Page 1 of 22
DR8.1 | Common Viral Skin Infection Foundations — SDL Guide
Learning Objectives
- Describe the major virus families that infect human skin — Herpesviridae (HSV, VZV), Papillomaviridae (HPV) and Poxviridae (molluscum contagiosum virus) — and their aetiology
- Explain the pathogenesis common to each family, including herpesvirus latency and reactivation, HPV keratinocyte infection, and poxvirus cytoplasmic replication
- Recognise the family-level morphological signatures of common cutaneous viral infections in adults and children
- Outline the diagnostic approach and the management principles that apply across cutaneous viral infections
INSTRUCTIONS
Viral infections of the skin are among the commonest dermatological presentations you will meet in outpatient practice, in children and adults alike. Before you can confidently identify a specific entity — a cold sore, shingles, a wart, or a cluster of umbilicated papules — you need an organising framework: which virus families infect skin, how each behaves biologically, and what visual signature each leaves. This foundational SDL builds that map. It deliberately stays at the family and organising level; the focused recognition SDLs that follow (herpes simplex, varicella zoster, viral warts, molluscum contagiosum) drill into each entity in detail.
References
- Khanna N. Illustrated Synopsis of Dermatology & Sexually Transmitted Diseases, 6th ed. Ch: Viral Infections (textbook)
- Sacchidanand S (ed). IADVL Textbook of Dermatology, 4th ed. Section: Viral Infections of the Skin (textbook)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
A 6-year-old is brought to your clinic with a crop of small, dome-shaped bumps on his trunk; the same week, his grandmother attends with a painful, blistering rash running in a band across one side of her chest; and his father asks you about a rough growth on his finger that will not go away. Three patients, one family, three different viruses — a poxvirus, a herpesvirus and a papillomavirus — each leaving a distinct mark on the skin. Telling them apart, and knowing which needs an antiviral, which needs only reassurance, and which needs a minor procedure, begins with understanding the small number of virus families that infect human skin.
WHY THIS MATTERS
Cutaneous viral infections are a daily reality in Indian outpatient dermatology and general practice. They affect every age group, several are contagious within households and schools, some signal underlying immunosuppression such as HIV, and a few (herpes zoster, disseminated herpes) can cause real morbidity if missed or mistreated. As a final-year student and future intern, you will be expected to recognise these conditions on sight, reassure or treat appropriately, and know when antiviral therapy genuinely changes outcome versus when it adds cost without benefit. Building the family-level framework now means each specific entity you study next slots into place rather than being memorised in isolation.
RECALL
Recall from your first-year Microbiology and Physiology: viruses are obligate intracellular parasites that hijack host-cell machinery to replicate. DNA viruses — which include all three families relevant here — typically replicate using host nuclear enzymes (herpesviruses, papillomaviruses) or, unusually, entirely in the cytoplasm (poxviruses, which carry their own replication enzymes). Recall too the concept of cell-mediated immunity (CMI): T-lymphocyte responses that control intracellular pathogens. When CMI wanes — with ageing, HIV infection, malignancy or immunosuppressive drugs — latent viruses can reactivate and infections become more extensive. Keep these two ideas — where a virus replicates and how immunity contains it — in mind as you map the families below.
How Viruses Infect the Skin: An Orienting Overview
Provided image
The skin is both a barrier against viruses and, once that barrier is breached, a tissue in which viruses replicate and display characteristic patterns. Only a small number of DNA virus families account for the great majority of cutaneous viral infections you will encounter, and each leaves a recognisable morphological signature that, with practice, allows a confident bedside diagnosis. Organising these infections by virus family — rather than memorising each as an unrelated entity — is the single most useful framework for recognition, because members of a family share pathogenesis, diagnostic clues and treatment logic. A virus that establishes latency in a nerve ganglion will behave, recur and be treated quite differently from one that merely proliferates in the surface epidermis, and knowing which family you are dealing with immediately narrows both the differential and the next step. The same framework also tells you when a lesion is contagious, when it might signal underlying immunosuppression, and when an antiviral will or will not change the outcome.
Three families dominate cutaneous viral disease:
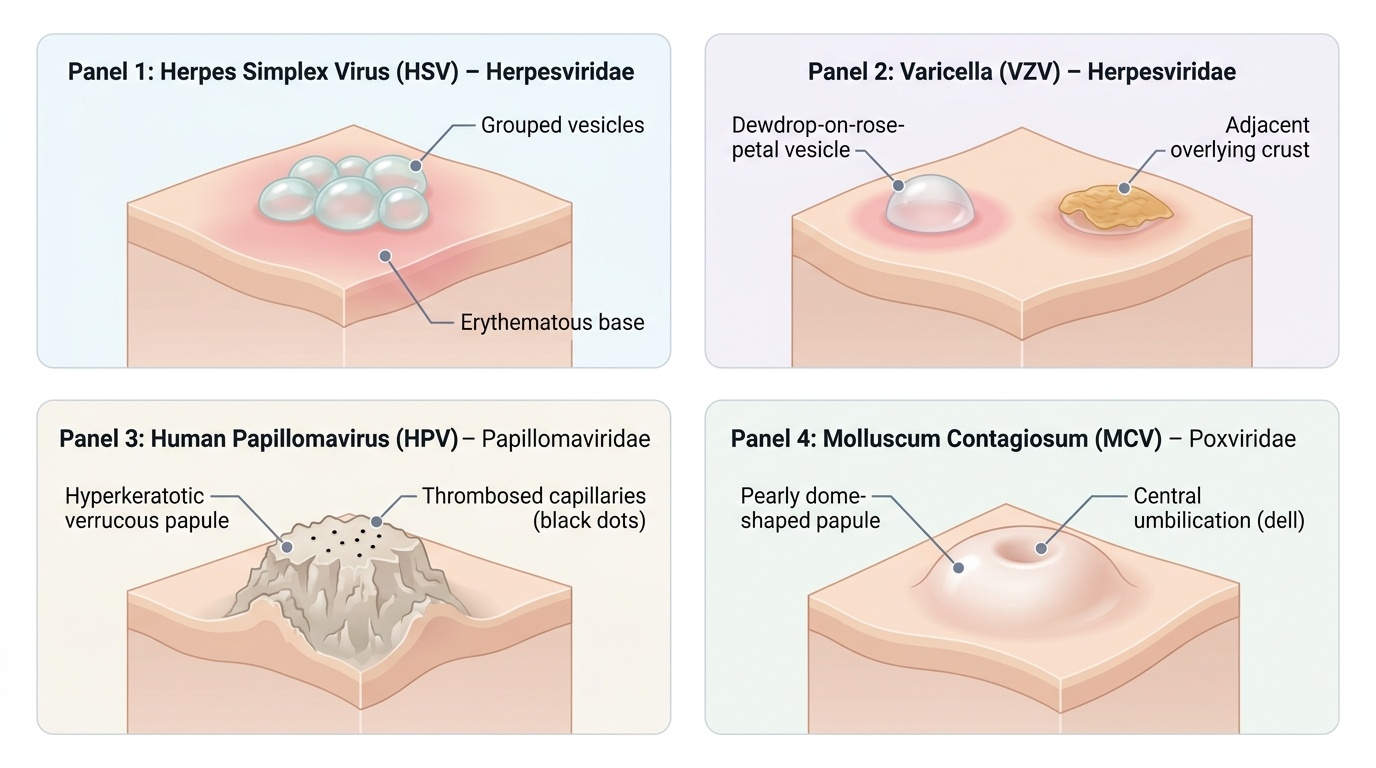
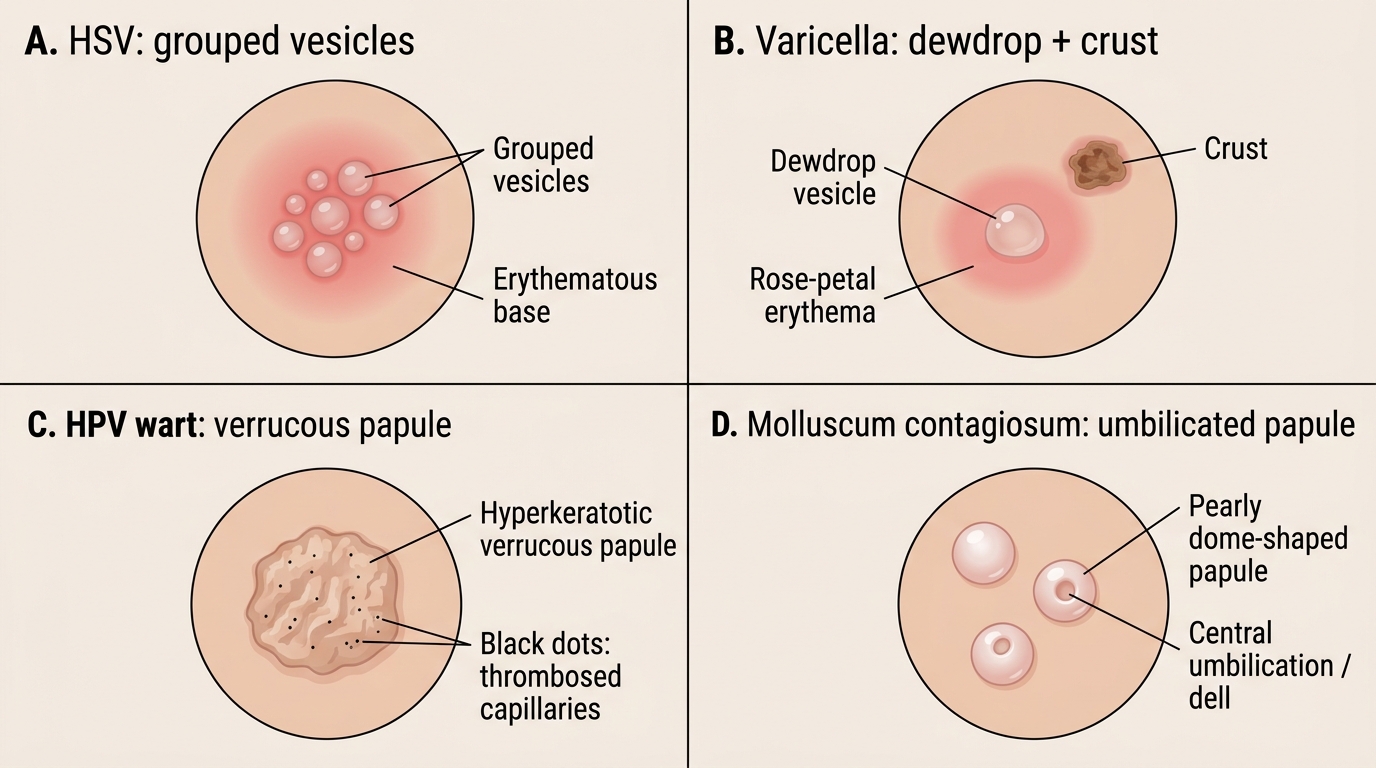
- Herpesviridae — enveloped DNA viruses that establish lifelong latency in sensory ganglia and periodically reactivate. The skin-relevant members are herpes simplex virus (HSV) types 1 and 2, and varicella zoster virus (VZV). Their signature lesion is the grouped vesicle on an erythematous base.
- Papillomaviridae — non-enveloped DNA viruses; human papillomavirus (HPV) infects keratinocytes and drives them to proliferate, producing warts (verrucae). The signature is a hyperkeratotic, verrucous papule, often with tiny black dots (thrombosed capillaries).
- Poxviridae — large DNA viruses that replicate entirely in the cytoplasm; the skin-relevant member is molluscum contagiosum virus (MCV). The signature is a pearly, dome-shaped papule with a central dimple (umbilication).
Keeping these three families and their visual signatures in mind turns a confusing array of skin lesions into a short, structured differential.
Viral Skin Lesion Morphologies
Herpesviruses: Pathogenesis, Latency and Reactivation
Herpesvirus Latency and Reactivation
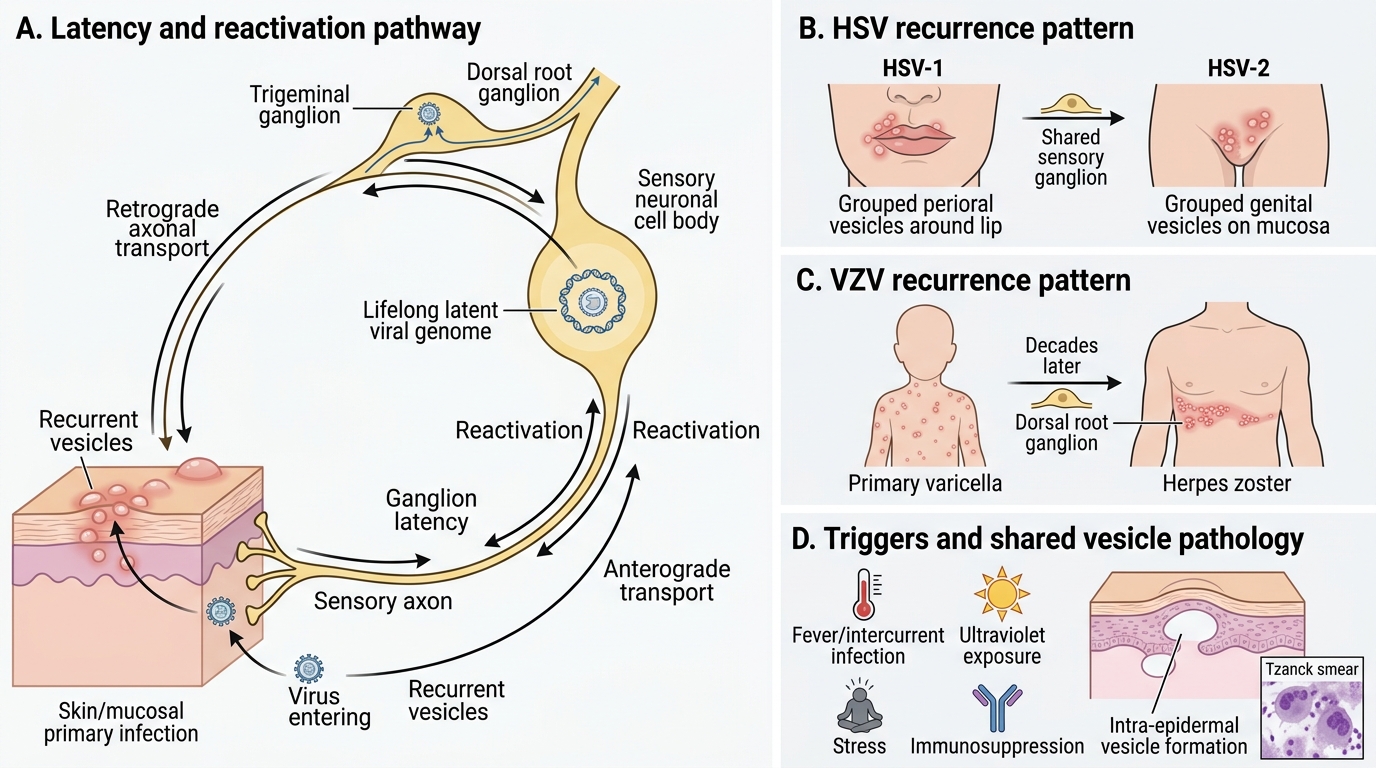
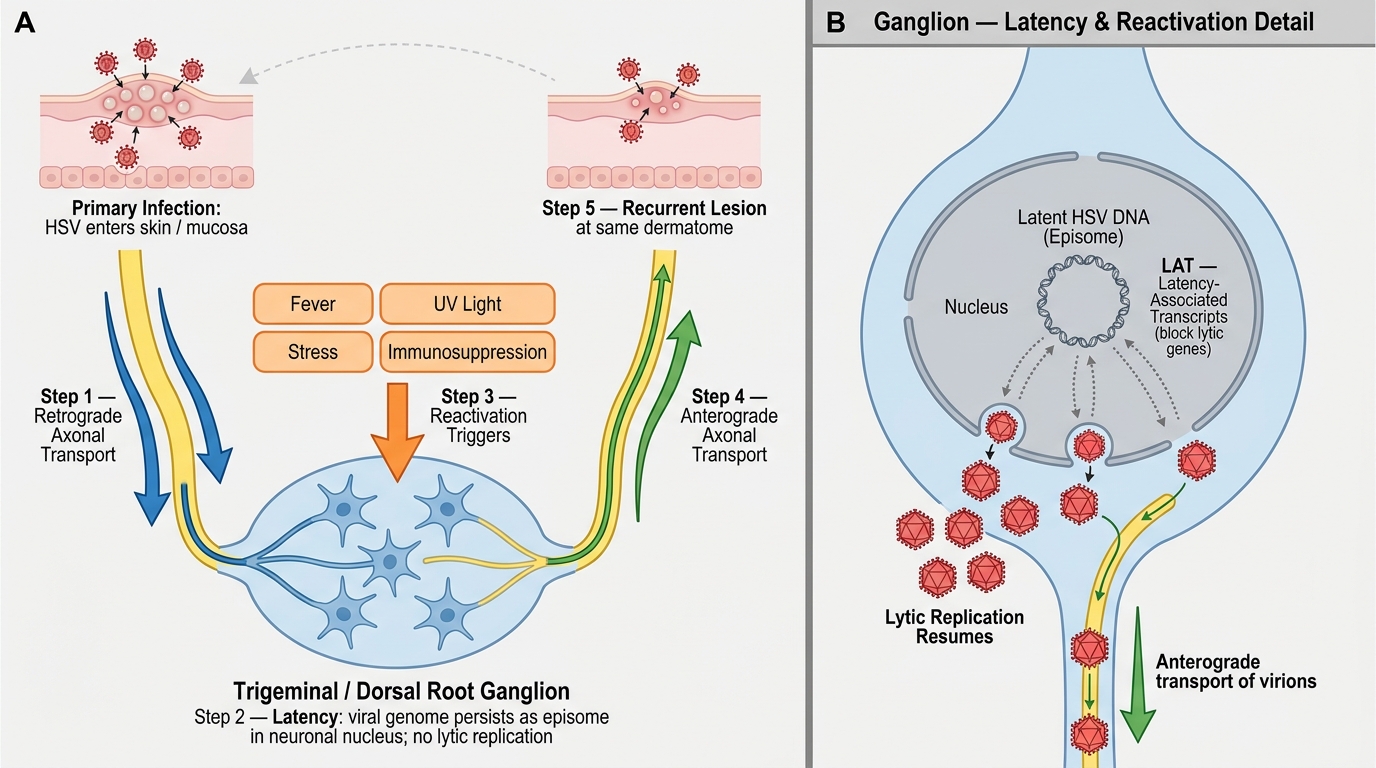
The defining behaviour of the herpesviruses is latency followed by reactivation, and understanding this single mechanism explains the entire clinical pattern of recurrent cold sores and of shingles. After a primary infection at the skin or mucosa, herpesviruses travel along sensory nerve axons to the cell bodies in the dorsal root or trigeminal ganglia, where the viral genome persists silently for life. The virus is not eradicated by the immune system; it is merely held in check. When local or systemic factors lower immune surveillance, the virus reactivates, travels back down the nerve to the skin, and produces a recurrent lesion in the territory that nerve supplies.
For HSV, primary infection is often subclinical; reactivation produces the familiar recurrent grouped vesicles — perioral for HSV-1 (herpes labialis) and genital for HSV-2. For VZV, primary infection is varicella (chickenpox) — a widespread eruption — after which the virus lies latent in dorsal root ganglia; decades later, reactivation produces herpes zoster (shingles), confined to the dermatome of the affected ganglion.
Key reactivation triggers, shared across herpesviruses, include:
- Fever and intercurrent infection
- Ultraviolet (sun) exposure
- Emotional or physical stress
- Immunosuppression — HIV, malignancy, chemotherapy, ageing
Because both HSV and VZV produce intra-epidermal vesicles by the same mechanism, a Tzanck smear from the base of a fresh vesicle shows multinucleate giant cells in both — a shared clue that confirms a herpesvirus but does not distinguish HSV from VZV (that requires PCR or direct fluorescent antibody testing).
HSV Lifecycle: Primary Infection, Ganglionic Latency, and Reactivation
SELF-CHECK
A Tzanck smear taken from the floor of a fresh vesicle shows multinucleate giant cells. What does this result tell you?
A. It confirms human papillomavirus infection
B. It confirms a herpesvirus (HSV or VZV) but cannot distinguish between them
C. It confirms molluscum contagiosum by showing Henderson-Paterson bodies
D. It excludes all viral causes and points to a bacterial infection
Reveal Answer
Answer: B. It confirms a herpesvirus (HSV or VZV) but cannot distinguish between them
Multinucleate giant cells on a Tzanck smear are the cytological hallmark of herpesvirus infection and are seen in both herpes simplex and varicella zoster lesions. The test confirms a herpesvirus is present but cannot tell HSV apart from VZV, nor HSV-1 from HSV-2 — that distinction requires PCR or direct fluorescent antibody (DFA) testing. The Tzanck smear is negative in HPV warts and in molluscum contagiosum (where the relevant finding is Henderson-Paterson cytoplasmic inclusion bodies, not giant cells).
HPV and Poxvirus: Pathogenesis Mechanisms
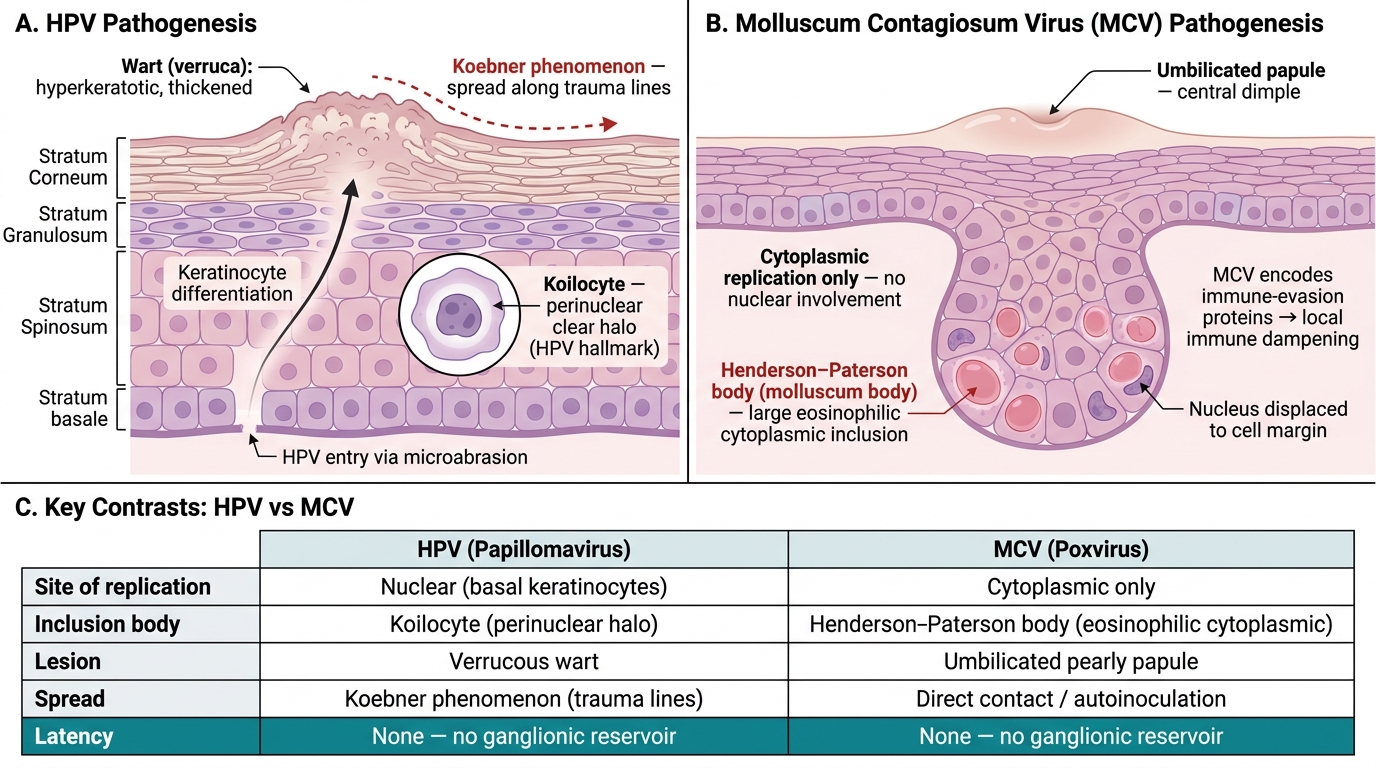
HPV and Molluscum Contagiosum Virus: Epidermal Pathogenesis Compared
Unlike the herpesviruses, neither HPV nor molluscum contagiosum virus establishes latency in nerve ganglia; both infect the epidermis locally and produce their lesions by directly altering keratinocyte behaviour. Recognising that these two families do not reactivate from a distant reservoir explains why their lesions are fixed in place and why they spread by direct contact and autoinoculation rather than by recurrence in a nerve territory.
Human papillomavirus (HPV) enters basal keratinocytes through tiny breaks in the skin. As infected cells differentiate and move toward the surface, the virus drives them to proliferate, producing the thickened, hyperkeratotic, verrucous lesion we call a wart. The histological hallmark is the koilocyte — a keratinocyte with a perinuclear clear halo. Because the virus is shed from the lesion surface and re-enters through new abrasions, warts characteristically spread along lines of trauma, an example of the Koebner phenomenon.
Molluscum contagiosum virus (MCV), a poxvirus, replicates entirely within the cytoplasm of keratinocytes, producing large eosinophilic cytoplasmic inclusion bodies called Henderson-Paterson (molluscum) bodies — distinct from the intranuclear inclusions of herpesviruses. The infected cells form a discrete pearly papule with a characteristic central dimple. MCV encodes proteins that locally dampen the immune response, which is why lesions can persist for months and why they become extensive in immunocompromised hosts.
The practical contrasts to carry forward are:
- No ganglion latency for either — lesions are local and spread by contact/autoinoculation, not nerve-territory recurrence.
- HPV → keratinocyte proliferation → verrucous papule with thrombosed capillaries; koilocytes on histology.
- MCV → cytoplasmic replication → umbilicated papule; Henderson-Paterson bodies on histology.