Page 5 of 22
DR8.2 | Herpes Simplex Recognition — SDL Guide
Learning Objectives
- Recognise herpes simplex and herpes labialis by their morphological signature — grouped vesicles on an erythematous base with prodrome and recurrence
- Explain why herpes simplex recurs, in terms of ganglion latency and reactivation triggers
- Distinguish primary from recurrent HSV disease and HSV-1 from HSV-2 by site and clinical pattern
- Differentiate herpes simplex from herpes zoster, aphthous ulcers, impetigo and syphilitic chancre, and select appropriate investigations and treatment
INSTRUCTIONS
Herpes simplex is one of the commonest viral infections of the skin and mucosa, and the recurrent cold sore (herpes labialis) is something almost every clinician sees weekly. The skill this SDL builds is recognition: reading the grouped vesicles on an erythematous base, the prodrome of tingling, and the tendency to recur at the same site, and then distinguishing herpes simplex confidently from the conditions that mimic it. Getting this right means reassuring most patients, treating appropriately with aciclovir or valaciclovir when it helps, and recognising the few situations — neonatal, disseminated or immunocompromised disease — where prompt action matters.
References
- Khanna N. Illustrated Synopsis of Dermatology & Sexually Transmitted Diseases, 6th ed. Ch: Viral Infections (Herpes Simplex) (textbook)
- Sacchidanand S (ed). IADVL Textbook of Dermatology, 4th ed. Section: Herpes Simplex Virus Infections (textbook)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
A 22-year-old college student returns to your clinic for the third time this year with the same complaint: a day of tingling and burning on her lower lip, followed by a cluster of small blisters that crust over and heal in about a week. She is otherwise well and is convinced something must be seriously wrong because 'it keeps coming back.' Her recurrent cold sore is the visible signature of a virus that has been living quietly in a nerve ganglion since childhood, reactivating whenever her immune guard drops. Recognising this pattern — grouped vesicles on an erythematous base that recur at the same site after a tingling prodrome — lets you reassure her, explain why it recurs, and treat it sensibly.
WHY THIS MATTERS
Herpes simplex will be one of the most frequent diagnoses you make in general and dermatological practice. Beyond the common cold sore, you must recognise genital herpes (a sexually transmitted infection requiring counselling and partner consideration), severe primary gingivostomatitis in children, and the danger situations — neonatal herpes, eczema herpeticum, and disseminated infection in the immunocompromised — where delayed recognition can be life-threatening. Knowing what herpes simplex looks like, why it recurs, and what it can be confused with allows you to reassure the majority, treat the minority who benefit from antivirals, and escalate the few who are genuinely at risk. This is a high-yield, everyday recognition skill.
RECALL
Recall from the viral foundations SDL and from Microbiology that herpes simplex virus is a member of the Herpesviridae — an enveloped DNA virus that establishes lifelong latency in sensory ganglia and reactivates periodically. Recall the herpesvirus life cycle: primary mucocutaneous infection, retrograde axonal transport to the ganglion, latency, and reactivation back down the nerve to the skin. Recall too that a Tzanck smear from a fresh herpesvirus vesicle shows multinucleate giant cells, a finding shared with varicella zoster, and that cell-mediated immunity is what holds the virus in check between recurrences. Keep these mechanisms in mind — they explain every clinical feature of herpes simplex you are about to recognise.
Recognising Herpes Simplex: The Morphological Portrait
Morphological Portrait of Herpes Simplex
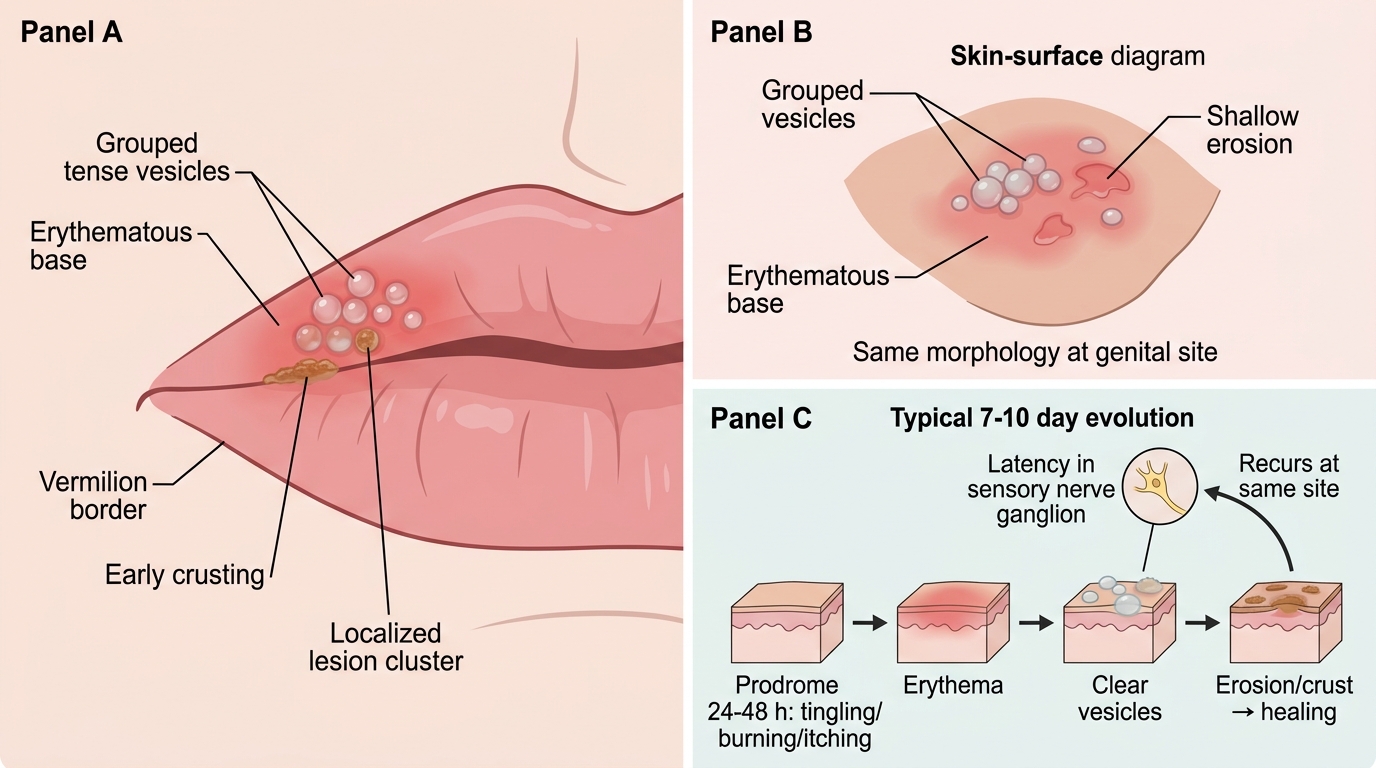
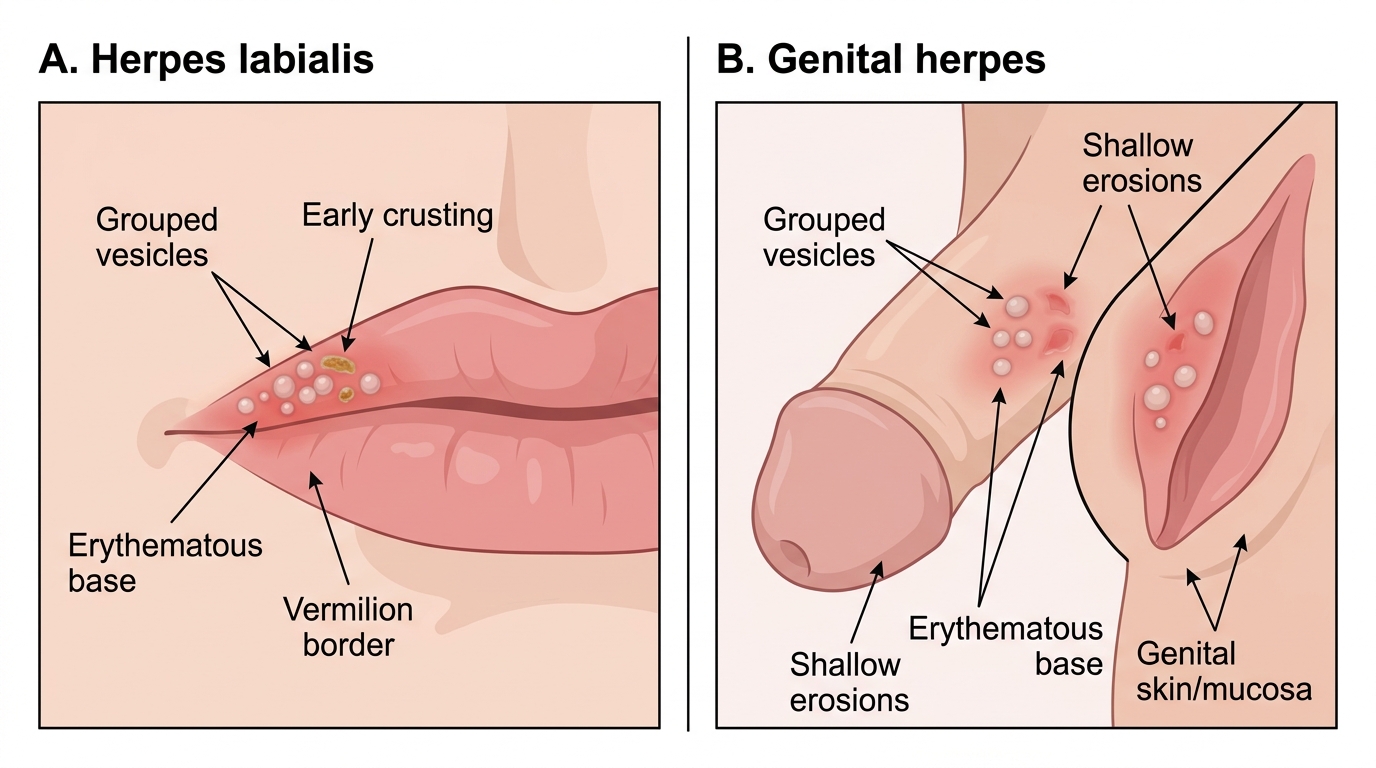
The defining visual portrait of herpes simplex is a cluster of small, tense vesicles sitting on a red (erythematous) base, and learning to read this signature is the core recognition skill of this SDL. The lesions typically begin as a localised patch of erythema, on which a group of clear vesicles erupts; over a few days the vesicles become cloudy, may form a small erosion or pustule, and then crust before healing, usually without scarring. A characteristic prodrome of tingling, burning or itching precedes the visible eruption by roughly 24 to 48 hours, and patients often learn to recognise their own warning sensation. The most common presentation is herpes labialis (the cold sore), a recurrent cluster on or near the vermilion border of the lip, but the same morphology appears in genital herpes and at other sites.
The features that together make the portrait recognisable are:
- Grouped vesicles (not a single vesicle, not a scattered eruption) on an erythematous base.
- A prodrome of localised tingling or burning before the vesicles appear.
- A tendency to recur at the same site, reflecting the nerve territory that harbours the latent virus.
- Evolution over about 7–10 days from erythema → vesicle → erosion/crust → healing.
Clinical Morphology of Herpes Simplex Lesions
HSV Pathogenesis: Why It Recurs
HSV Latency and Reactivation: The Neural Basis of Recurrence
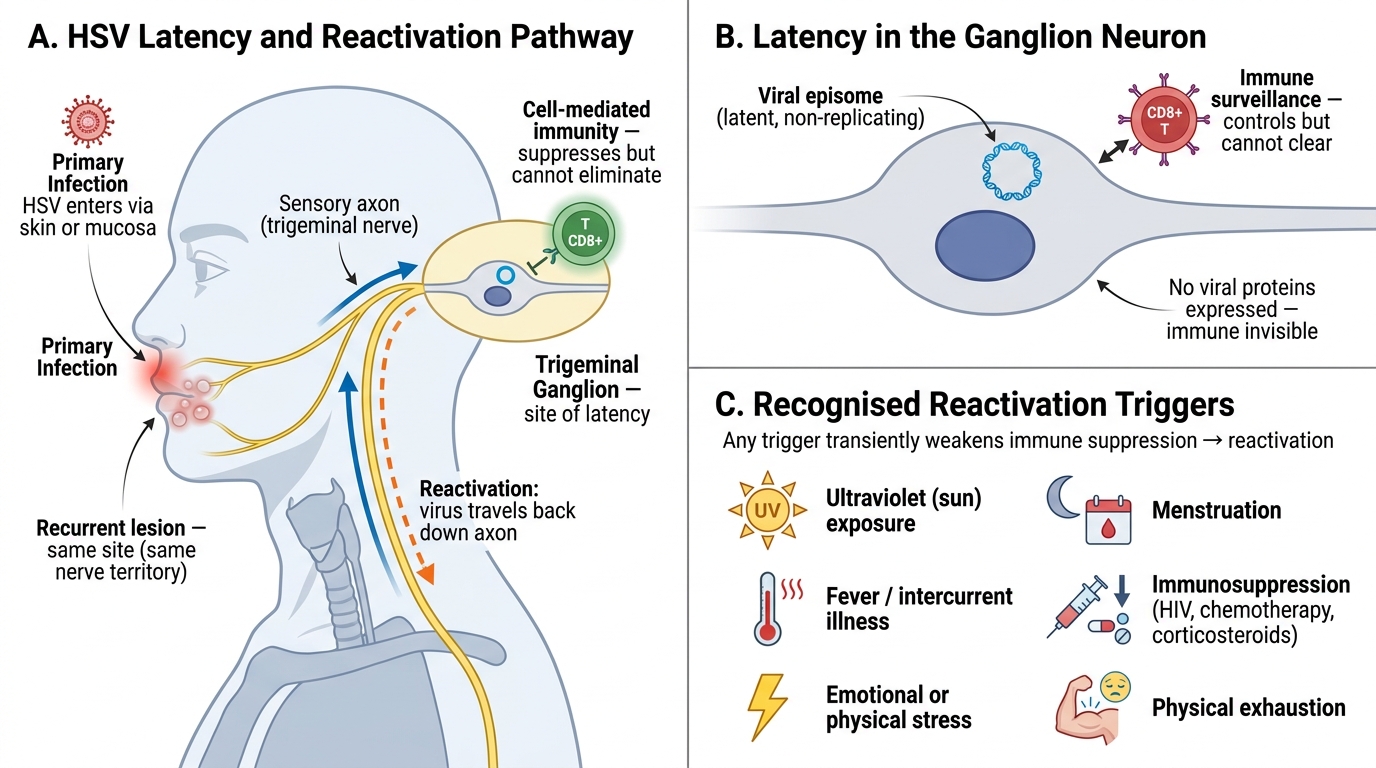
The single most useful idea for understanding herpes simplex is that the recurrent clinical pattern is a direct readout of the virus's biology. At primary infection, HSV enters through skin or mucosa, replicates locally, and then travels along sensory nerve axons to the cell bodies in the regional ganglion — the trigeminal ganglion for orolabial infection, the sacral ganglia for genital infection. There the viral genome persists in a latent state for the rest of the patient's life, neither eradicated nor actively replicating. The immune system, particularly cell-mediated immunity, keeps the latent virus suppressed but cannot remove it. When that suppression is transiently weakened, the virus reactivates, travels back down the same nerve to the skin, and produces a recurrent lesion in exactly the territory served by that nerve — which is why recurrences appear at the same site each time.
The recognised reactivation triggers, which patients can often identify in their own history, include:
- Fever and intercurrent infection (the old name 'fever blister' reflects this)
- Ultraviolet (sun) exposure
- Emotional or physical stress and fatigue
- Menstruation
- Immunosuppression — HIV, malignancy, chemotherapy, systemic corticosteroids
Understanding this mechanism lets you explain to patients, truthfully and reassuringly, why their cold sores recur and why the goal of treatment is to control episodes rather than to cure the latent infection.
SELF-CHECK
A patient asks why her cold sores keep recurring on exactly the same part of her lip. What is the correct explanation?
A. Each episode is a fresh infection caught from contact with another person
B. The virus lies latent in the trigeminal ganglion and, on reactivation, travels back down the same sensory nerve to produce a lesion in that nerve's territory
C. The virus has integrated into the skin cells of the lip and replicates there continuously
D. Recurrence at the same site indicates the infection is caused by a poxvirus rather than a herpesvirus
Reveal Answer
Answer: B. The virus lies latent in the trigeminal ganglion and, on reactivation, travels back down the same sensory nerve to produce a lesion in that nerve's territory
Recurrent herpes labialis reflects herpesvirus latency and reactivation. After primary infection, HSV travels to and lies dormant in the trigeminal ganglion. On reactivation (triggered by fever, UV, stress, menstruation or immunosuppression), the virus travels back down the same sensory nerve and produces a lesion in that nerve's cutaneous territory — which is why recurrences appear at the same site. Each episode is reactivation of the patient's own latent virus, not a new infection, and the latent virus cannot be eradicated, which is why treatment controls episodes rather than curing the infection. Herpes simplex is a herpesvirus, not a poxvirus.
Clinical Features: Primary vs Recurrent HSV, HSV-1 vs HSV-2
Primary vs Recurrent HSV and HSV-1 vs HSV-2
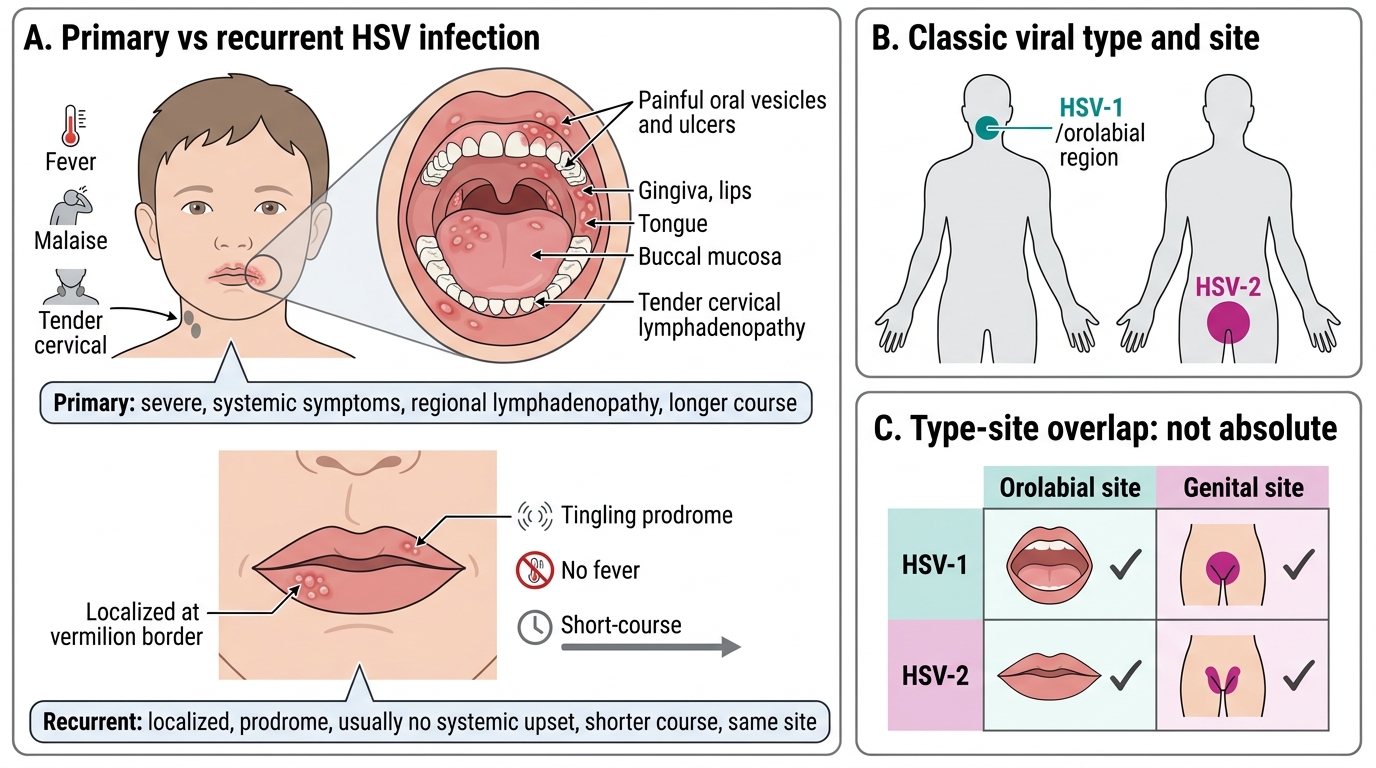
Recognising herpes simplex well means distinguishing a first (primary) infection from a recurrence, and understanding the relationship between viral type and site. Primary infection is the first encounter with the virus in a person without prior immunity, and it is typically more severe and more prolonged than later recurrences: primary orolabial infection often presents as herpetic gingivostomatitis in young children, with extensive painful oral vesicles and ulcers, fever, malaise and tender cervical lymphadenopathy, while primary genital infection presents as painful vulvovaginitis or balanitis with systemic upset. Recurrent disease, by contrast, is localised, briefer, preceded by a prodrome, and usually without systemic symptoms — the everyday cold sore. As for viral type, HSV-1 classically causes orolabial infection (herpes labialis) and HSV-2 classically causes genital infection, but this division is not absolute: either type can infect either site, so site alone does not definitively assign the subtype.
The distinctions to hold in mind are:
- Primary HSV: more severe, systemic symptoms (fever, malaise), regional lymphadenopathy, longer course; gingivostomatitis (oral) or vulvovaginitis/balanitis (genital).
- Recurrent HSV: localised, prodrome of tingling, no systemic upset, shorter course, same site each time.
- HSV-1: classically orolabial; HSV-2: classically genital — but each can affect either site, so type cannot be assumed from site alone (PCR distinguishes when it matters).