Page 3 of 12
DR14.1-2 | Urticaria Angioedema Classification and Management — SDL Guide (Part 3)
Investigations in Chronic Urticaria
Investigations in Chronic Urticaria
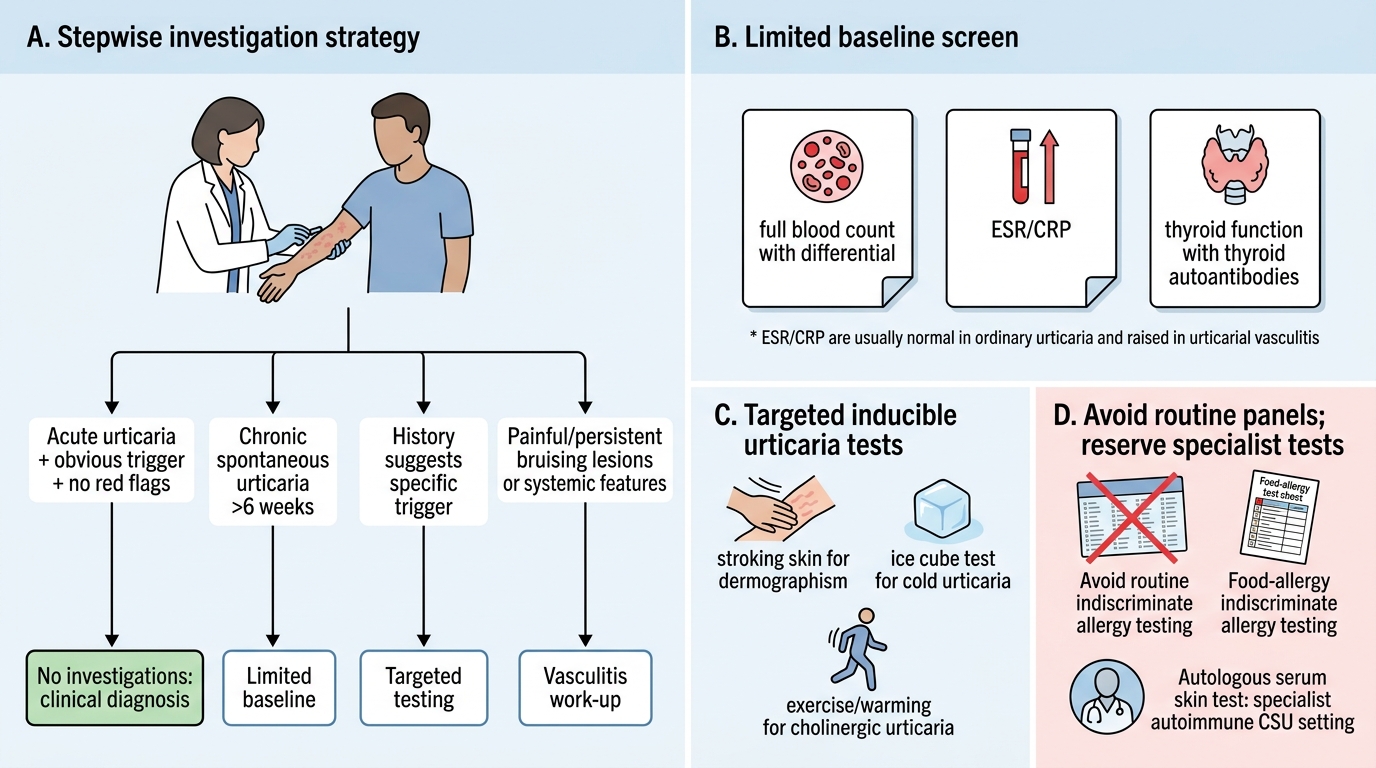
A common error in managing urticaria is to over-investigate the patient, ordering extensive allergy panels that rarely change management. The correct approach is targeted and stepwise, driven by the history and the suspicion of an alternative diagnosis rather than by routine. For acute urticaria with an obvious trigger and no red flags, no investigation is required — the diagnosis is clinical and the condition self-limiting. For chronic spontaneous urticaria, a limited baseline screen is reasonable to exclude a systemic contributor: a full blood count with differential (eosinophilia may suggest a parasitic or allergic cause), inflammatory markers (ESR/CRP — importantly, these are normal in ordinary urticaria and raised in urticarial vasculitis), and thyroid function with thyroid autoantibodies, given the recognised association with autoimmune thyroid disease. Routine, indiscriminate food-allergy testing is not recommended because results correlate poorly with clinical disease.
Where the history points to a specific cause, targeted testing is appropriate. Inducible urticarias are confirmed by reproducing the lesion with a controlled physical challenge — stroking the skin for dermographism, applying an ice cube for cold urticaria, or exercise/warming for cholinergic urticaria. Where chronic spontaneous urticaria is suspected to be autoimmune, an autologous serum skin test may be used in specialist settings. If any lesion behaves like vasculitis — persisting beyond 24 hours, painful, bruising — a skin biopsy and complement studies are indicated, and if recurrent angioedema occurs without wheals, C4 and C1-esterase inhibitor levels should be checked to exclude hereditary angioedema. The overarching rule is that investigation is for the atypical or refractory case; the typical case is diagnosed and treated on clinical grounds alone.
The investigation framework:
- Acute, clear trigger: no investigation.
- Chronic spontaneous baseline: FBC, ESR/CRP, TFT + thyroid autoantibodies.
- Inducible: physical challenge test (stroke, ice cube, exercise).
- Vasculitis suspicion: skin biopsy + complement (C3/C4).
- Angioedema without wheals: C4 and C1-esterase inhibitor levels (hereditary angioedema).
SELF-CHECK
A 62-year-old man on enalapril for hypertension develops recurrent episodes of deep swelling of the lips and tongue over several months. There are no itchy wheals, and oral cetirizine and prednisolone have produced no improvement. What is the most likely mechanism and the most appropriate first step?
A. IgE-mediated urticaria; increase the antihistamine dose to four times standard
B. Bradykinin-mediated angioedema due to the ACE-inhibitor; stop the enalapril, as this angioedema does not respond to antihistamines or steroids
C. Chronic spontaneous urticaria; start omalizumab immediately
D. Cholinergic urticaria; advise the patient to avoid hot showers
Reveal Answer
Answer: B. Bradykinin-mediated angioedema due to the ACE-inhibitor; stop the enalapril, as this angioedema does not respond to antihistamines or steroids
Recurrent deep angioedema without any wheals or itch, occurring in a patient on an ACE-inhibitor and failing to respond to antihistamines and corticosteroids, is the classic picture of bradykinin-mediated, ACE-inhibitor-induced angioedema. Because the swelling is driven by accumulation of bradykinin (whose breakdown the ACE-inhibitor blocks) and not by histamine, antihistamines and steroids are ineffective — a key point that explains the lack of response. The essential first step is to stop the ACE-inhibitor and switch to an alternative antihistensive class; the angioedema may take days to weeks to settle. Severe airway involvement is managed supportively, and specialist bradykinin-targeted therapies exist, but recognising the mechanism and withdrawing the offending drug is the decisive action.
Management: Stepwise Antihistamine-First Approach
Stepwise Antihistamine-First Management of Urticaria
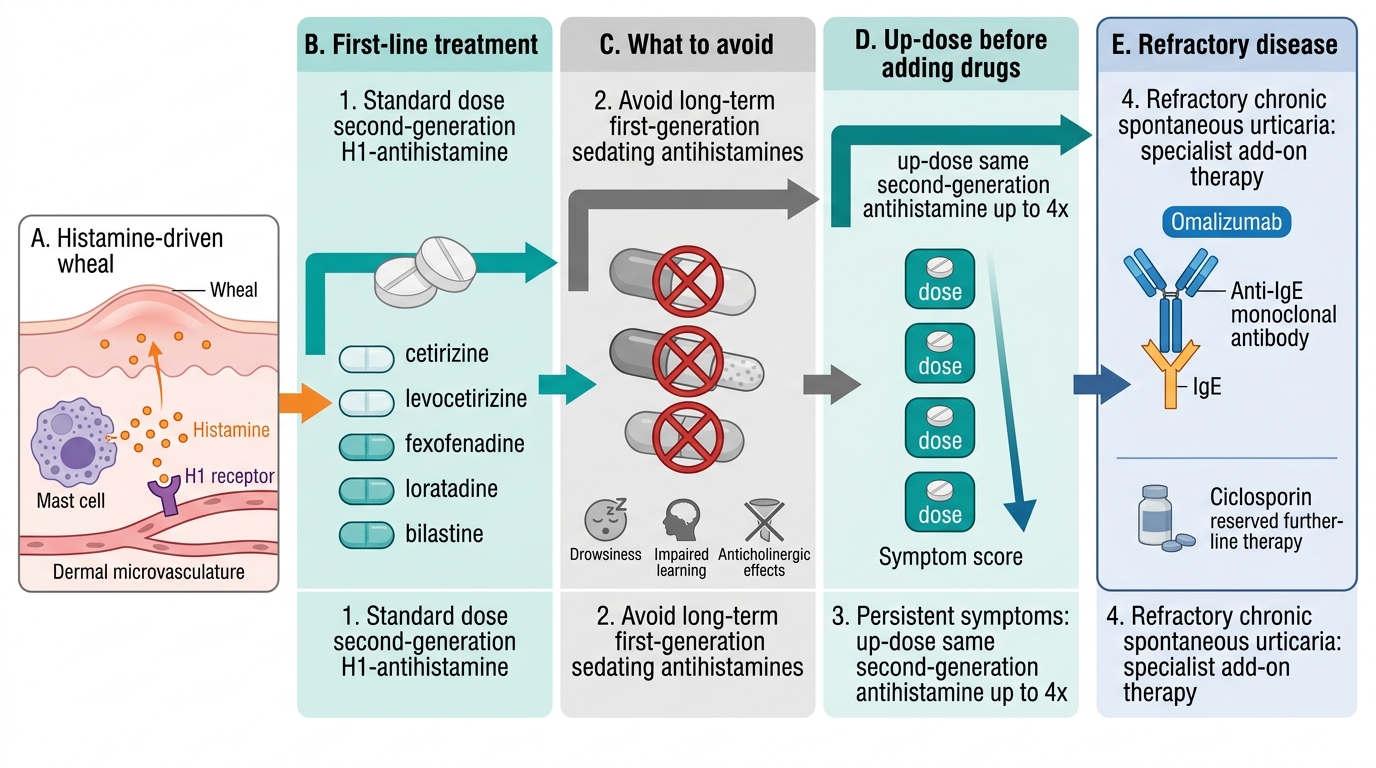
The management of urticaria follows a logical, guideline-based ladder that flows directly from the pathogenesis: because histamine acting on H1 receptors drives the wheal, the cornerstone of treatment is the H1-antihistamine, and the strategy is to start standard, then up-dose, then add specialist therapy for the refractory few. The recommended first-line agent is a second-generation, non-sedating H1-antihistamine — such as cetirizine, levocetirizine, fexofenadine, loratadine, or bilastine — given at the standard licensed dose. These are preferred over the older first-generation agents (chlorpheniramine, hydroxyzine, promethazine) because they control symptoms without the sedation and anticholinergic effects that impair learning, driving, and quality of life; first-generation sedating antihistamines should be avoided for long-term control. If symptoms persist on a standard dose, current guidelines recommend up-dosing the same second-generation antihistamine to as much as four times the standard dose before adding any further drug — a safe and effective step that many clinicians underuse.
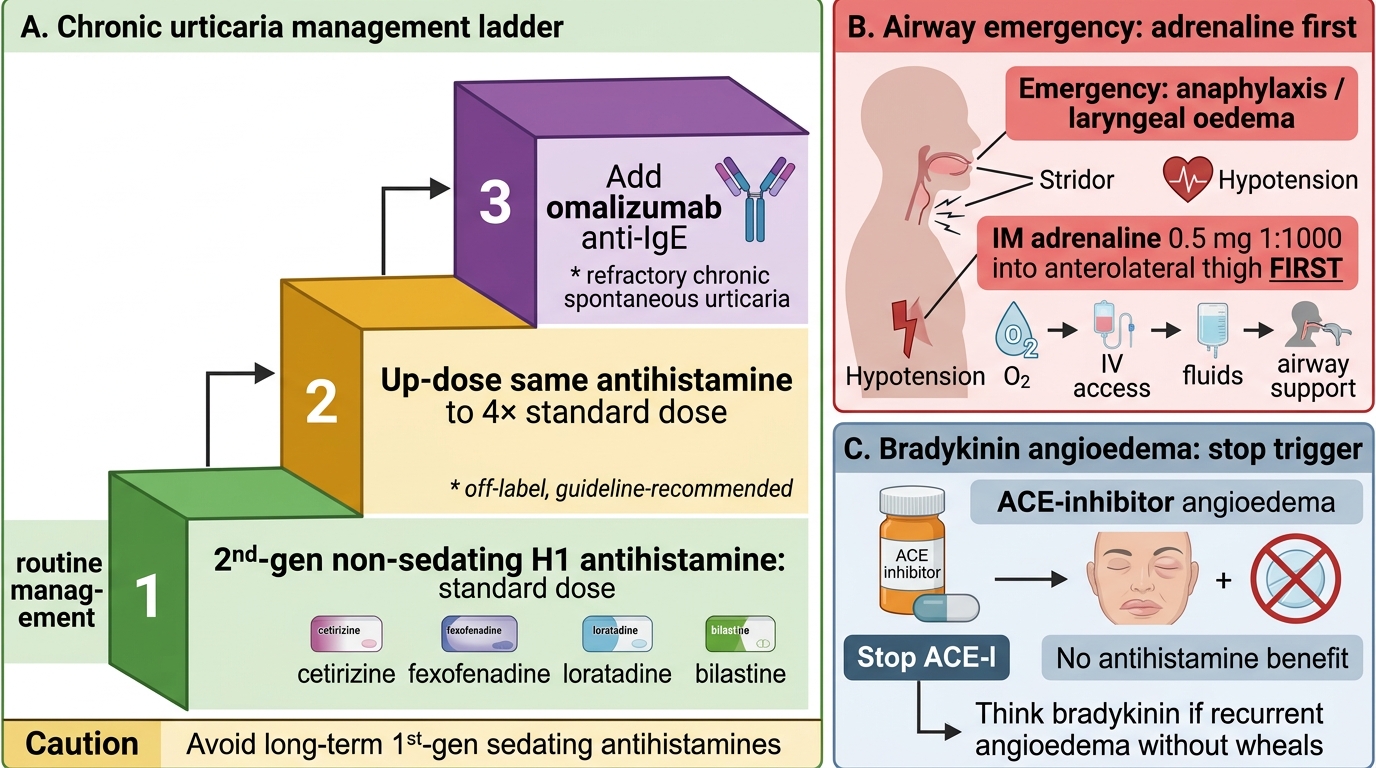
For the minority of patients with chronic spontaneous urticaria that remains refractory despite an up-dosed antihistamine, the recommended add-on is omalizumab, a monoclonal anti-IgE antibody, which is effective where antihistamines alone fail; other immunomodulators such as ciclosporin are reserved for further refractory disease under specialist care. A short course of oral corticosteroids may be used to settle a severe acute flare but is not a treatment for chronic disease. Separately and most importantly, angioedema with airway compromise or any feature of anaphylaxis is a medical emergency: the immediate treatment is intramuscular adrenaline (epinephrine), 0.5 mg of 1:1000 in an adult, repeated as needed, together with oxygen, intravenous fluids, and urgent airway assessment — antihistamines and steroids are adjuncts only and must never delay adrenaline. Finally, remember that bradykinin-mediated angioedema (ACE-inhibitor-induced or hereditary) does not respond to this histamine-directed ladder and requires drug withdrawal and specific therapy.
Urticaria and Angioedema Management Ladder
The management ladder at a glance:
- Step 1: second-generation non-sedating H1-antihistamine at standard dose.
- Step 2: up-dose the same antihistamine to up to 4× standard dose.
- Step 3 (refractory chronic spontaneous): add omalizumab (anti-IgE).
- Avoid: long-term first-generation sedating antihistamines.
- Emergency (airway angioedema/anaphylaxis): IM adrenaline 0.5 mg 1:1000 first, then O2, fluids, airway support.
- Bradykinin angioedema (ACE-I/HAE): withdraw the drug; histamine-directed therapy does not work.
CLINICAL PEARL
The most dangerous mistake in this topic is to reach for an antihistamine when the patient needs adrenaline. A patient whose tongue or larynx is swelling, who has stridor, breathlessness, or hypotension, is in (or heading towards) anaphylaxis — and the life-saving drug is intramuscular adrenaline, given immediately into the anterolateral thigh, not an antihistamine. The corollary mistake is the slow one: persisting with antihistamines and steroids in a patient with recurrent angioedema and no wheals, when the real diagnosis is bradykinin-mediated (ACE-inhibitor or hereditary) angioedema that will never respond to histamine-directed drugs. Two simple questions resolve both traps — 'Is the airway threatened?' (if yes, adrenaline now) and 'Are there wheals and itch?' (if no, think bradykinin and stop the ACE-inhibitor).
Self-Assessment
Before moving on, test whether you can apply — not just recall — the framework of this module, because the difference between knowing the facts and using them safely is exactly what these self-check questions probe. Work through each scenario below and commit to an answer before reading on; the goal is to rehearse the clinical decisions you will actually face, not to memorise isolated facts. Pay particular attention to the two highest-stakes judgements: distinguishing a transient wheal from a persistent vasculitic lesion, and recognising the angioedema that needs adrenaline rather than an antihistamine. If you find yourself hesitating on the mechanism behind ACE-inhibitor angioedema or on the order of the treatment ladder, return to the relevant section before attempting the cluster quiz.
Self-check questions to attempt:
1. State the maximum duration of an individual urticarial wheal, and name the condition you must suspect when a lesion outlasts it.
2. Classify urticaria along its two axes, giving the duration cut-off and at least three inducible subtypes.
3. Explain why an ACE-inhibitor causes angioedema and why antihistamines do not help it.
4. List the management ladder for chronic spontaneous urticaria from first-line to refractory add-on.
5. State the single first drug, dose, and route for angioedema with airway compromise.