Page 2 of 17
FM3.{1,3} | Asphyxia: General & Mechanical — SDL Guide (Part 2)
Smothering and Choking: Features and ML Aspects
Smothering vs. Choking (Café-Coronary): Mechanisms of External and Internal Airway Obstruction
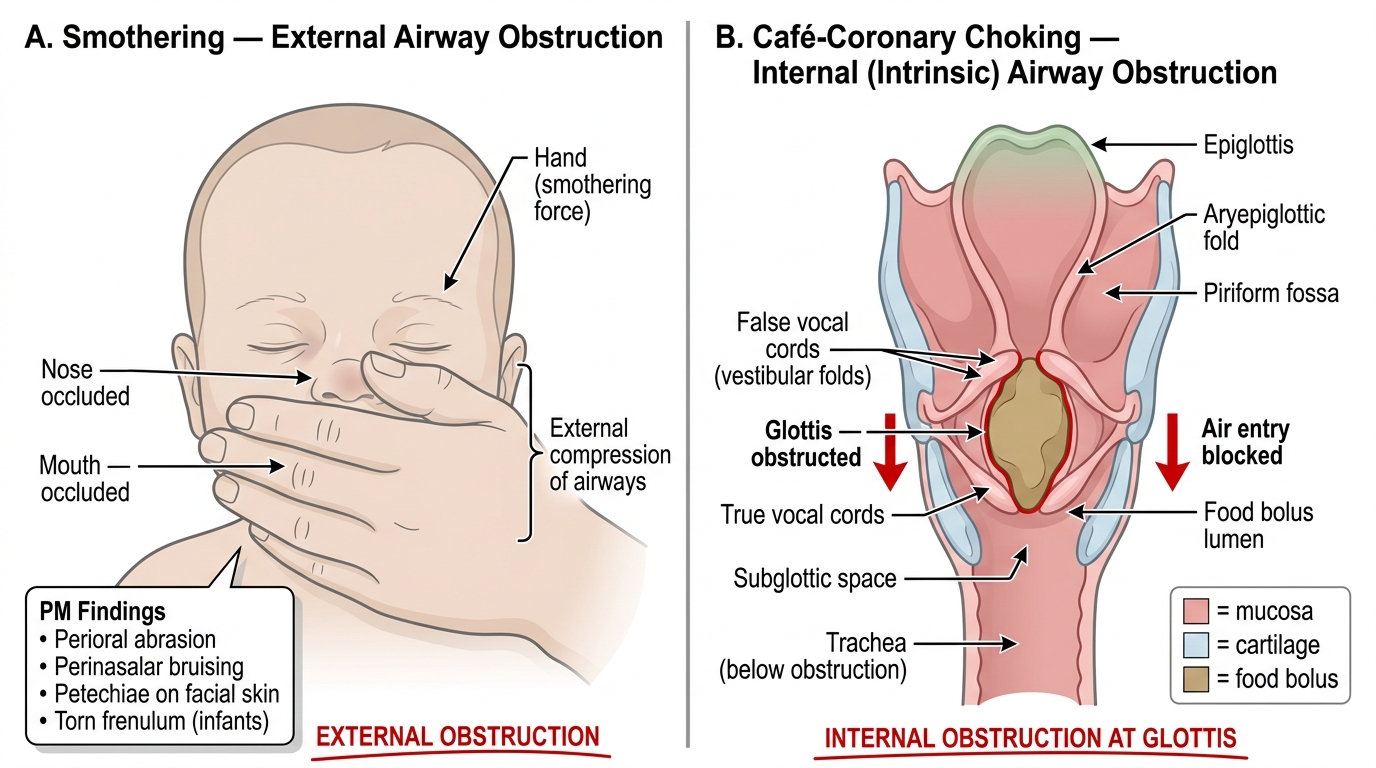
Smothering refers to the obstruction of the external airways — the nose and mouth — preventing air entry into the lungs. The obstruction is external, applied to the face, and the asphyxiating force may be a hand, a pillow, a plastic bag, or the bodyweight of another person. Smothering is an important type in forensic practice because it leaves minimal external evidence, making detection and medico-legal attribution challenging.
In adults, smothering requires the victim to be physically overpowered, deeply unconscious (intoxication, epilepsy, extreme age), or physically restrained. This is why smothering homicides cluster at the extremes of age and in victims with neurological impairment. In infants, a hand or soft surface over the face can cause death rapidly, and the PM findings may be subtle or absent.
PM findings in smothering:
• External: bruising or abrasions around the nose and mouth (perioral/perinasalar), particularly from a hand; petechiae on facial skin; torn frenulum (upper lip) in infants. However, when a soft object (pillow, blanket) is used, external injuries may be entirely absent.
• Internal: general asphyxial signs (Tardieu spots, cyanotic viscera, fluid dark blood); occasionally fibres from the smothering material may be found in the airways.
• Distinction from SIDS (sudden infant death syndrome) may be impossible at autopsy — this is a critical and well-recognised limitation.
Choking refers to obstruction of the internal airway — at the level of the larynx, trachea, or a major bronchus — by a foreign body. This is usually accidental. The classic scenario is the café-coronary syndrome: an elderly person (often with ill-fitting dentures), an intoxicated adult, or a small child inhales a food bolus that impacts at the glottis or subglottis, producing sudden death that mimics a cardiac event. The history of a meal, witness account of sudden distress while eating, and finding the food bolus at the glottis on examination establish the diagnosis.
PM findings in choking:
• Presence of the foreign body (food, toy, denture fragment) at the glottis or in the trachea
• General asphyxial signs
• Mucosal congestion of the upper airway around the obstruction
• No external signs of violence
ML aspects of smothering and choking:
Smothering is almost always either homicide (infanticide or elder abuse) or accident (overlying infant). The presence of perioral bruising, a torn frenulum, or petechiae on the face in an infant should prompt serious consideration of non-accidental injury. Documentation must be meticulous — photograph the face in close-up before touching. Choking, by contrast, is almost always accidental, but cases of deliberate forced choking (homicidal) do occur and must be distinguished by the clinical history, witness accounts, and any evidence of restraint.
Traumatic Asphyxia
Mechanism of Traumatic Asphyxia and Masque Ecchymotique
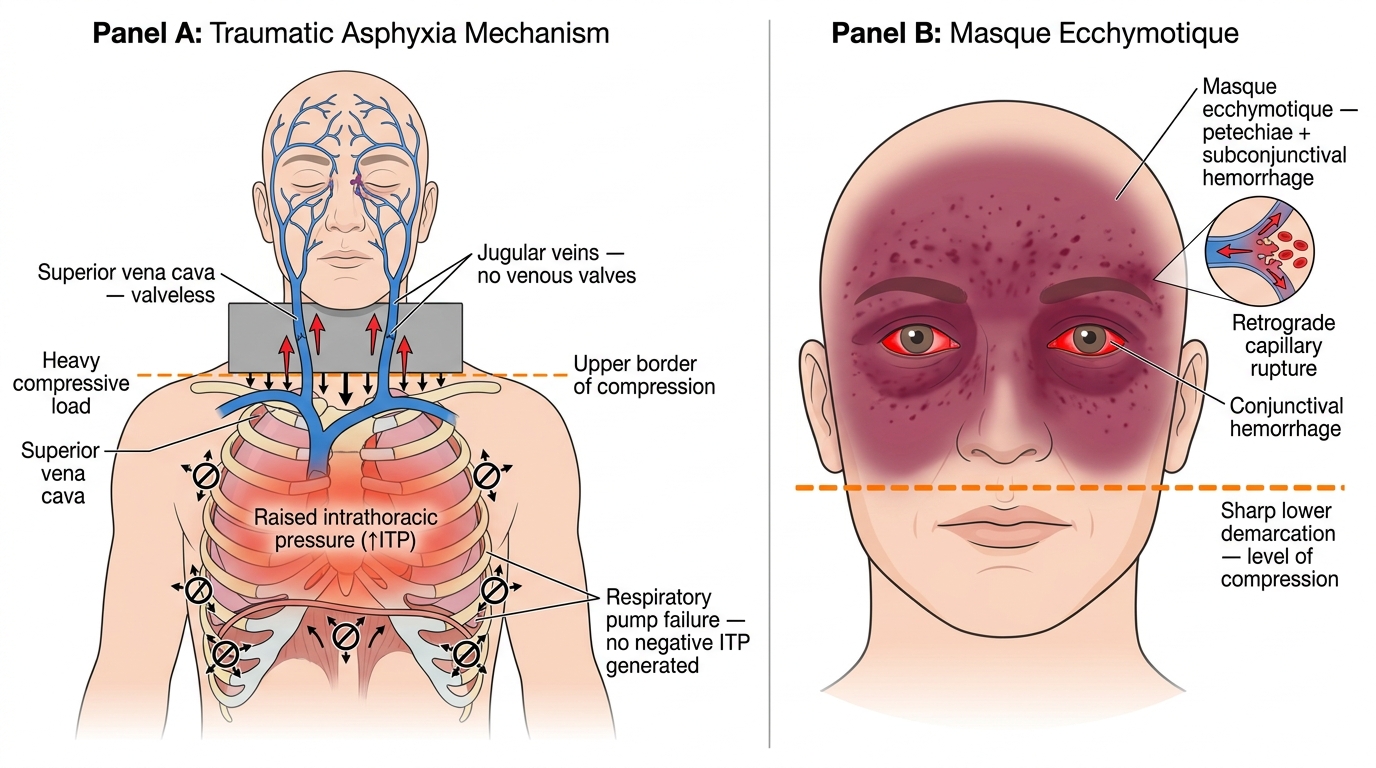
Traumatic asphyxia (also called crush asphyxia) results from external compression of the thorax and upper abdomen that mechanically prevents respiratory excursion of the chest wall. The compression does not obstruct the airway directly — instead, it immobilises the respiratory muscles (primarily the intercostals and diaphragm) so that the individual cannot generate the negative intrathoracic pressure needed for inspiration. The mechanism is therefore a failure of the respiratory pump, not an obstruction of the air column.
Traumatic asphyxia occurs in crowd crushes (religious gatherings, stampedes, football stadia), industrial accidents (machinery entrapment, building or wall collapse, grain silo entrapment, burial under earth or rubble), vehicular accidents where the chest is pinned, and occasionally in restraint scenarios. The incident at the hook of this SDL (grain storage collapse) illustrates the typical context.
The raised intra-thoracic pressure is immediately transmitted retrograde through the mediastinal veins (superior vena cava → jugular veins → capillaries of the face, conjunctivae, and upper extremities), because the valveless jugular veins offer no resistance to back-pressure. This accounts for the dramatic and characteristic external PM finding:
- Masque ecchymotique (mask of Morestin, traumatic cyanosis): intense violet-blue or purplish discolouration, petechiae, and oedema of the face, neck, and upper chest — sharply demarcated from the pale, compressed trunk below. The mask appearance is diagnostic of chest-wall compression asphyxia and is one of the most visually striking PM signs in forensic pathology.
- Bilateral subconjunctival haemorrhages: extensive, often sheet-like rather than petechial.
- Petechiae on the skin of the face, eyelids, and upper neck (above the compression line).
- Internal: general asphyxial signs; rib fractures and pulmonary contusions may co-exist if the compressing force was severe.
ML significance: The nature of the compressing object and the pattern of injury can help reconstruct the scene. Traumatic asphyxia is almost always accidental or associated with gross negligence (inadequate crowd management, industrial safety failure). Documentation of the masque and photography before the body is moved are essential.
Sexual (Autoerotic) Asphyxia
Provided image
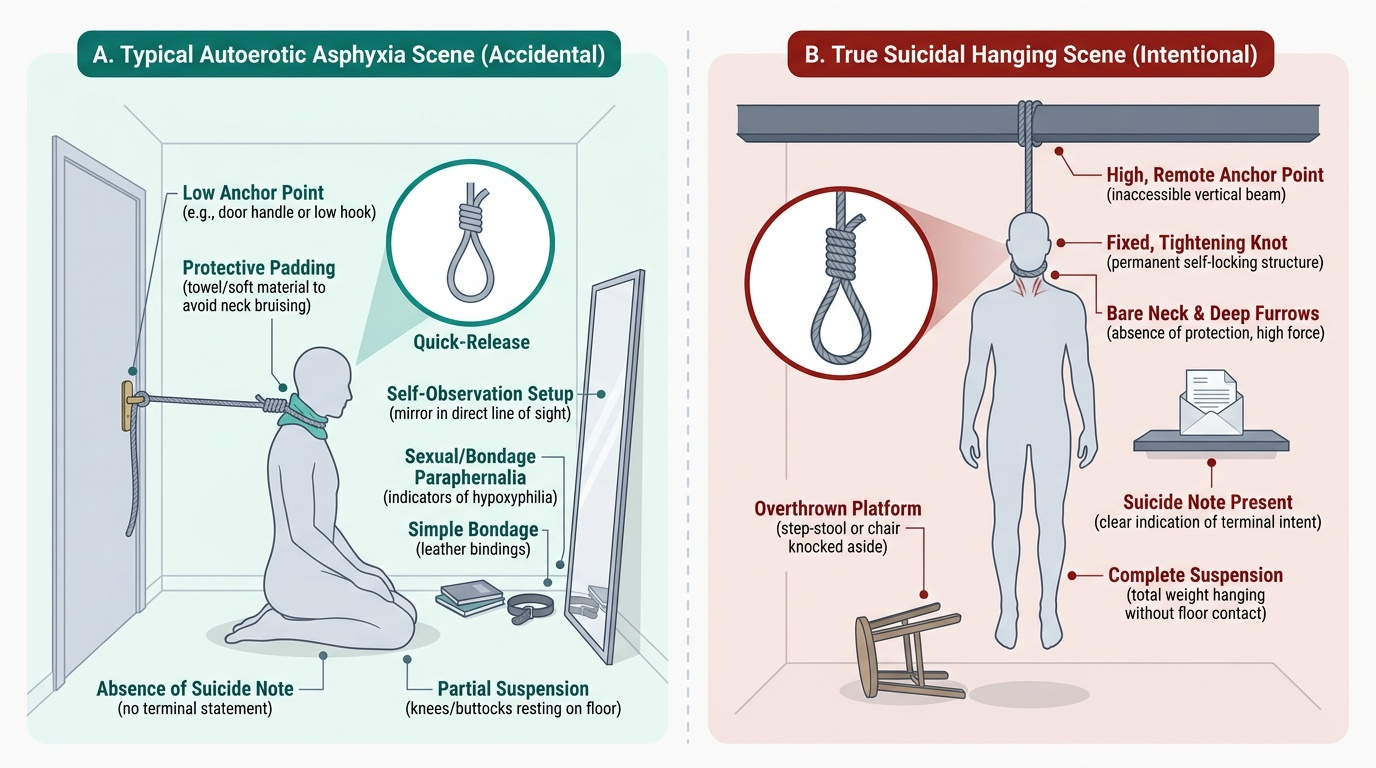
Sexual asphyxia, also called autoerotic asphyxia or hypoxyphilia, is a poorly-understood and under-reported entity in which an individual deliberately induces cerebral hypoxia as part of a sexual act, with the aim of intensifying orgasm. The physiological rationale offered in the literature is that mild cerebral hypoxia produces euphoria and heightened sensory awareness. The practice is almost exclusively solitary and male, though female cases are reported. The asphyxiating mechanism is typically self-hanging (partial suspension), a ligature around the neck with a quick-release mechanism, plastic bag over the head, or rebreathing apparatus.
The death is accidental — the person intends to release themselves before loss of consciousness, but the hypoxia progresses more rapidly than anticipated, the release mechanism fails, or a knot tightens beyond the individual's ability to undo while increasingly confused. The result is an unintentional death that, at the scene, may appear indistinguishable from a suicidal hanging.
Features that assist in differentiating autoerotic asphyxia from suicidal hanging:
• Evidence of a quick-release or escape mechanism (a separate rope, a slip-knot, a pad under the ligature)
• Bondage materials, sexual paraphernalia, mirrors positioned to allow self-viewing
• Protective padding under the ligature to prevent permanent marking (the individual intends to survive)
• Pornographic material at the scene
• Absence of a suicide note or any prior suicidal communication
• Dressed in cross-gender clothing in some cases
• Genitalia exposed or the individual partially undressed in a purposeful manner
The PM findings are identical to those of suicidal hanging, so the scene investigation and circumstantial evidence are pivotal. This has profound ML implications: a verdict of accidental death vs suicide affects life insurance payouts, family grief, and social stigma. The forensic physician should document the scene meticulously and avoid premature conclusions.
SELF-CHECK
A post-mortem examination reveals a 4-month-old infant with perioral petechiae and a torn upper labial frenulum. The parents report the infant 'just stopped breathing' overnight. Which asphyxial mechanism must be actively considered?
A. Choking on a foreign body
B. Smothering (non-accidental injury)
C. Traumatic asphyxia
D. Positional asphyxia
Reveal Answer
Answer: B. Smothering (non-accidental injury)
A torn frenulum (upper lip) in an infant is a recognised sentinel injury of non-accidental smothering or forced feeding. Perioral petechiae in combination strongly suggest external compression over the nose and mouth. Choking would be expected to reveal a foreign body in the airway. Traumatic asphyxia requires chest compression. Positional asphyxia would not produce perioral injuries. While SIDS cannot be excluded purely on PM grounds, these injuries mandate thorough investigation for non-accidental smothering.