Page 6 of 17
FM3.2 | Hanging & Strangulation — SDL Guide (Part 2)
Throttling (Manual Strangulation): Features and PM Findings
Cutaneous Marks and Grip Pattern in Throttling (Manual Strangulation)
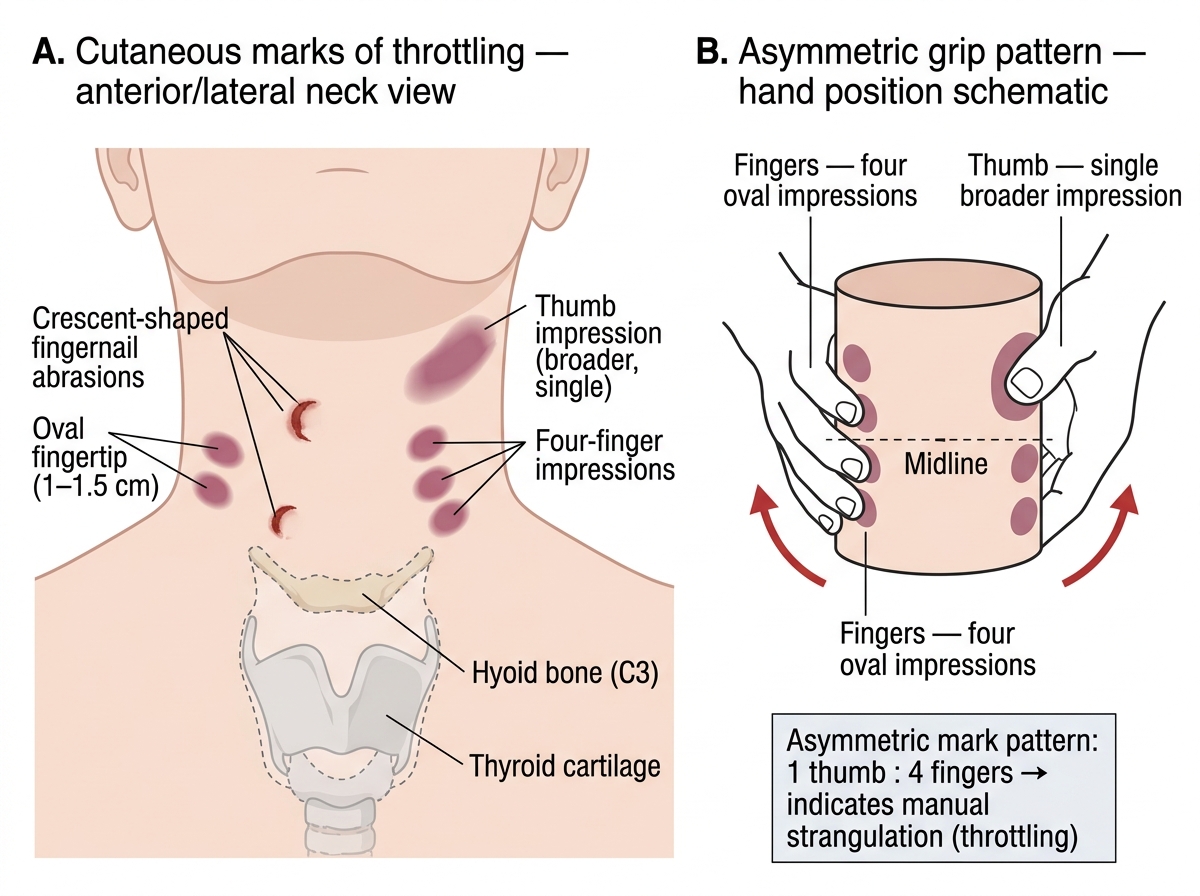
Throttling is manual strangulation — compression of the neck by the hands of another person. It is entirely and invariably a homicidal act in adults. The fingers and thumbs of the assailant compress the neck from the front and sides, occluding the jugular veins and carotid arteries. The mechanism of death is identical to other forms of neck compression — venous obstruction → cerebral hypoxia — but the PM findings are distinctive because the compressing instrument is the human hand.
PM findings in throttling:
- Fingernail abrasions (crescent-shaped contusions): the characteristic mark of throttling. Multiple small, 1–2 cm crescent-shaped cuts or bruises arranged in a semicircle pattern on the front and sides of the neck, reflecting the grip of the assailant's fingers. These are the most specific PM finding of throttling.
- Oval/round bruises from fingertips: corresponding to the pad of each finger pressing into the neck soft tissues
- Asymmetric distribution: one thumb typically leaves a broader bruise on one side; the four fingers leave marks on the opposite side. The distribution can suggest whether the assailant used one hand or two, and whether they were facing the victim
- No ligature mark: the hands leave bruises and nail marks but no encircling imprint
- Hyoid bone fracture: occurs more commonly in throttling than in hanging or ligature strangulation, because manual compression generates high localised pressure against the hyoid. Greater fracture rate also in the elderly due to ossification
- Laryngeal cartilage fractures: thyroid and cricoid cartilage fractures possible
- Internal neck dissection: haemorrhage in strap muscles, damage to carotid sheaths, carotid body contusion
- Facial signs of asphyxia: prominent congestion, petechiae, cyanosis — more intense than in hanging because victims struggle longer
ML significance: Because throttling is invariably homicidal, the PM report must document every finger mark, photograph them, and, if possible, take dimensions that allow estimation of the assailant's hand size. Injuries to the victim's hands (defensive wounds from grabbing the attacker's wrists) should also be documented. Position of the body and staging of the scene may sometimes suggest that marks were inflicted post-mortem — neck dissection and histological assessment of bruise vitality (leucocytic infiltration) can help resolve this.
Examination and Preservation of Ligature Material
Correct Preservation of Ligature Evidence
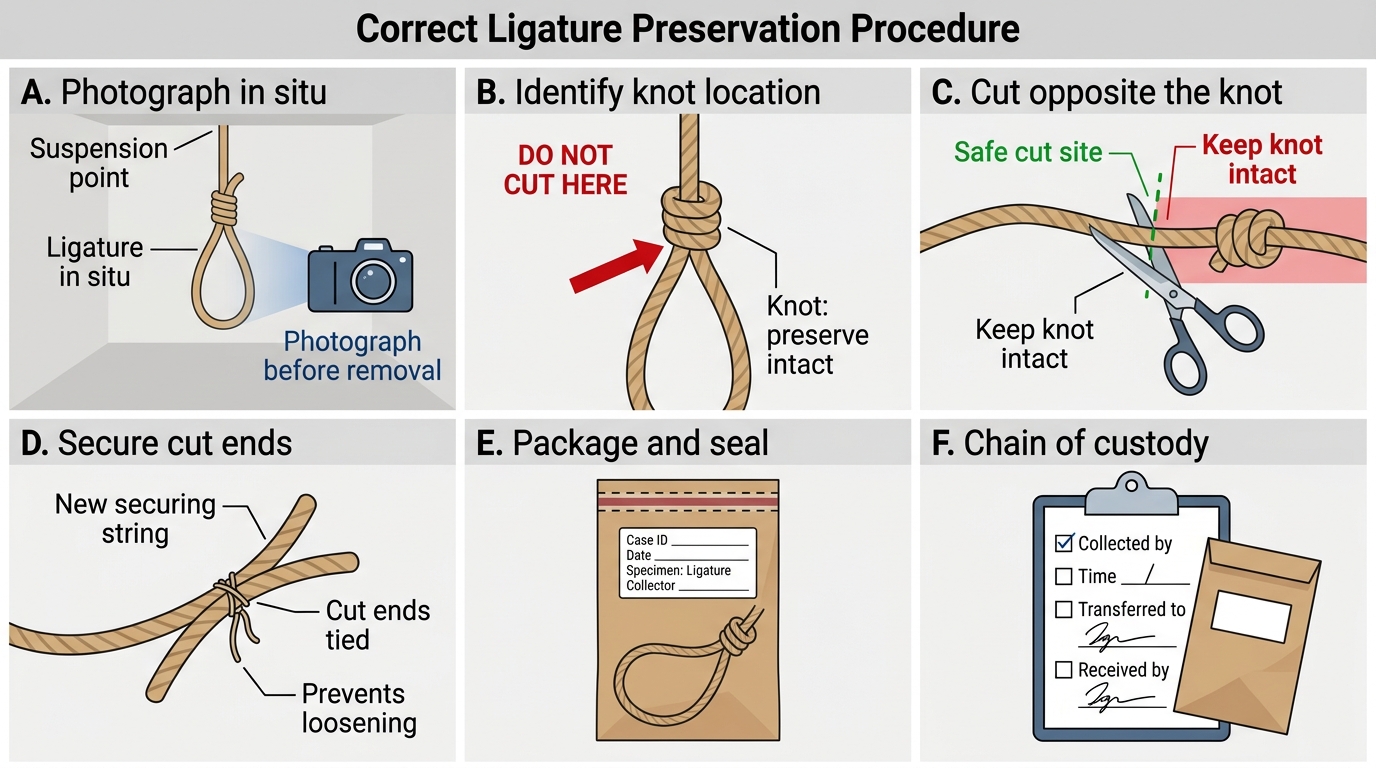
The examination and proper handling of the ligature is a critical forensic act. Improper removal of the ligature from a hanging victim — particularly cutting through the knot — can destroy the single most important physical evidence in the case. A well-preserved knot can reveal whether it was self-tied (consistent with suicide) or tied by another (suggesting homicide). Forensic laboratories examine knot type, material fibres, and fingerprints on the ligature.
Step-by-step procedure for ligature examination and preservation:
- Do not remove the body until scene photographs are complete: Photograph the suspension point, the body position, the ligature material in situ, and the knot from multiple angles. Describe and measure the height of the suspension point from the floor.
- Cut the ligature at a point well away from the knot (usually on the side opposite the knot): Use scissors or a knife to cut the rope, never through or adjacent to the knot. This preserves the knot's integrity entirely.
- Secure the cut ends immediately: Tie the free end with a new piece of string or seal it with adhesive tape to prevent the knot from loosening.
- Do NOT untie the knot under any circumstances at the scene or mortuary. The knot must reach the forensic science laboratory in its original state.
- Document the ligature in detail: Material (rope, cloth, wire, belt), diameter, any special characteristics (double knot, slip knot, quick-release, padding under ligature), colour, any labels or identifiable marks.
- Preserve in a clean paper envelope or paper bag: Do NOT use plastic (traps moisture, promotes decomposition of biological trace evidence). Seal and label with the case number, date, name, and the officer/physician who collected it. This initiates the chain of custody — every subsequent transfer must be documented.
- At PM examination: Before neck dissection, the PM report should describe the ligature mark in full — position, orientation, depth, breadth, parchment quality, pattern. Compare the mark pattern with the ligature material (does the weave match?).
Dispatch: The preserved ligature is dispatched to the Forensic Science Laboratory (FSL) with a forwarding letter specifying the query (e.g. 'comment on the type of knot — was it self-tied or applied by another?; presence of fingerprints; fibre analysis').
SELF-CHECK
You are called to examine a body found with a thin cord around the neck. The ligature mark is at the level of the thyroid cartilage, horizontal, and continuous around the entire circumference of the neck. The face shows marked congestion and bilateral subconjunctival haemorrhages. The most likely manner of death is:
A. Suicidal hanging (typical)
B. Accidental positional asphyxia
C. Ligature strangulation — investigate as homicide
D. Autoerotic asphyxia
Reveal Answer
Answer: C. Ligature strangulation — investigate as homicide
The three distinguishing features of ligature strangulation — as opposed to hanging — are: mark at/below the thyroid cartilage (not above), horizontal orientation (not oblique), and continuous circumference (no gap at the knot). All three are present here. Together with the marked facial congestion and bilateral subconjunctival haemorrhages (consistent with sustained struggle before death), this pattern mandates investigation as a homicide. Suicidal hanging produces an oblique, above-thyroid, discontinuous mark. The case history in the SDL hook illustrates exactly this scenario.
Medicolegal Aspects: Differentiating Hanging, Strangulation, and Throttling
The medicolegal determination of manner of death in neck compression deaths is one of the most forensically consequential judgments a physician makes. The table below, together with the narrative above, provides the systematic comparative framework.
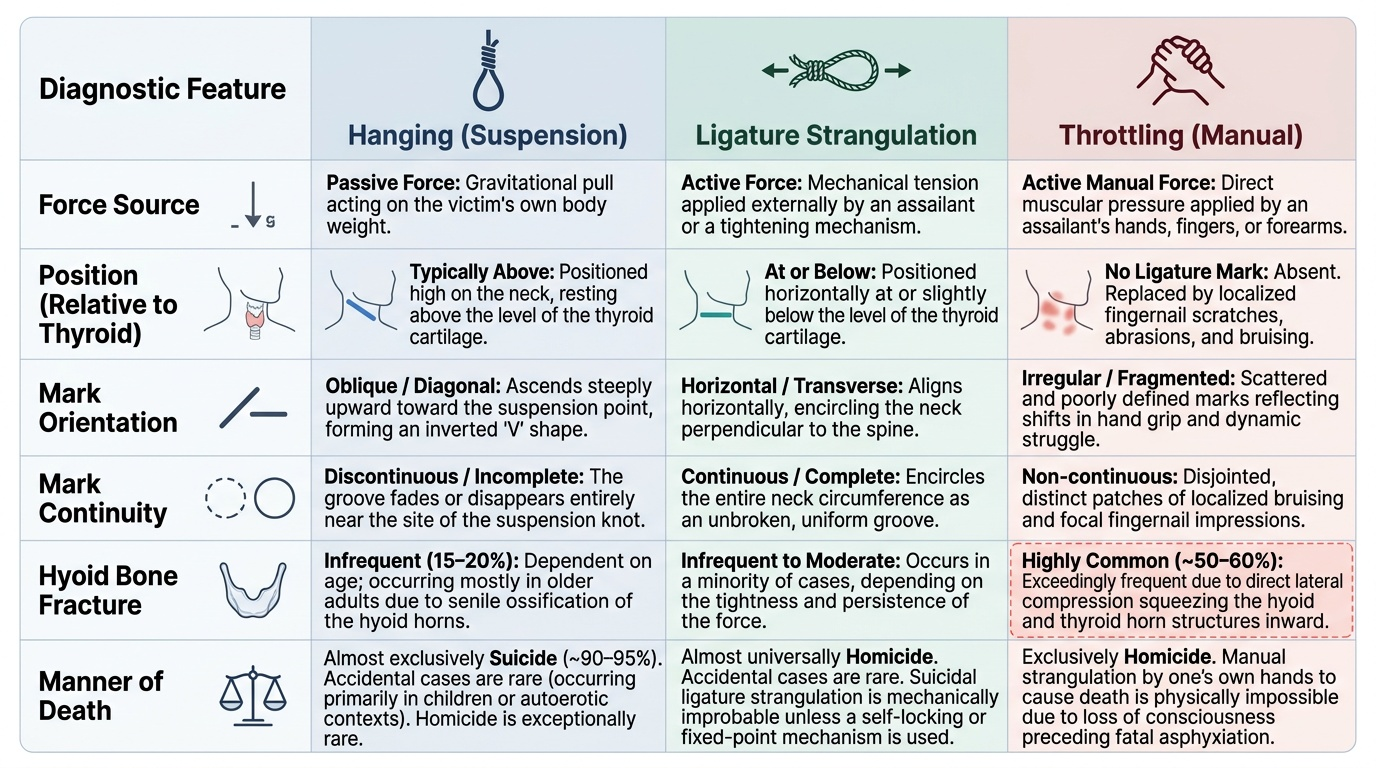
Provided image
General principles for manner-of-death determination:
- Hanging is strongly associated with suicide in adults (approximately 90–95% of hanging deaths in forensic series are suicide). However, homicidal hanging has been described (victim rendered unconscious first, then suspended), as has accidental hanging in children or intoxicated individuals. Scene investigation, absence of force marks on the body, intact ligature knot, and a suicide note all support suicide. The forensic physician does not determine manner of death — the court does, using the physician's expert report.
- Ligature strangulation is almost always homicide in adults. A suicide by ligature strangulation would require maintaining grip on the ligature while losing consciousness — mechanically possible only with a fixed-point mechanism (garotte stick left in place) but extremely rare.
- Throttling is invariably homicide in adults. It is impossible to throttle oneself to death. Documentation must be systematic and thorough, with all finger marks photographed and measured.
IPC relevance:
• IPC Section 302 (murder): applicable if homicidal strangulation or throttling is established with evidence of intent to kill
• IPC Section 304 (culpable homicide not amounting to murder): where intent to kill is unclear but the act was likely to cause death
• IPC Section 299–302 framework: the distinction between culpable homicide (304) and murder (302) depends on intent and knowledge — the forensic physician's role is to establish cause and manner of death, not intent
Key points for expert court testimony:
1. State all positive findings precisely (position of mark, orientation, continuity, facial congestion pattern)
2. State negative findings as well (e.g., 'no finger marks or nail abrasions were found on the neck')
3. Avoid categorical declarations of manner: 'the findings are consistent with/inconsistent with hanging/strangulation' is more defensible than 'this is homicide'
4. If PM findings are equivocal (e.g. decomposed body, post-mortem artefact modification of the ligature mark), acknowledge the limitation
5. Ligature evidence (knot type, fibre match) and scene evidence are as important as the PM report
CLINICAL PEARL
Never cut through the knot. When removing a ligature from a hanging or strangulation victim, always cut the rope on the side opposite the knot, at a point well clear of it. The type of knot — slip knot, fixed knot, granny knot — is forensic evidence that a court may rely on to determine whether the victim could have tied it themselves. A destroyed knot cannot be reconstructed. This single procedural rule has settled contested court cases.