Page 10 of 35
DR10.6 | Syphilis Treatment Workflow — SDL Guide
Learning Objectives
- Identify the clinical and serological triggers for initiating syphilis treatment.
- Explain why penicillin is first-line and why short-acting forms are inadequate for early syphilis.
- Select the correct benzathine penicillin G regimen by stage, including neurosyphilis, pregnancy, and congenital syphilis.
- Manage genital ulcer disease within the NACO syndromic framework (Kit 3 for non-herpetic GUD).
- Monitor treatment response by VDRL titre and recognise and manage the Jarisch-Herxheimer reaction.
INSTRUCTIONS
Syphilis is one of the few serious infections with a simple, cheap, and reliably effective cure — benzathine penicillin G — provided you match the regimen to the stage and handle a few special situations correctly. This module turns the diagnosis you made in the previous SDL into a treatment workflow: which dose for which stage, what to do in pregnancy and in the newborn, and how to monitor that the treatment has worked.
References
- NACO National Guidelines on Prevention, Management and Control of RTI/STI, Ministry of Health & Family Welfare, Government of India (textbook)
- Neena Khanna, Illustrated Synopsis of Dermatology and Sexually Transmitted Diseases, Ch. on Syphilis (treatment) (textbook)
- IADVL Textbook of Dermatology, Ch. on Syphilis and WHO Guidelines for the Treatment of Treponema pallidum (Syphilis) (textbook)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
A pregnant woman attends her first antenatal visit and her routine VDRL comes back reactive. Untreated, her syphilis can cause stillbirth, prematurity, or a baby born with congenital syphilis — a tragedy that is almost entirely preventable. The treatment is a single intramuscular injection of benzathine penicillin G that costs very little and works reliably. The only thing standing between this mother and a healthy baby is a clinician who knows the right drug, the right dose for her stage, and what to do if she happens to be allergic to penicillin. Treating syphilis correctly is one of the highest-yield, lowest-cost interventions in all of clinical medicine.
WHY THIS MATTERS
You will treat syphilis far more often than you might expect — in antenatal clinics where universal screening catches asymptomatic maternal infection, in STI clinics, and whenever a contact of a confirmed case presents. The stakes of getting it right are high: a correct, stage-appropriate regimen cures the patient and, in pregnancy, protects the fetus; an incorrect one (the wrong duration, a non-penicillin drug in pregnancy, or benzathine penicillin mistakenly used for neurosyphilis) risks treatment failure and serious complications. You must also be able to reassure a patient through the Jarisch-Herxheimer reaction without abandoning a curative drug, and to manage a genital ulcer syndromically when definitive diagnosis is not yet available. This is practical, examinable, and life-saving knowledge.
RECALL
Recall what the previous SDL established, because treatment depends entirely on it. You learned to stage syphilis — primary, secondary, early latent (within two years), late latent or tertiary (over two years), neurosyphilis, and congenital — and to read serology, using the non-treponemal VDRL/RPR titre as the marker of disease activity that falls with successful treatment. You also know from pharmacology that penicillins are beta-lactam antibiotics that inhibit bacterial cell-wall synthesis, and that benzathine penicillin is a long-acting (depot) form that maintains low blood levels for weeks. Hold these together: the stage tells you the regimen, and the VDRL titre tells you whether it worked.
Presentations That Demand Syphilis Treatment — Clinical and Serological Triggers
Syphilis Treatment Triggers
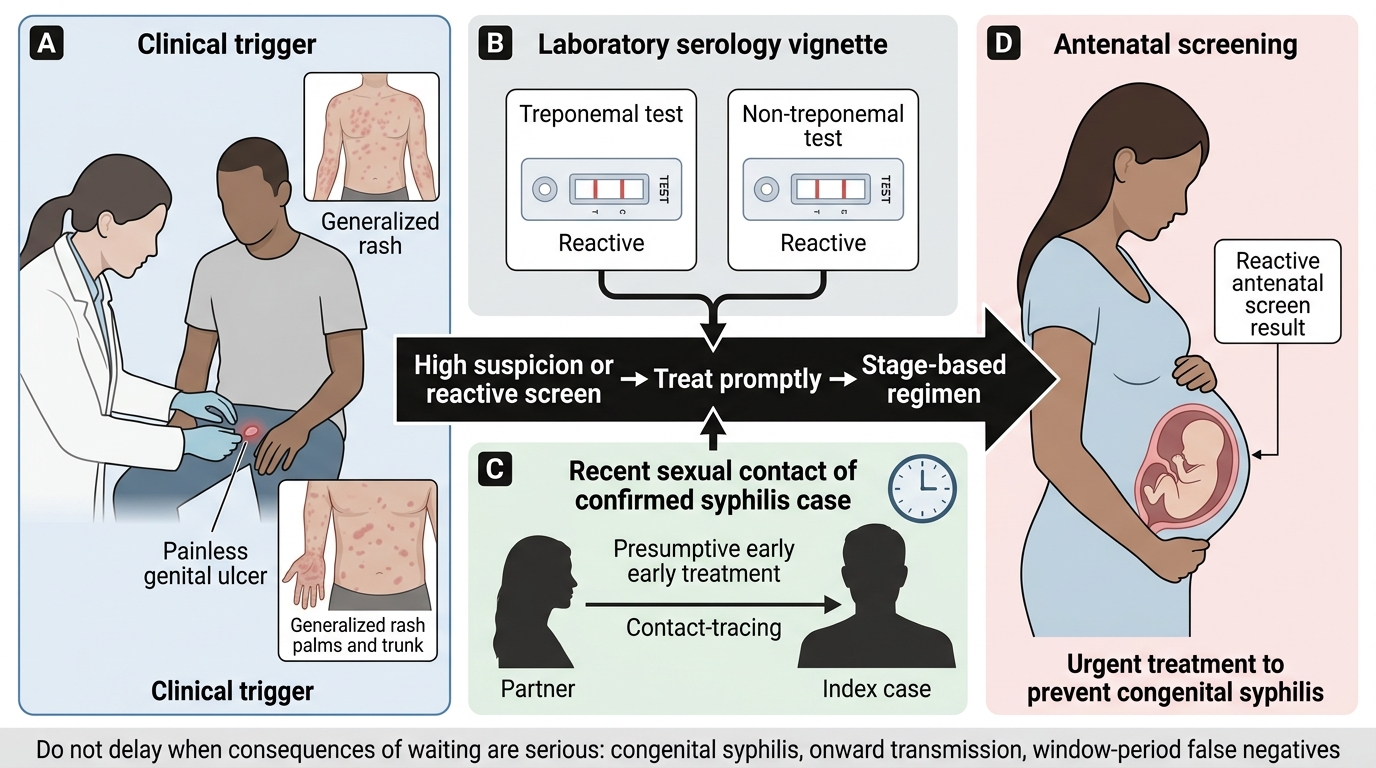
Treatment is triggered by recognisable clinical and serological situations, and recognising them — and not delaying — is the first competency. You treat the patient with a clinically diagnosed primary chancre or the unmistakable features of secondary syphilis; you treat the patient whose serology is reactive on the appropriate combination of tests; you treat, presumptively, the recent sexual contact of a confirmed case even before their own serology returns, because early treatment prevents both disease and onward transmission; and you treat the pregnant woman whose antenatal screen is reactive, urgently, because every week of delay increases fetal risk. In each of these the principle is the same: where the clinical index of suspicion is high and the consequences of waiting are serious, you do not withhold curative treatment pending every confirmatory result.
This bias toward timely treatment is not carelessness but sound public-health and clinical reasoning. Syphilis is curable, the drug is safe and cheap, the complications of delay (congenital syphilis, ongoing transmission) are severe, and the diagnostic tests have window periods and false negatives that can lull a clinician into inaction. The skill is to read the trigger — symptomatic case, reactive serology, exposed contact, or reactive antenatal screen — and to move to the correct stage-based regimen promptly.
- Treat: clinically diagnosed primary/secondary cases; serology-reactive cases; recent contacts (presumptively); reactive antenatal screens (urgently).
- Do not delay curative treatment pending every confirmatory result when suspicion is high.
- Each trigger leads to a stage-based regimen, not a one-size-fits-all dose.
How Penicillin Kills T. pallidum — Mechanism and Why Alternatives Are Limited
Why Penicillin Remains First-Line for Syphilis
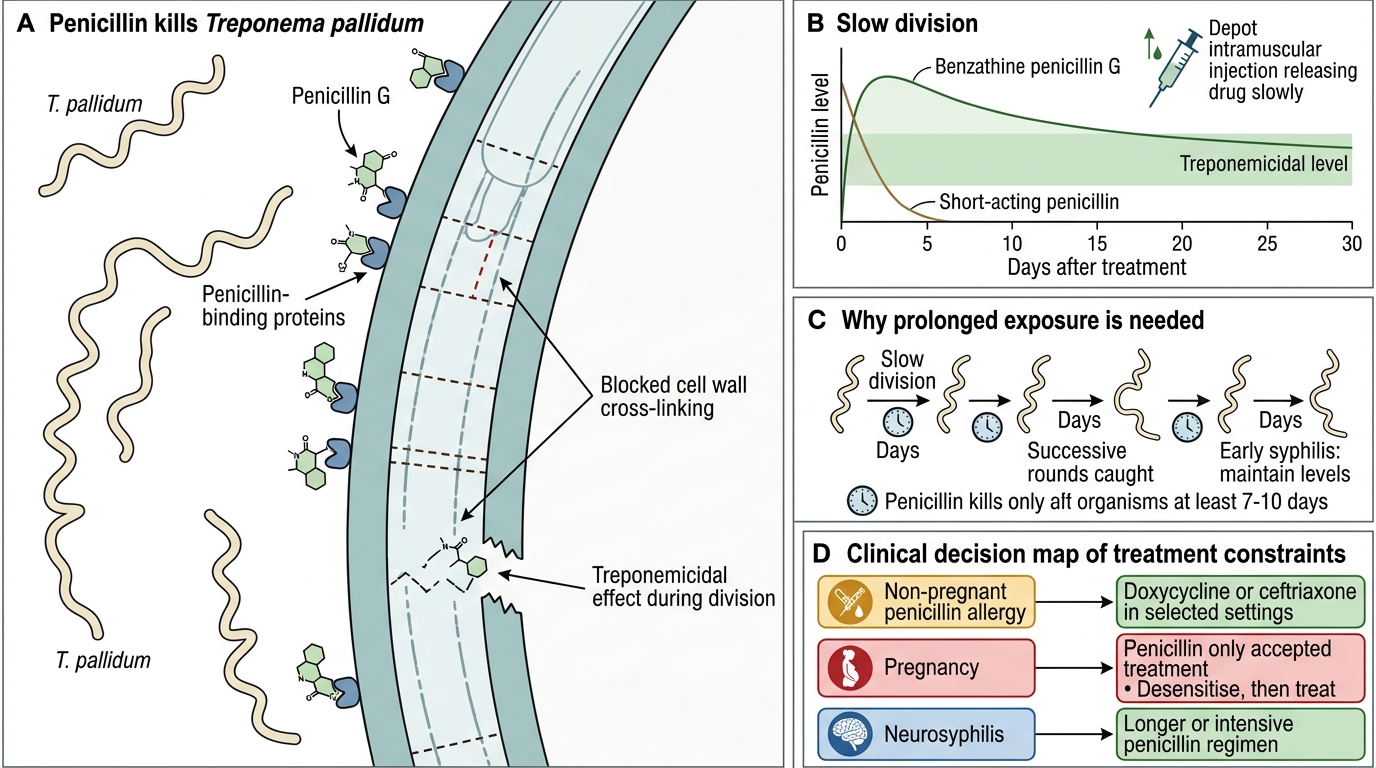
Penicillin remains first-line for syphilis after more than seventy years because Treponema pallidum has never developed clinically meaningful resistance to it, a remarkable fact in an age of widespread antimicrobial resistance. Benzathine penicillin G is a beta-lactam that binds penicillin-binding proteins and inhibits cross-linking of the bacterial cell wall, killing the organism. The catch is that T. pallidum divides very slowly, and penicillin only kills dividing organisms, so the drug must maintain treponemicidal levels continuously for many days — at least seven to ten days for early syphilis — to catch successive rounds of division. This is precisely why the long-acting depot benzathine form is used: a single intramuscular injection releases penicillin slowly and sustains adequate levels for weeks, whereas short-acting penicillin would clear too fast to be reliably curative. It is also why late and neurological disease need longer or more intensive regimens.
Alternatives are limited and each has a caveat. In genuine penicillin allergy in non-pregnant patients, doxycycline (or, in some settings, ceftriaxone) can be used. But in pregnancy penicillin is the only accepted treatment: doxycycline is contraindicated and other alternatives are not adequately proven to protect the fetus, so a penicillin-allergic pregnant woman must be desensitised to penicillin and then treated with it. For neurosyphilis, benzathine penicillin is inadequate because it does not achieve treponemicidal concentrations in cerebrospinal fluid, so intravenous aqueous crystalline penicillin G is required. Treatment of early syphilis may also provoke the Jarisch-Herxheimer reaction — a self-limiting febrile reaction caused by the sudden release of antigens from dying spirochaetes, not a drug allergy.
- T. pallidum has no meaningful penicillin resistance; benzathine penicillin G is first-line.
- The organism divides slowly, so sustained treponemicidal levels are needed — hence the long-acting depot form.
- Pregnancy → penicillin only (desensitise if allergic); neurosyphilis → IV aqueous penicillin (benzathine fails in CSF).
Stage-Based Treatment Regimens for Syphilis
Stage-Based Syphilis Treatment Regimens
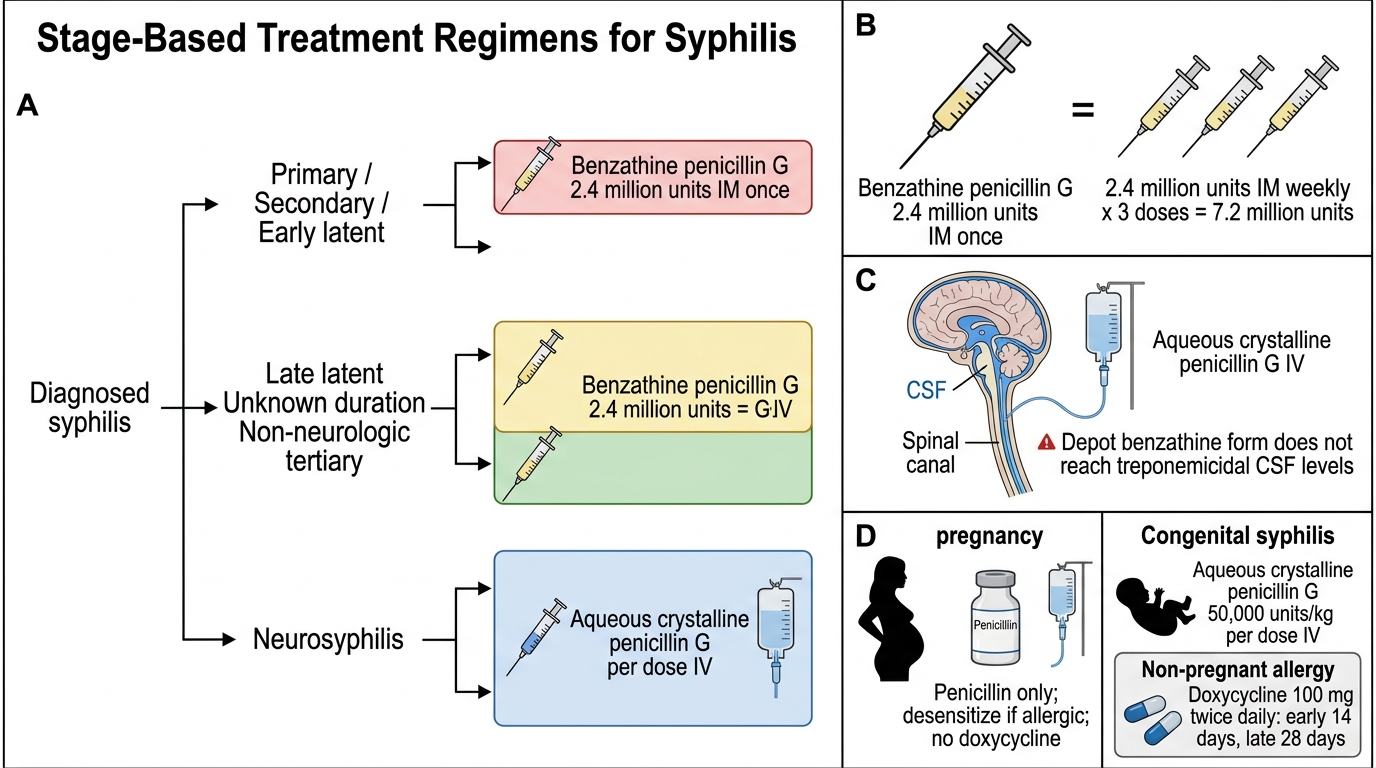
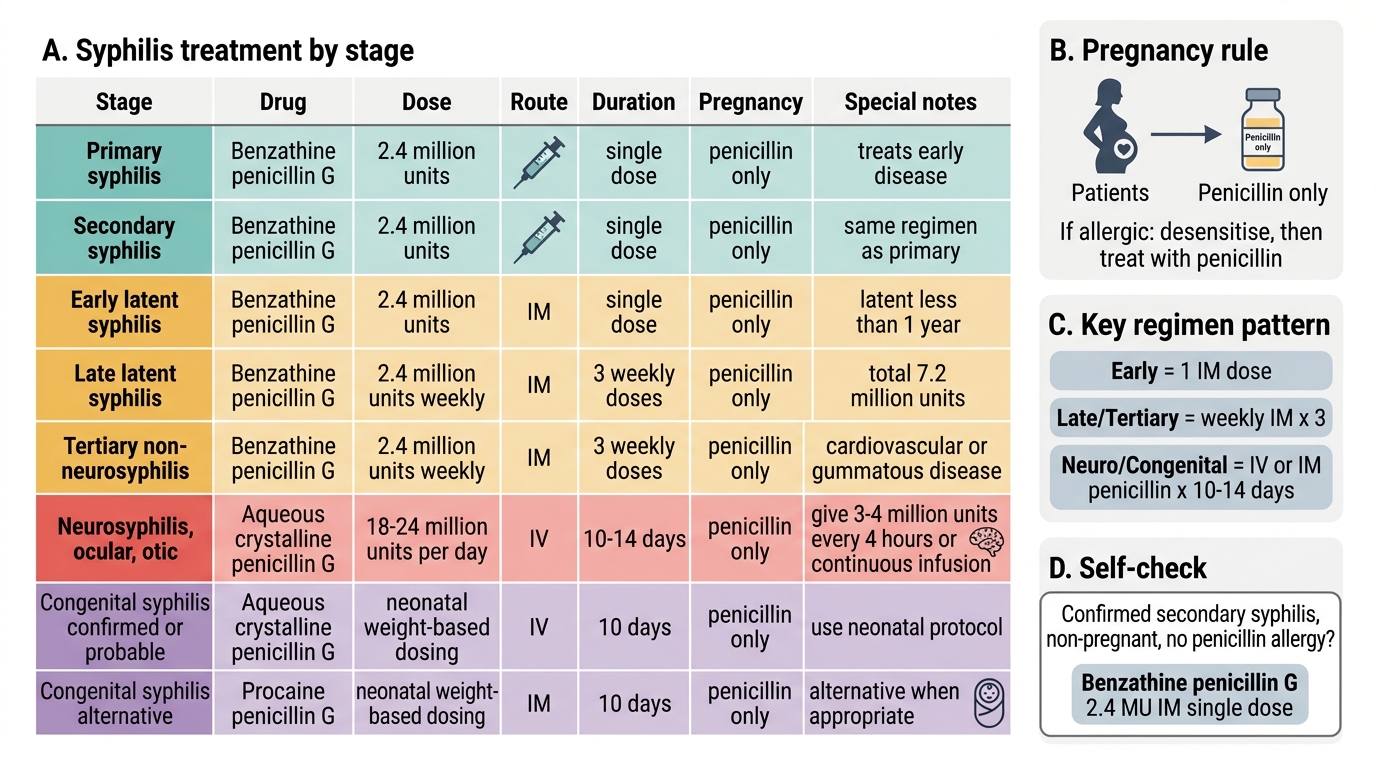
The core of treatment is matching the benzathine penicillin G regimen to the stage. For primary, secondary, and early latent syphilis (acquired within the preceding two years), the regimen is a single dose of benzathine penicillin G 2.4 million units intramuscularly. For late latent syphilis, latent syphilis of unknown duration, and tertiary syphilis that does not involve the nervous system, the regimen is benzathine penicillin G 2.4 million units intramuscularly given weekly for three doses (a total of 7.2 million units) — the longer course reflecting the slower, lower-burden nature of late disease. Neurosyphilis is the important exception: it requires aqueous crystalline penicillin G, 3–4 million units intravenously every four hours for ten to fourteen days, because the depot benzathine form does not reach treponemicidal levels in the CSF. In genuine penicillin allergy in non-pregnant patients, doxycycline 100 mg twice daily is used — for fourteen days in early syphilis and for twenty-eight days in late disease.
Two special populations must be handled exactly. In pregnancy, penicillin is the only accepted treatment for the stage; a penicillin-allergic pregnant woman is desensitised and then treated with penicillin, never substituted with doxycycline (which is fetotoxic). For congenital syphilis (proven or probable), the neonate is treated with aqueous crystalline penicillin G (50,000 units/kg per dose intravenously, every 12 hours in the first 7 days of life then every 8 hours, for a total of 10 days) or procaine penicillin G 50,000 units/kg intramuscularly once daily for 10 days. Note that NACO delivers benzathine penicillin G through its programme; confirm exact neonatal dosing against current national guidance.
Syphilis Treatment by Stage
- Primary/secondary/early latent → benzathine penicillin G 2.4 MU IM, single dose.
- Late latent / tertiary (non-neuro) → benzathine penicillin G 2.4 MU IM weekly × 3.
- Neurosyphilis → aqueous crystalline penicillin G IV; pregnancy → penicillin only (desensitise if allergic); congenital → aqueous/procaine penicillin × 10 days.
SELF-CHECK
What is the correct treatment for confirmed secondary syphilis in a non-pregnant patient with no penicillin allergy?
A. Benzathine penicillin G 2.4 million units IM, weekly for three doses
B. Benzathine penicillin G 2.4 million units IM as a single dose
C. Aqueous crystalline penicillin G 3–4 million units IV every 4 hours for 14 days
D. Doxycycline 100 mg twice daily for 28 days
Reveal Answer
Answer: B. Benzathine penicillin G 2.4 million units IM as a single dose
Secondary syphilis (like primary and early latent) is treated with a single dose of benzathine penicillin G 2.4 million units IM. The three-weekly-dose regimen is for late latent/tertiary disease; IV aqueous crystalline penicillin is for neurosyphilis; doxycycline is only an alternative in non-pregnant penicillin-allergic patients.