Page 8 of 18
FM2.{20,24,26} | Special-Situation Autopsies: Custody, Negligence & Anaesthetic Deaths — SDL Guide (Part 2)
Protocol for Anaesthetic and Operative Deaths
Death during or immediately following anaesthesia and surgery triggers a specific medico-legal investigation protocol because the cause of death is frequently contested between the surgical team, the anaesthesiologist, the institution, and the patient's family. The forensic physician conducting this autopsy must operate as an investigator, not merely a pathologist.
The special collection protocol for anaesthetic/operative death autopsy includes:
| Specimen/Item | What It Detects | Preservation | Chain of Custody |
|---|---|---|---|
| Blood (ante-cubital, cardiac) | Anaesthetic agent levels, drug toxicity, electrolytes | Sodium fluoride tube; separate plain tube | Sealed, labelled → to FSL under magistrate order |
| Urine | Metabolites of drugs, anaesthetic agents | Sealed tube | FSL |
| Gastric contents | Aspiration contents, drugs ingested | No preservative | FSL |
| All syringe/vial contents used during procedure | Verify what was actually administered | Seals intact; send as-is | Police custody via court order |
| Anaesthetic record (chart) | Drug doses, timing, vital sign trends | Court order to hospital to produce | Judicial custody |
| Operation notes, nursing chart | Sequence of events, timeline | Court order | Judicial custody |
| Equipment (if malfunction suspected) | Technical failure | Isolated and sealed by court order | Court custody |
| Brain, spinal cord | Anaesthetic-related CNS changes, air embolism | Formalin (histology) | Histopathologist |
| Lung | Aspiration, pulmonary embolism, bronchospasm | Formalin | Histopathologist |
The physician must document the state of the airway, the position of the endotracheal tube if still in situ, and the presence of any injection sites. Hospital records cannot be collected by the forensic physician directly — they must be obtained by the police or magistrate under a court order to prevent selective disclosure.
An important structural principle: the forensic physician's role in anaesthetic death investigation is to establish what pathological changes occurred and what material evidence exists — not to directly determine whether the anaesthetic care was adequate. The adequacy of care question requires expert testimony from an anaesthesiologist or the relevant surgical specialist. This distinction between the pathological opinion (what the PM showed) and the expert clinical opinion (was the care standard met?) is essential for the team-based approach mandated by FM2.26.
SELF-CHECK
In the investigation of an anaesthetic death, the forensic physician wishes to obtain the anaesthetic chart and operation notes. The physician should:
A. Request the hospital superintendent to produce the records at the time of autopsy
B. Ask the anaesthesiologist to submit a copy of the anaesthetic chart
C. Obtain the records through a court order (magistrate order) to prevent selective disclosure
D. Attach a copy of the hospital discharge summary to the PM report
Reveal Answer
Answer: C. Obtain the records through a court order (magistrate order) to prevent selective disclosure
Hospital records in anaesthetic death investigations must be obtained under a court (magistrate) order to prevent selective disclosure or alteration of records by the institution. Requesting records directly from the hospital administrator or treating team creates a significant risk that incomplete or selectively edited records are provided, potentially compromising the investigation.
Medicolegal Inference and Statutory Framework
The medicolegal framework governing special-situation deaths draws on multiple statutory provisions that the forensic physician must know precisely.
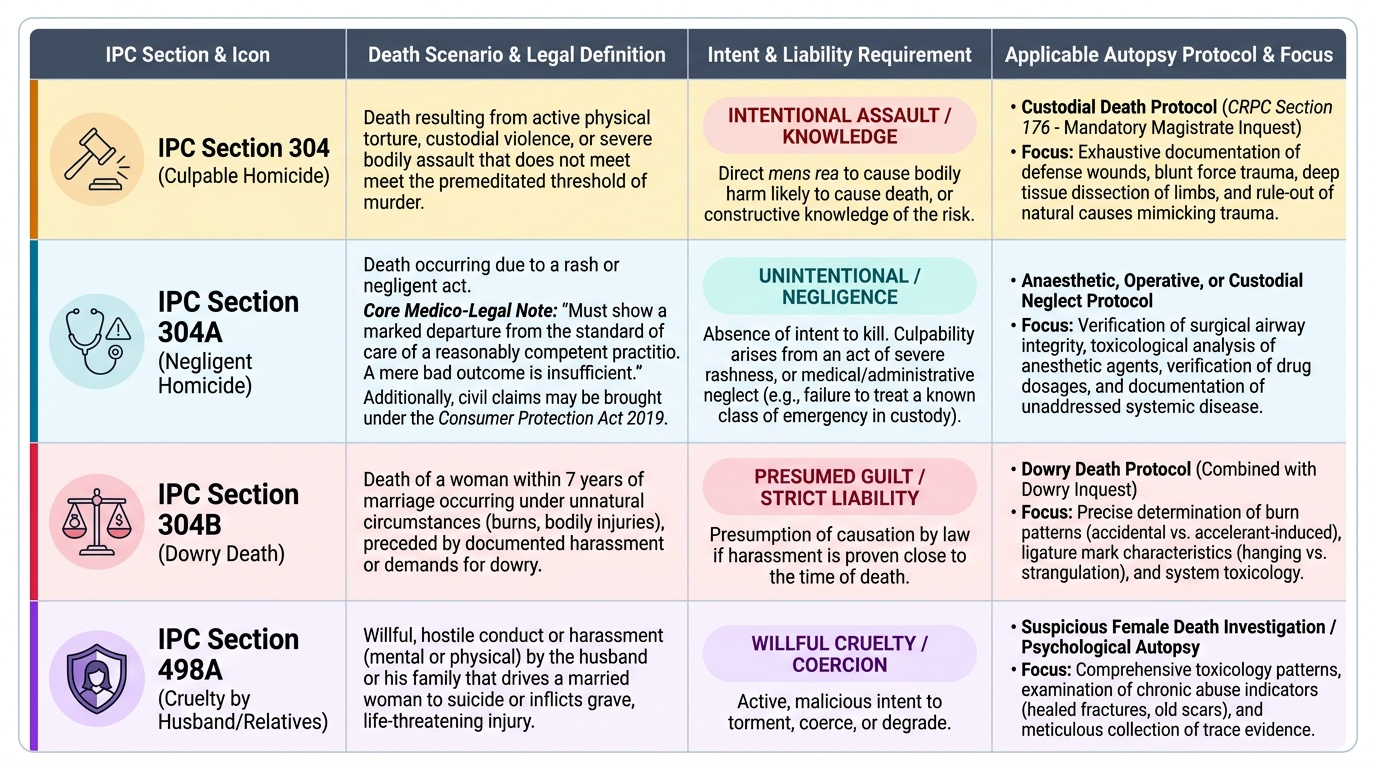
For custodial deaths: the primary statutory provisions are CRPC Section 176 (mandatory magistrate inquest, as discussed); IPC Section 304 (culpable homicide not amounting to murder — if assault is established); IPC Section 304A (causing death by a rash or negligent act — for cases where the custody death results from negligence rather than intentional assault, e.g. untreated medical emergency). The NHRC has authority under the Protection of Human Rights Act 1993 to investigate and recommend compensation, though it cannot try criminal offences. The accountability of the state extends to constructive knowledge: if the deceased was known to have a medical condition that required treatment and was not provided treatment, that constitutes actionable negligence even in the absence of direct assault.
For anaesthetic and operative deaths: the primary provision is IPC Section 304A — negligence causing death (unintentional). Consumer protection claims under the Consumer Protection Act 2019 (which replaced the 1986 Act — do NOT cite the 1986 Act for current jurisdiction) may also be brought by the family. The threshold for IPC 304A is a 'rash or negligent act' — mere bad outcome is insufficient; there must be a departure from the standard of care that a reasonably competent practitioner would have maintained.
For dowry deaths: these fall under the custodial protocol when the death occurs in custody, but also invoke IPC Section 304B (dowry death — death within seven years of marriage associated with cruelty or harassment related to dowry demands) and IPC Section 498A (cruelty by husband or relatives). CRPC Section 176 mandatory magistrate inquest applies. The forensic physician must document findings that speak to the nature and age of injuries and whether signs of chronic physical abuse are present.
Team-based approach (FM2.26): the team model is not optional in these cases — it is a professional standard and a practical requirement. The forensic physician cannot be expected to opine on the adequacy of anaesthetic care without an anaesthesiologist's input; cannot fully evaluate custodial injuries without consultation when specialist interpretation is required; and working in a team provides institutional protection against allegations of biased reporting. The lead forensic physician coordinates the team, assigns specific examination responsibilities, and integrates all specialist findings into a coherent PM report and opinion.
Provided image
CLINICAL PEARL
Pearl: Know the two NHRC guideline sets separately. Students frequently state 'NHRC guidelines' as a single monolithic entity. There are two distinct operational documents: the general framework for investigating human rights violations (principles-level) and the specific 1997 Guidelines for Investigation of Deaths in Custody (operationally specific — video recording, Section 176, report to magistrate not police, team composition, NHRC notification within 24 hours). In examination viva or scenario questions, specify which set you are applying and to which element of the protocol you are referring.
SELF-CHECK
Under which IPC section can a doctor be prosecuted for a death caused by a rash or negligent act during medical care?
A. IPC Section 302
B. IPC Section 304
C. IPC Section 304A
D. IPC Section 304B
Reveal Answer
Answer: C. IPC Section 304A
IPC Section 304A covers causing death by a rash or negligent act, not amounting to culpable homicide — the applicable provision for deaths from medical negligence. Section 302 is murder; Section 304 is culpable homicide not amounting to murder (requires intent); Section 304B is dowry death. The distinction between 304 and 304A hinges on intent: 304A applies when there is no intent to cause death but there is a rash/negligent act.