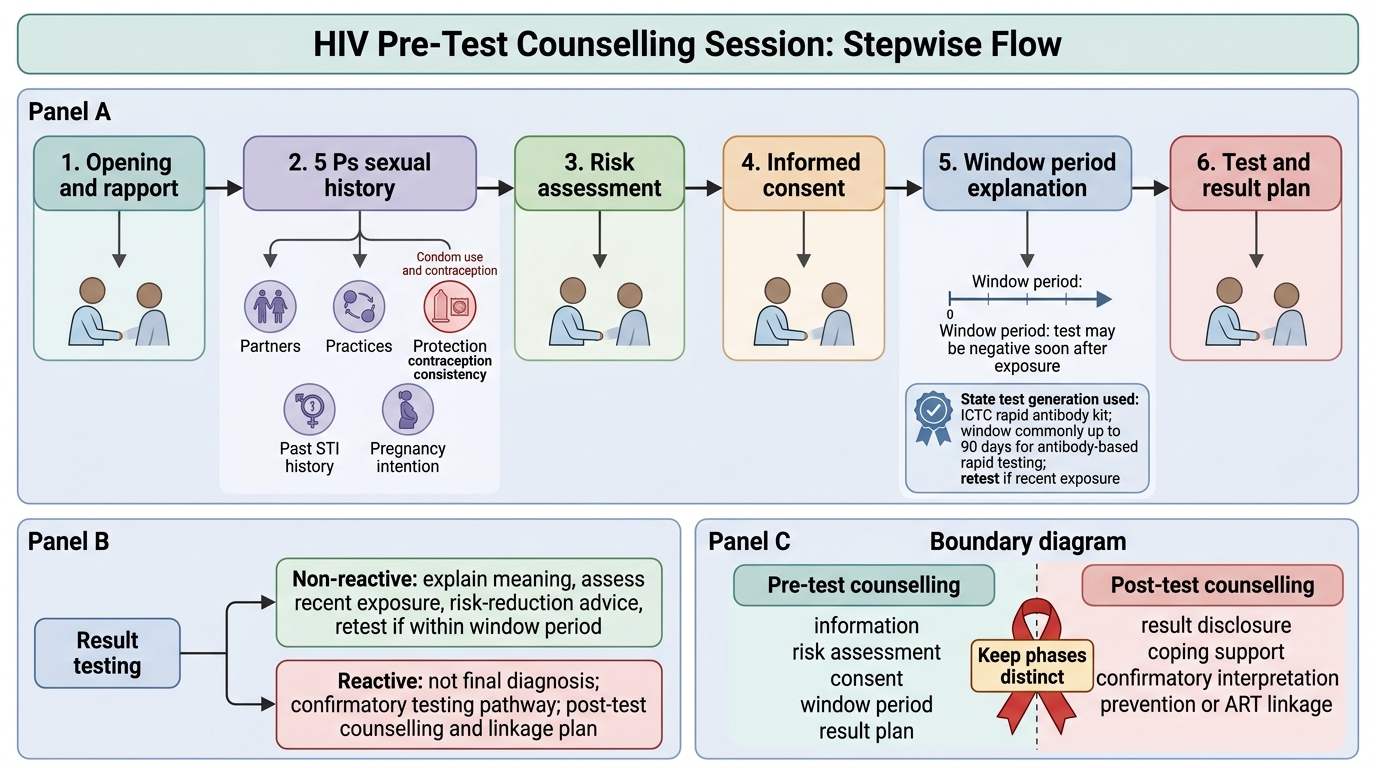
Conducting the session well means following a clear sequence so that the conversation builds logically from rapport to consent. Begin by opening the conversation: introduce the topic, explain why you are asking, and assure confidentiality. Then work through the 5 Ps to build a picture of risk. Use what you learn to transition to risk assessment — naming, gently, the specific exposures that raise concern. From there, move into HIV pre-test counselling proper: explain what the test detects, that consent is voluntary and the patient may decline, and crucially explain the window period — the interval after exposure during which a test may read negative despite infection. The length of this period depends on the test generation, so you must state which test is being used: a fourth-generation antigen/antibody combination assay detects infection earlier (roughly ten to thirty-three days after exposure), whereas an older antibody-only (third-generation) test may take up to about forty-five days to turn positive. Always specify the test rather than quoting a bare number, and verify the test in use at your centre against current NACO ICTC guidance. Finally, close by preparing the patient for the result: what a reactive result will mean, what a non-reactive result within the window period will mean, and the plan for follow-up.
This pre-test conversation is distinct from post-test counselling. Pre-test counselling covers risk assessment, consent, and the window period; post-test counselling covers disclosure of the result, its meaning, and linkage to care or to risk-reduction support. Keeping the two phases clear in your own mind keeps the session structured for the patient.
HIV Pre-Test Counselling Flow at ICTC
- Sequence: open → 5 Ps → risk assessment → consent → window period → result plan.
- State the test generation when explaining the window period; verify against current ICTC guidance.
- Pre-test counselling ≠ post-test counselling — keep the phases distinct.
SELF-CHECK
In the 5 Ps framework for taking a sexual history, what does the 'Protection' P specifically assess?
A. The patient's protection from domestic violence
B. Whether and how consistently the patient uses condoms and contraception to reduce STI and pregnancy risk
C. The legal protections available to the patient under confidentiality law
D. The patient's vaccination status against all infectious diseases
Reveal Answer
Answer: B. Whether and how consistently the patient uses condoms and contraception to reduce STI and pregnancy risk
In the 5 Ps (Partners, Practices, Protection, Past STI history, Pregnancy intention), the 'Protection from STIs' P assesses condom use and contraception — whether the patient uses protection, how consistently, and their understanding of risk reduction. This directly informs the risk-reduction counselling that follows.