Page 9 of 17
FM2.17-19 | Deaths from Physical Agents & Neglect — SDL Guide
Learning Objectives
- Describe the clinical features and post-mortem findings of heat illness (heat stroke, sun stroke, heat exhaustion, heat cramps) and cold injuries (systemic hypothermia, frostbite, trench foot, immersion foot)
- Describe the PM findings in burns and scalds, explain the vital reaction that distinguishes ante-mortem from post-mortem burns, and list the degrees of burns
- Describe the PM findings and distinguishing features of lightning injury versus domestic/power-line electrocution
- Describe the types of radiation injury, acute radiation syndrome stages, and their medico-legal context
- Describe the clinical features and PM findings of death from starvation and neglect, and apply the relevant legal framework
INSTRUCTIONS
Deaths from physical agents — heat, cold, burns, electricity, radiation — and from neglect and starvation are encountered across a wide spectrum of forensic practice: from industrial accidents to child abuse, from lightning during monsoon to building fires. Each physical agent leaves distinctive marks. This module teaches you to read those marks, reconstruct the causal chain, and frame the medico-legal opinion — including when negligence or homicide should be considered.
References
- KSN Reddy — Essentials of Forensic Medicine & Toxicology (textbook)
- BV Subrahmanyam — Modi's Medical Jurisprudence and Toxicology (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Three medico-legal cases arrive at the government mortuary on a summer day: (1) A 55-year-old construction labourer found collapsed on a rooftop at 2 PM with a core temperature of 41.2°C; (2) A 7-year-old child found unconscious in a locked car, with 30% burns of the chest and arms — the mother states 'it was an accident with boiling water'; (3) A body found near a substation with a small pale entry wound on the left palm and a corresponding exit wound on the right foot. How does the forensic physician approach each case differently? What question does the child's case raise that the others do not?
WHY THIS MATTERS
Physical agent deaths span a diverse forensic terrain — from heat stroke deaths among elderly patients during power failures to lightning fatalities that peak during the Indian monsoon. Critically, these deaths straddle the accident-neglect-homicide continuum. A worker who dies of heat stroke may be the victim of his employer's failure to provide adequate water and rest (IPC 304A — negligent death). A child with ante-mortem burns may have been deliberately scalded. A death attributed to 'accidental electrocution' may have involved deliberate interference with protective equipment. The forensic physician's skill at identifying the agent, establishing ante-mortem vs post-mortem injury, and estimating timing is what unlocks or forecloses the legal question.
RECALL
Recall from Year-1 Physiology:
- Thermoregulation: The hypothalamus maintains core temperature through sweating, vasodilatation, and metabolic rate adjustment. What happens when the ambient temperature exceeds 37°C and humidity is high?
- Protein denaturation: Heat irreversibly alters protein tertiary structure above ~42°C. Why does this matter for cell membranes in heat stroke?
- Ohm's Law and current: Electrical current (Amperes) = Voltage (Volts) ÷ Resistance (Ohms). Wet skin has much lower resistance than dry skin — why does this matter in electrocution?
- From Biochemistry: DNA and ionising radiation — how do gamma rays and X-rays damage DNA, and why does haematopoietic tissue fail first at high doses?
Thermal Deaths: Heat Illness
Heat Illness Spectrum: Clinical Features and Forensic Significance
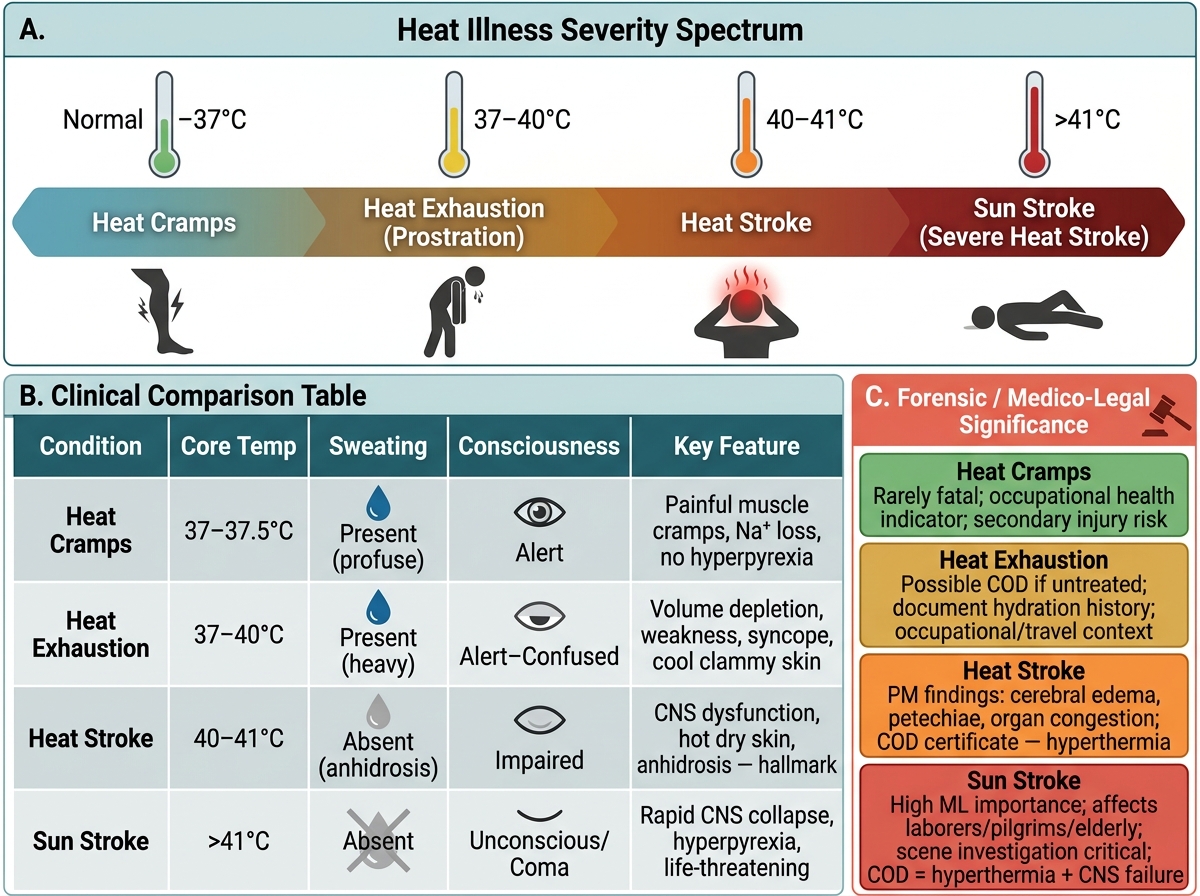
Heat illness is a spectrum of conditions resulting from the body's failure to maintain thermoregulatory equilibrium when heat gain exceeds heat dissipation. In forensic medicine, understanding the spectrum is critical because the conditions differ in severity, PM findings, and medico-legal implications. Indian forensic practice encounters heat illness deaths particularly among labourers, outdoor workers, pilgrims, and the elderly during summer months.
The four main syndromes, arranged from least to most severe:
Heat cramps are the mildest form. Excessive sweating causes salt (sodium chloride) loss from sweat, while water intake replaces fluid volume — the result is a sodium deficit in muscle tissue. Painful, sustained cramping of large muscles (calves, thighs, abdomen) occurs, typically without hyperpyrexia. Body temperature is normal or mildly elevated. Treatment is salt and fluid replacement. From a forensic perspective, heat cramps are rarely a direct cause of death but may lead to collapse and secondary injury. They are more commonly relevant as an occupational health indicator of inadequate rest and salt supplementation.
Heat exhaustion (heat prostration) results from volume depletion: prolonged sweating without adequate fluid replacement leads to dehydration and relative cardiovascular collapse. Core temperature is elevated but typically does not exceed 40°C, and — critically — consciousness is maintained (or only mildly altered). The patient is pale, sweating profusely, tachycardic, and hypotensive; they may have nausea, headache, and weakness. This is the most common heat-related illness seen clinically. Heat exhaustion is reversible with fluid replacement and cooling.
Heat stroke is a true medical emergency and the most severe and potentially fatal form. The core body temperature rises above 40°C with loss of thermoregulatory function — the sweating mechanism fails, and the patient's skin becomes hot and DRY (anhidrosis is the hallmark of classic heat stroke, though exertional heat stroke may still show sweating). CNS dysfunction — confusion, delirium, seizures, and coma — distinguishes heat stroke from heat exhaustion. Multi-organ failure (hepatic, renal, coagulopathy, rhabdomyolysis) ensues if untreated. Heat stroke can be:
• Classic (non-exertional) heat stroke: occurs in elderly, very young, and chronically ill during sustained high ambient temperatures (heat waves); passive heat exposure
• Exertional heat stroke: occurs in young, healthy individuals during intense physical activity in heat (soldiers, athletes, pilgrims)
Sun stroke is heat stroke precipitated specifically by direct solar exposure — the solar radiation adds a thermal load beyond the ambient temperature. The underlying pathophysiology is identical to classic heat stroke.
PM findings in heat stroke/sun stroke:
• Brain: oedema, petechiae, vascular congestion; cortical neurones show ischaemic changes
• Liver: acute hepatocellular necrosis (centrilobular)
• Kidneys: acute tubular necrosis
• Heart: focal myocardial necrosis
• Blood: DIC changes — microthrombi, petechial haemorrhages in multiple organs
• Skin: typically hot and dry
• No pathognomonic PM finding — the diagnosis relies on the history, scene temperature data, and exclusion of other causes of multi-organ failure
ML aspects of heat illness: Deaths from heat illness in an occupational setting (construction workers, those working near industrial furnaces) may constitute negligent death under IPC 304A if the employer failed to provide adequate rest, water, and heat management. Deaths of children or elderly in locked vehicles or rooms may raise questions of neglect or homicide if a responsible caregiver was present.
Thermal Deaths: Cold Injury
Hypothermia Severity Spectrum and Post-mortem Findings
Cold injuries are classified into two categories: systemic hypothermia (the entire body core temperature falls) and localised cold injuries (freezing or non-freezing injury to peripheral tissues while the core temperature is maintained). In India, systemic hypothermia is encountered in mountaineers, trekkers at altitude, flood victims, and occasionally in homeless individuals during winter. Localised cold injuries are primarily occupational (cold storage workers, military personnel) and in disaster-rescue scenarios.
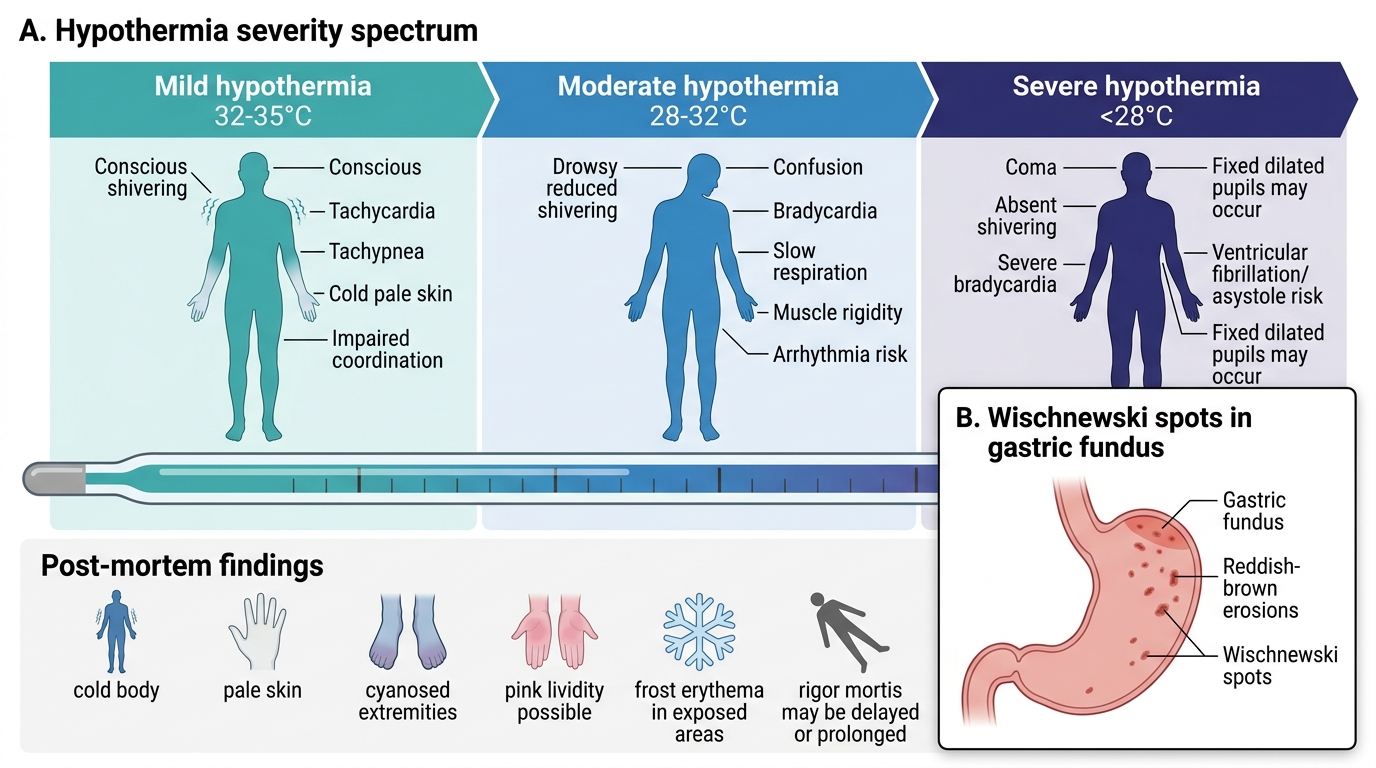
Systemic hypothermia is defined as a core body temperature below 35°C. It is graded by severity:
• Mild hypothermia (32–35°C): shivering (the body's thermogenic mechanism), vasoconstriction, mental confusion beginning
• Moderate hypothermia (28–32°C): shivering ceases (energy depleted), arrhythmias begin, progressive loss of consciousness
• Severe hypothermia (<28°C): ventricular fibrillation risk is highest; the heart is most sensitive to hypothermic arrhythmia at this range; fixed dilated pupils may mimic death
Important clinical note: Severe hypothermia can produce a state mimicking death — no palpable pulse, no detectable respiration, fixed dilated pupils. The clinical maxim applies: 'A patient is not dead until they are warm and dead.' Resuscitation should be attempted until core temperature is restored, because hypothermia provides cerebral protection.
PM findings in hypothermia:
• Wischnewski spots (Wischnewski's ulcers): reddish-brown mucosal erosions or haemorrhagic spots in the gastric fundus, regarded as a characteristic internal PM finding of hypothermia; they result from ischaemia and reperfusion injury to the gastric mucosa
• Frost erythema (pernio): pink-red skin discolouration over exposed areas, from peripheral vasodilatation that occurs paradoxically in late hypothermia
• 'Paradoxical undressing': a terminal behavioural phenomenon — severely hypothermic individuals remove their clothes due to a sensation of burning heat (mechanism: paradoxical peripheral vasodilatation causes a warm flush). Found at scenes as clothing scattered near the body.
• General signs: mild hepatic and renal congestion, pulmonary oedema, no pathognomonic histological finding
Localised cold injuries:
- Frostbite: occurs when peripheral tissue temperature falls below 0°C, causing ice crystal formation intracellularly and extracellularly. The extremities (fingers, toes), ears, nose, and cheeks are most vulnerable. Four degrees of severity mirror burn classification: first degree (erythema, oedema), second degree (blistering), third degree (necrosis of skin and subcutaneous tissue), fourth degree (gangrene to bone). At PM, frostbitten tissue appears dry, black, mummified.
- Trench foot (non-freezing cold injury): results from prolonged (12+ hours) exposure to cold, wet conditions above 0°C. Vascular damage is caused by sustained vasoconstriction and hypoxic endothelial injury. Associated with World War I trench conditions, but still occurs in flood victims, trekkers, and military personnel. Clinically: pallor, oedema, intense burning pain on rewarming.
- Immersion foot: a form of trench foot in which the entire foot is submerged in cold water. Common in shipwreck survivors, flood victims.
ML contexts for cold injury deaths: Exposure of vulnerable individuals (intoxicated persons left outdoors, neglected elderly, infants without adequate clothing) to lethal cold raises questions of neglect. In some deaths, the hypothesis of 'hidden homicide' must be considered if a vulnerable person is found dead in cold conditions — were they rendered unconscious and exposed deliberately?
SELF-CHECK
Which of the following is a characteristic PM finding of systemic hypothermia that should prompt the forensic physician to consider cold as the cause of death?
A. Masque ecchymotique (traumatic cyanosis of the face)
B. Wischnewski spots (reddish-brown gastric mucosal erosions in the fundus)
C. Lichtenberg figures (feathering on the skin)
D. Emphysema aquosum (waterlogged, over-distended lungs)
Reveal Answer
Answer: B. Wischnewski spots (reddish-brown gastric mucosal erosions in the fundus)
Wischnewski spots — reddish-brown haemorrhagic erosions in the gastric fundus — are a characteristic (though not exclusively pathognomonic) internal PM finding in deaths from hypothermia. They result from ischaemia-reperfusion injury to the gastric mucosa. Masque ecchymotique is pathognomonic of traumatic/crush asphyxia. Lichtenberg figures are pathognomonic of lightning strike. Emphysema aquosum is characteristic of wet drowning.
Burns and Scalds: Ante-Mortem vs Post-Mortem and Vital Reaction
Burns result from the application of dry heat (flames, hot metals, radiant heat) to the body surface. Scalds result from moist heat (hot liquids: boiling water, steam, hot oils). The pathological effects — thermal coagulation of protein, cell membrane destruction — are similar, but the pattern of injury differs: burns tend to produce irregular patterns following flame contact, while scalds produce splash or drip patterns.
Degrees of burns (classification by depth of tissue destruction):
• First degree (superficial): erythema (redness), pain, no blister formation; epidermis intact but inflamed
• Second degree (partial thickness): blistering with serum-filled vesicles; epidermis and upper dermis involved; painful, moist
• Third degree (full thickness): destruction of full skin depth including dermis and skin appendages; skin appears pale, charred, or leathery; painless (nerve endings destroyed)
• Fourth degree: involvement of deeper structures — subcutaneous fat, muscle, bone; occurs in prolonged flame exposure or contact with extremely hot surfaces
The critical forensic question: Was the burn ante-mortem or post-mortem?
This question has profound medico-legal significance. A burn victim found in a fire may have been alive when the fire started (accident or homicide by fire) or may have been dead before the fire was set (fire used to conceal a prior killing). The distinction rests on the concept of the vital reaction — the tissue response that only occurs in living tissue.
Histological Vital Reaction Criteria: Ante-mortem vs Post-mortem Burns
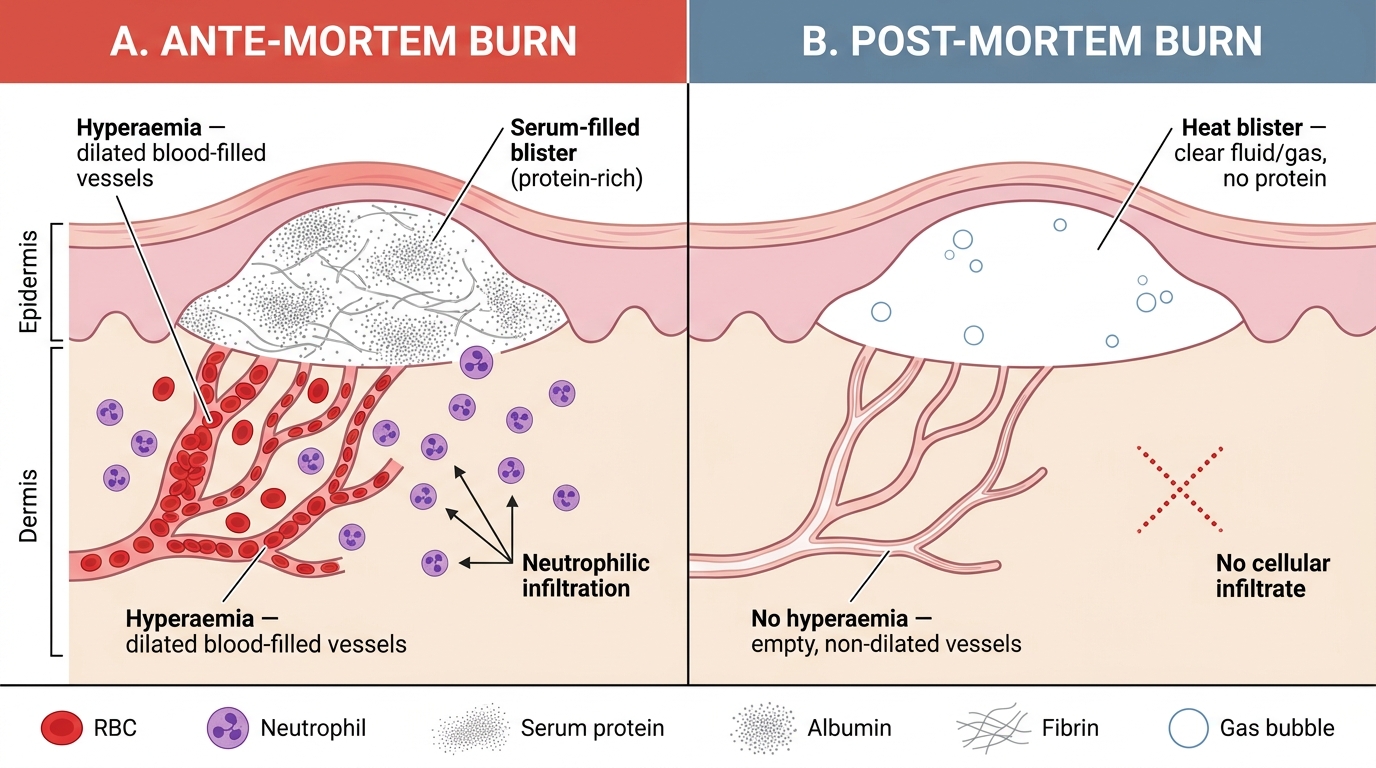
Vital reaction criteria in ante-mortem burns:
1. Hyperaemia (active congestion): the living body responds to thermal injury with vascular dilatation and increased blood flow. At PM, histology shows dilated, blood-filled vessels at the burn margin.
2. Blistering with serum: The blister fluid of ante-mortem burns is serous — it contains plasma proteins (albumin), fibrin, and inflammatory cells (neutrophils and macrophages). This protein-rich fluid is a product of acute inflammation, which requires living cells.
3. Leucocytic (neutrophilic) infiltration: Neutrophils migrate into the burn tissue within 30–60 minutes of a thermal injury in a living person. Their presence at the burn margin on histology is the most reliable and specific marker of vital reaction.
4. Vital soot inhalation: If the victim was alive in a burning enclosure, they will have inhaled smoke. PM findings: soot in the airways (trachea, bronchi), carboxyhaemoglobin in the blood (>10%, typically >50% in fire deaths). Carbon monoxide saturation in blood is the single most reliable indicator that a fire victim was alive when the fire started.
Post-mortem burns: A body exposed to fire after death may develop heat blisters, but these differ: the blister fluid is thin, watery, and gas-filled (not serum-rich), with no cellular infiltrate. The skin char pattern and distribution may differ from ante-mortem burns. Absence of soot in airways and absence of carboxyhaemoglobin in blood strongly suggest post-mortem fire exposure.
Pugilistic attitude (boxer's posture): In fire deaths, the heat causes muscle proteins to contract and coagulate, causing flexion of the elbows, knees, and hips — the body assumes a flexed 'boxing' posture. This is a post-mortem heat artefact and does NOT indicate the victim was alive or fighting.
Scalds vs dry burns: In the context of child abuse (the hook scenario), the pattern of scalds can indicate whether immersion or splash occurred. Immersion scalds (deliberate holding of a child's body part in hot water) produce sharply demarcated burn lines ('high-water marks'), sparing flexural creases; accidental splash scalds produce irregular splash patterns, often on the front of the body. Forced immersion scalds of the buttocks and perineum are characteristic of non-accidental injury.