Page 8 of 35
DR10.2 | Syphilis Diagnosis — SDL Guide (Part 2)
Diagnostic Tests for Syphilis — Direct Detection and Serology
Diagnostic Tests for Syphilis
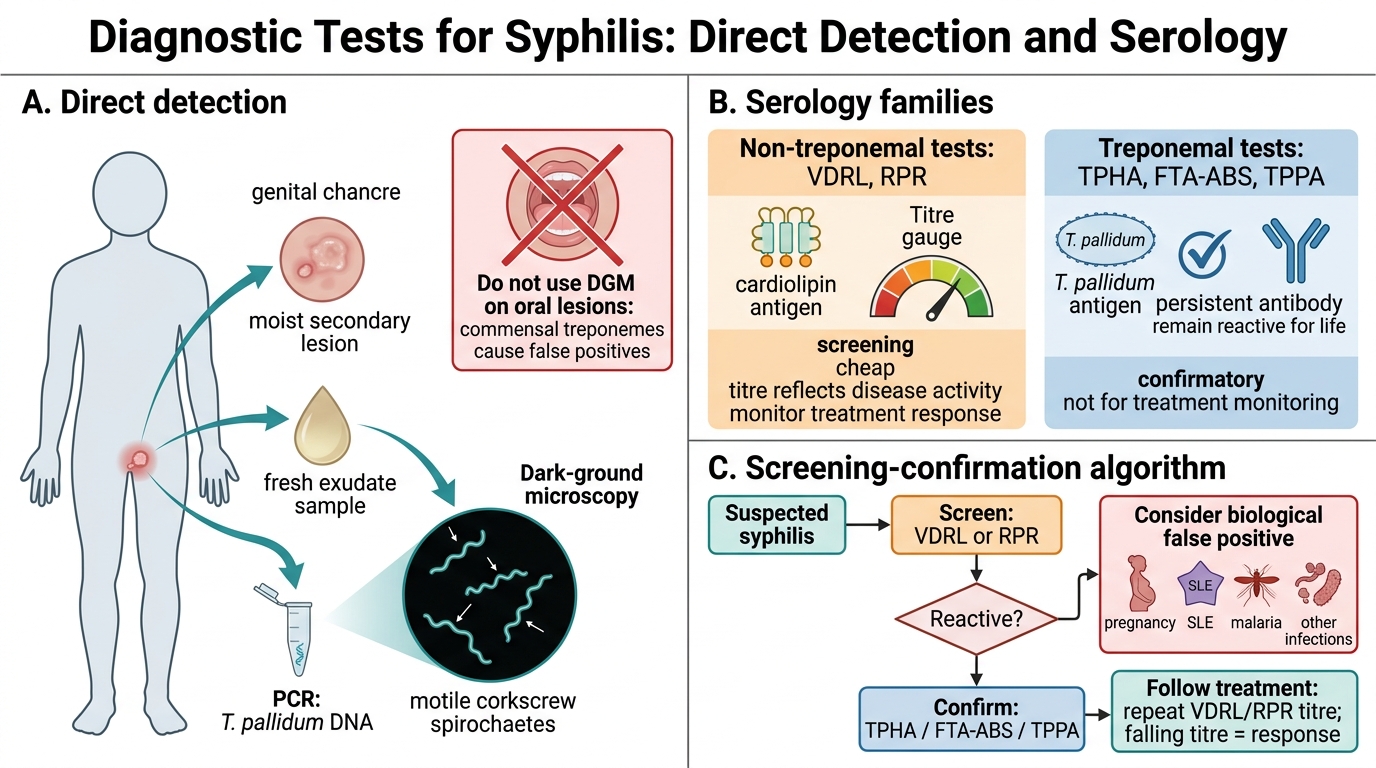
Choosing the right test means understanding what each one detects and when it is reliable. Direct detection demonstrates the organism itself: dark-ground microscopy (DGM) of fresh exudate from a chancre or a moist secondary lesion shows the motile spirochaetes and is highly specific in early syphilis — but it is only valid on genital/wet lesions, not oral ones, because harmless commensal treponemes in the mouth would give a false positive; PCR can also detect treponemal DNA where available. Serology is the mainstay, and it comes in two families with complementary roles. Non-treponemal tests — VDRL and RPR — detect antibody to cardiolipin; they are cheap, used for screening, and, crucially, their titre rises and falls with disease activity, so they are used to monitor treatment response. Their weakness is biological false positives (BFPs): conditions such as pregnancy, systemic lupus erythematosus, malaria, and other infections can produce a reactive non-treponemal test in the absence of syphilis. Treponemal tests — TPHA, FTA-ABS, and TPPA — detect antibody to T. pallidum antigens directly; they are confirmatory, they sort out a true positive from a biological false positive, but they remain reactive for life even after successful treatment, so they cannot be used to monitor response or to prove cure.
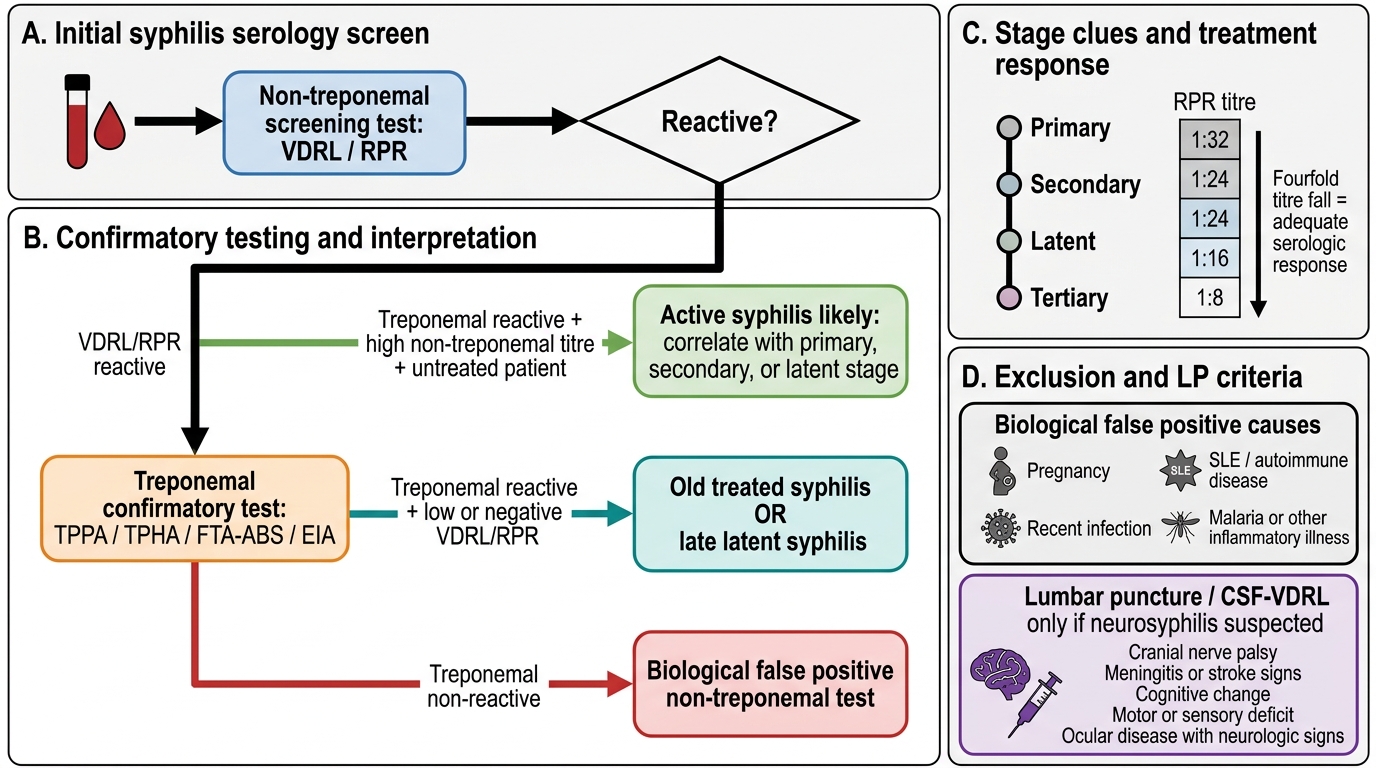
The practical algorithm follows from these properties: screen with a non-treponemal test, confirm a reactive screen with a treponemal test, and use the non-treponemal titre to monitor treatment. A discordant pattern — reactive non-treponemal but negative treponemal — points to a biological false positive rather than syphilis.
Syphilis Diagnostic Tests and Serological Interpretation
- Direct: dark-ground microscopy of chancre exudate (not oral lesions); PCR where available.
- Non-treponemal (VDRL/RPR): screening + titre monitoring; prone to biological false positives.
- Treponemal (TPHA/FTA-ABS/TPPA): confirmatory; stay reactive for life — not for monitoring.
Interpreting Serological Results and Staging the Patient
Interpreting Syphilis Serology and Staging
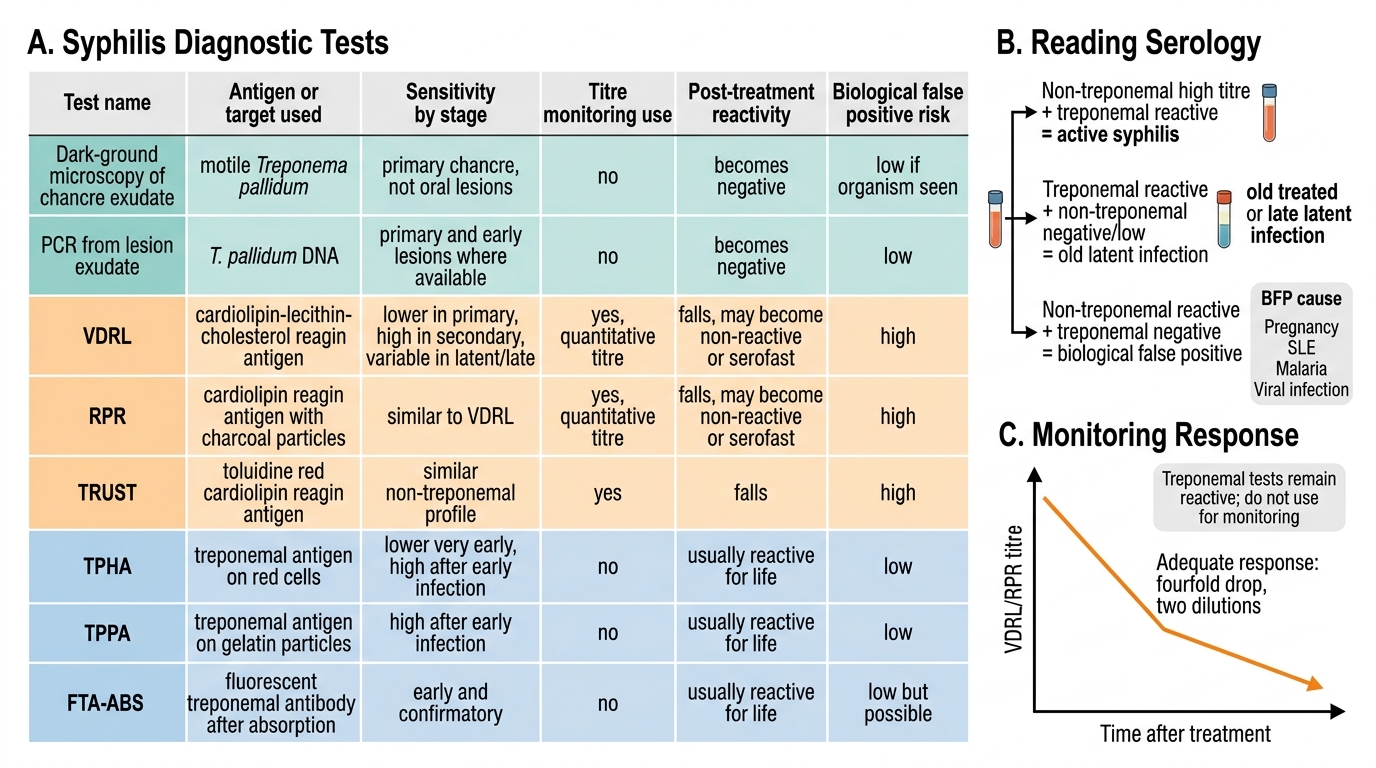
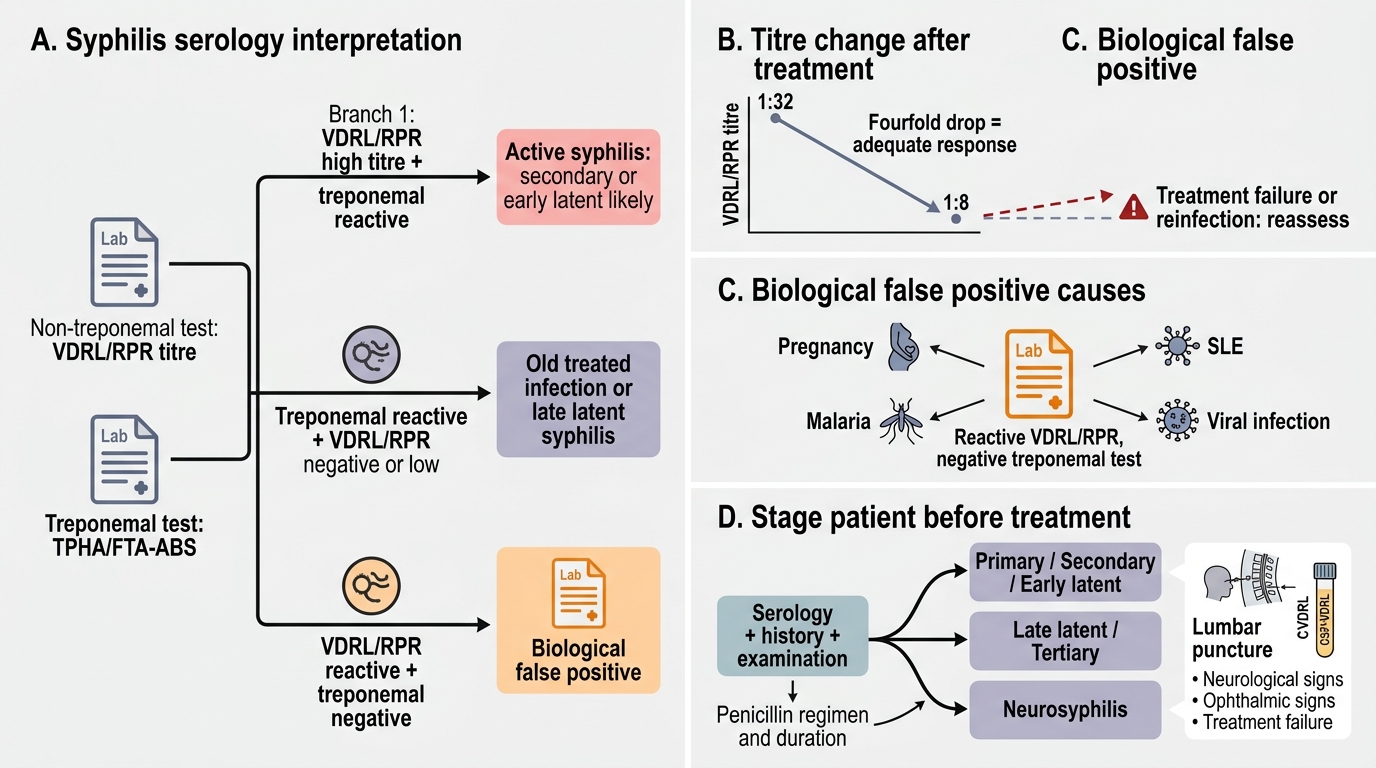
Interpreting serology correctly is where diagnosis becomes management, because the titre and the test combination tell you the stage and the next step. A high non-treponemal titre (for example VDRL reactive at 1:32) with a reactive treponemal test in an untreated patient indicates active syphilis — most often secondary or early latent disease — and a falling titre after treatment (conventionally a fourfold, i.e. two-dilution, drop) signals an adequate response. A reactive treponemal test with a negative or low non-treponemal test suggests old, treated, or late latent infection, because the treponemal antibody persists while the non-treponemal marker of activity has waned. A reactive non-treponemal test with a negative treponemal test is the signature of a biological false positive — investigate the BFP causes (pregnancy, SLE, malaria, viral infection) rather than diagnosing syphilis. When neurosyphilis is suspected — neurological or ophthalmic signs, or treatment failure — a lumbar puncture for CSF examination (including CSF-VDRL) is indicated, because the choice of regimen changes for neurosyphilis.
This interpretive step is the bridge to treatment, which the next SDL covers in full: the stage you assign — primary/secondary/early latent versus late latent/tertiary versus neurosyphilis — directly selects the penicillin regimen and its duration. Diagnosis is not complete until you have placed the patient on the staging spectrum.
Syphilis Serology Interpretation Algorithm
- High non-treponemal titre + reactive treponemal (untreated) → active disease; fourfold titre fall = adequate response.
- Reactive treponemal + low/negative non-treponemal → old/treated/late latent.
- Reactive non-treponemal + negative treponemal → biological false positive; LP/CSF-VDRL if neurosyphilis suspected.
SELF-CHECK
A non-pregnant patient has a VDRL reactive at 1:2 but an FTA-ABS that is non-reactive. What is the most likely explanation?
A. Active secondary syphilis requiring immediate treatment
B. A biological false positive — the treponemal test is negative, so true syphilis is unlikely; investigate causes such as autoimmune disease, recent infection, or pregnancy
C. Neurosyphilis, which always gives this pattern
D. Successfully treated tertiary syphilis
Reveal Answer
Answer: B. A biological false positive — the treponemal test is negative, so true syphilis is unlikely; investigate causes such as autoimmune disease, recent infection, or pregnancy
A reactive non-treponemal test (VDRL) with a negative treponemal test (FTA-ABS) is the classic pattern of a biological false positive. Treponemal tests are specific confirmatory tests; a negative result makes true syphilis unlikely, so causes of biological false positives (pregnancy, SLE, malaria, other infections) should be sought.
Self-Assessment — Syphilis Diagnostic Scenarios
Consolidate your diagnostic reasoning with these scenarios, and in each force yourself to state which feature or test result drives the conclusion. First, distinguish the stages from morphology: a painless indurated genital ulcer is primary; a palmoplantar rash with mucous patches and condyloma lata is secondary; positive serology with no signs is latent; and gummata, aortitis, or an Argyll Robertson pupil are tertiary. Second, choose the right test for the situation: dark-ground microscopy for the exudate of a fresh chancre (never for an oral lesion), a non-treponemal test (VDRL/RPR) to screen and to monitor by titre, and a treponemal test (TPHA/FTA-ABS/TPPA) to confirm. Third, interpret discordant serology: a reactive non-treponemal with a negative treponemal test is a biological false positive, not syphilis — a point that recurs in antenatal screening, where pregnancy itself can cause a false-positive non-treponemal test.
For each self-check, link the finding to the next action: which test to order, what the titre means for monitoring, and which stage you would assign — because that stage is what the treatment SDL will use to pick the penicillin regimen.
- Read the stage from morphology and serology together.
- Match the test to the question: DGM (organism), non-treponemal (screen/monitor), treponemal (confirm).
- A reactive non-treponemal with a negative treponemal test is a biological false positive.
SELF-CHECK
Which is the appropriate bedside test to demonstrate the organism directly from the exudate of a fresh genital chancre?
A. VDRL on serum
B. Dark-ground microscopy of the chancre exudate
C. TPHA on serum
D. Tzanck smear of the ulcer base
Reveal Answer
Answer: B. Dark-ground microscopy of the chancre exudate
Dark-ground microscopy of fresh exudate from a genital chancre directly demonstrates motile Treponema pallidum and is highly specific in early syphilis. VDRL and TPHA are serological (antibody) tests, and the Tzanck smear is used for herpes (multinucleated giant cells), not syphilis. Note dark-ground microscopy is not valid on oral lesions because of commensal treponemes.
CLINICAL PEARL
Hold two facts together and most syphilis serology becomes easy to read. Non-treponemal tests (VDRL/RPR) track disease activity — their titre rises with active infection and falls with successful treatment, which is exactly why they are used both to screen and to monitor cure. Treponemal tests (TPHA/FTA-ABS/TPPA) track ever-having-been-infected — once positive they usually stay positive for life, so they confirm the diagnosis but tell you nothing about activity or response. A reactive non-treponemal test with a negative treponemal test is therefore not syphilis but a biological false positive — think pregnancy, SLE, malaria, or recent viral infection.