Page 2 of 6
FM9.2-4,FM14.17 | Torture, Custody Examination & Human-Rights Protocols — SDL Guide
Learning Objectives
- Define torture and describe the physical and psychological injuries it causes, including long-term sequelae
- State the Istanbul Protocol and the NHRC 1997 guidelines and their requirements for custodial medical examination
- Conduct and document a systematic examination of a person in police or judicial custody per FM14.17
- Demonstrate professionalism — including avoiding re-traumatisation, maintaining confidentiality, and appropriate referral — when examining torture survivors
- Prepare a medicolegal report for court or NHRC in cases of custodial torture or human rights violations
INSTRUCTIONS
Torture is one of the gravest violations of human dignity, and the forensic physician occupies a uniquely powerful position: as the professional most likely to encounter survivors and most qualified to document evidence that will determine accountability. This module covers the full arc from legal context through clinical method to the preparation of a medicolegal report — integrating the international Istanbul Protocol, the Indian NHRC guidelines, and the professional standards that protect both survivors and the integrity of the examination.
References
- KSN Reddy — Essentials of Forensic Medicine & Toxicology (textbook)
- BV Subrahmanyam — Modi's Medical Jurisprudence and Toxicology (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 35-year-old man is brought to the casualty by police, having been in custody for 48 hours on suspicion of theft. He is hunched, avoids eye contact, and initially refuses to speak. When you examine him, you find extensive contusions over his lower back and thighs, linear patterned bruises consistent with cane impacts, bilateral swelling of the soles of his feet with no external skin breaks, and tenderness along the wrists bilaterally. He whispers that 'they hurt me' but then falls silent. You are being asked by the officer present to give him a 'fitness for detention' clearance. How do you proceed — and what are your obligations under Indian law and international human rights standards?
WHY THIS MATTERS
Torture is not a distant abstraction — it occurs in Indian custodial settings, and the forensic physician is frequently the only professional with access to both the survivor and the evidence. The duty of the doctor in this context is not merely clinical: it is a legal obligation under NHRC guidelines, an ethical imperative under medical professionalism standards, and a contribution to the accountability mechanisms that prevent torture. Custodial deaths trigger mandatory NHRC reporting; torture survivors require specialist rehabilitation; and the medicolegal report prepared by the examining doctor is often the primary evidence in human rights proceedings before the National Human Rights Commission, High Courts under Article 226, and the Supreme Court under Article 32. Understanding both the international Istanbul Protocol and the Indian NHRC framework — and being able to apply them systematically — is a core competency for every Indian forensic physician.
RECALL
Before proceeding, bring forward the following:
- Wound classification from your earlier FM sessions: abrasion (epidermis only), contusion (blunt force with intact skin and subcutaneous haemorrhage), laceration (blunt force, irregular torn edges, tissue bridges present), and incised wound (sharp edge, clean margins). These distinctions are critical when describing torture injuries — their patterns help infer the implement and mechanism used.
- Constitutional provisions: Article 21 of the Indian Constitution — 'No person shall be deprived of his life or personal liberty except according to procedure established by law.' Supreme Court judgments (e.g. D.K. Basu v. State of West Bengal, 1997) have interpreted Article 21 to prohibit custodial torture.
- Indian Penal Code: IPC 330 — 'Voluntarily causing hurt to extort confession or to compel restoration of property.' A police officer who tortures a detainee to extract a confession is liable under IPC 330. IPC 304 applies if the victim dies.
- Basic anatomy of stress positions: suspension by the arms strains the rotator cuff and brachial plexus; falanga (beating of the soles) causes deep plantar fascia and metatarsal periosteal injury with minimal visible surface marks.
Legal and Professional Context: Why Torture Documentation Matters
Torture is defined by the United Nations Convention Against Torture and Other Cruel, Inhuman or Degrading Treatment or Punishment (UNCAT, 1984) as 'any act by which severe pain or suffering, whether physical or mental, is intentionally inflicted on a person' by or with the acquiescence of a public official, for purposes such as obtaining information, punishment, intimidation, or discrimination. The definition requires both severity of suffering AND the involvement of a state actor or someone acting in an official capacity — distinguishing it from ordinary criminal assault.
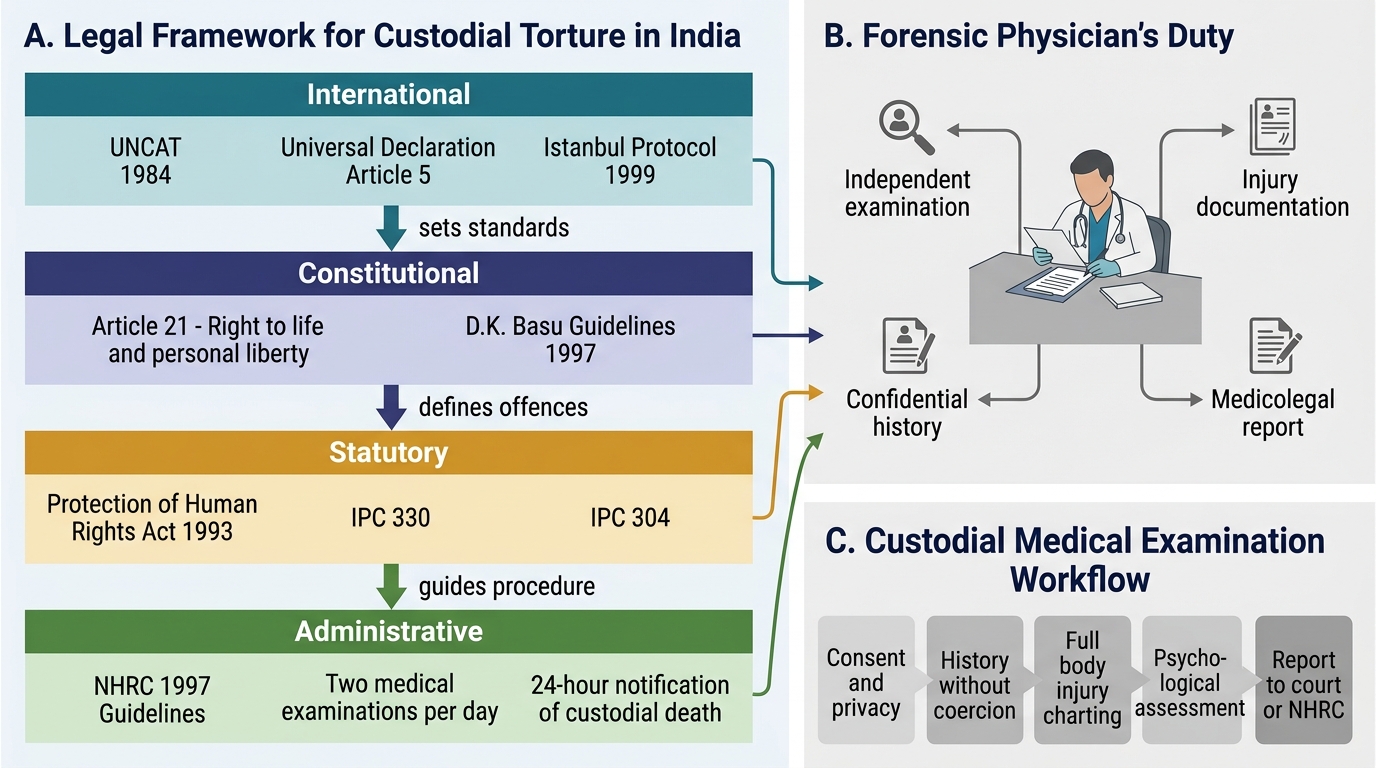
The legal framework in India spans multiple levels:
- International: Universal Declaration of Human Rights 1948 (Article 5: 'No one shall be subjected to torture or to cruel, inhuman or degrading treatment'); UNCAT 1984 — India has not formally ratified UNCAT as a treaty party, but has stated its commitment to its principles; Istanbul Protocol (1999) — the UN Manual on the Effective Investigation and Documentation of Torture, the international gold standard for forensic documentation.
- Constitutional: Article 21 (right to life and personal liberty) interpreted by the Supreme Court as prohibiting custodial torture. The landmark judgment D.K. Basu v. State of West Bengal (1997) laid down specific guidelines for arrest and detention to prevent custodial violence.
- Statutory — India: IPC 330 (voluntarily causing hurt to extort confession — cognisable offence); IPC 304 (culpable homicide if custodial death); Protection of Human Rights Act 1993 (established the National Human Rights Commission).
The professional context places the forensic physician in a dual and sometimes conflicting role. On one side is the clinical duty to assess and treat a patient; on the other is the role of impartial documenter whose findings will inform judicial and human rights proceedings. The key professional principle is that the examining doctor's primary allegiance is to the patient/survivor, not to the custodial authority. This means:
- The examination must be conducted without the police officer present in the examination room (privacy and absence of intimidation are prerequisites for a valid examination)
- The detainee must be informed of the purpose of the examination, who will receive the report, and the limits of confidentiality
- The doctor must not certify 'fit for detention' or 'no marks of violence' based on a cursory or coerced examination — this constitutes professional misconduct and potential complicity in torture
- Any pressure from custodial authorities to suppress or modify findings must be formally recorded and resisted
Legal Framework for Custodial Torture in India
SELF-CHECK
A police officer asks you to sign a 'no injury' certificate for a detainee without examining him, stating 'it's just routine.' What is the CORRECT response?
A. Sign the certificate — it is a routine administrative requirement
B. Examine the detainee thoroughly in private and document all findings accurately before issuing any certificate
C. Refuse to issue any certificate and send the detainee back without examination
D. Ask the detainee in the officer's presence whether he has any complaints
Reveal Answer
Answer: B. Examine the detainee thoroughly in private and document all findings accurately before issuing any certificate
The doctor must conduct a full, independent examination of the detainee in private (without the officer present), document all findings accurately, and only then issue a certificate reflecting the actual findings. Signing without examining is professional misconduct. Asking questions in the officer's presence is invalid because the detainee cannot answer freely. A thorough examination protects the detainee and protects the doctor from later allegations of complicity.
Governing Principles: Istanbul Protocol and NHRC Guidelines
Two governing instruments define the standards for medical documentation of torture in India: the Istanbul Protocol at the international level, and the NHRC 1997 guidelines at the national level. Both must be understood as complementary — the NHRC guidelines implement the spirit of the Istanbul Protocol within the Indian legal and custodial framework.
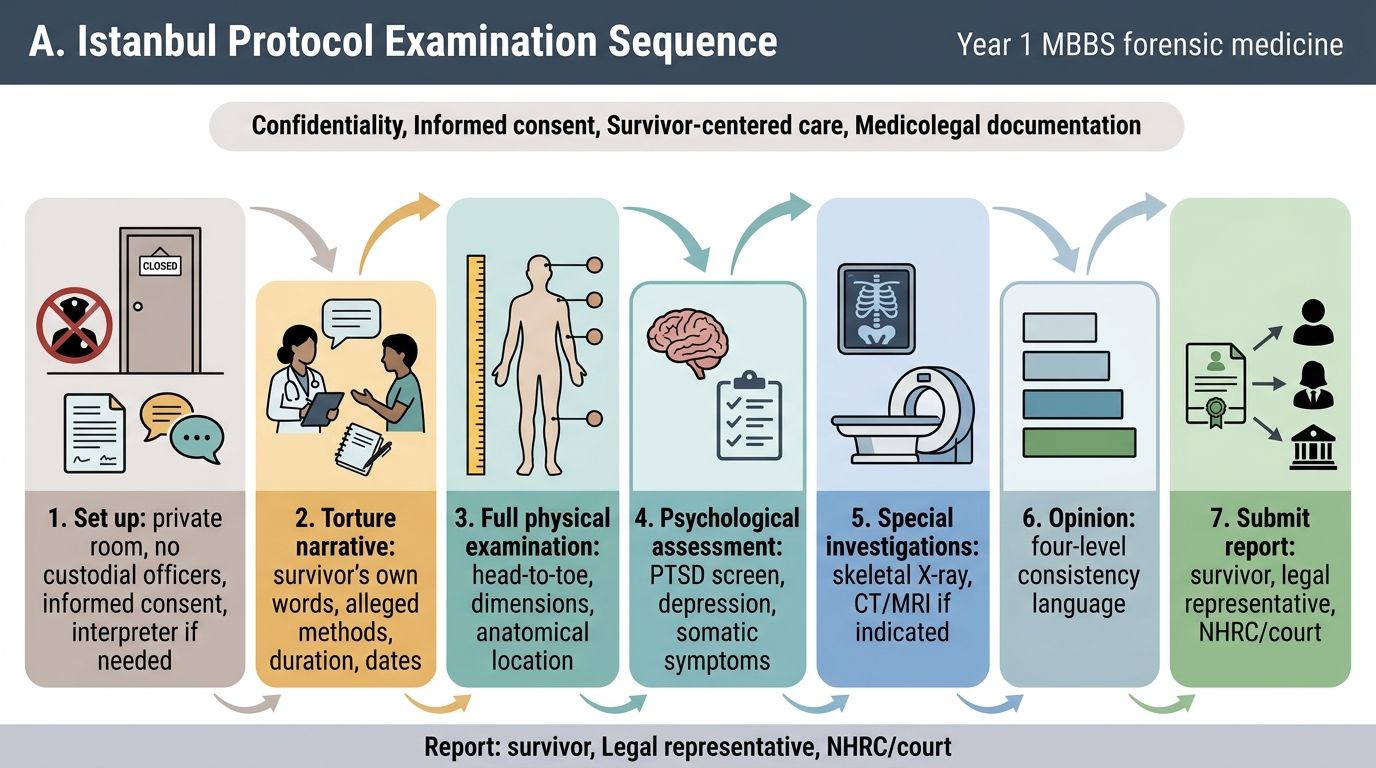
Istanbul Protocol (1999) — full name: UN Manual on the Effective Investigation and Documentation of Torture and Other Cruel, Inhuman or Degrading Treatment or Punishment — is the international gold standard. Its key requirements for medical examiners include:
- A comprehensive history: torture narrative (types of torture, duration, location, perpetrators as known to survivor), past medical history, current symptoms
- Complete physical examination with precise description of all injuries
- Psychological assessment: psychological sequelae including PTSD, depression, anxiety, functional impairment
- Assessment of the 'degree of consistency' between the physical/psychological findings and the torture allegations — the protocol requires the examiner to state whether findings are 'consistent with,' 'highly consistent with,' 'not consistent with,' or 'typical of' the alleged torture (the examiner does NOT conclude definitively — that is the tribunal's role)
- Examination should be completed within 72 hours of acute torture where possible; for historical torture the timeline is less critical
- The report must be given to the survivor, to their legal representative, and to the relevant human rights body
NHRC 1997 Guidelines — India's National Human Rights Commission issued specific guidelines for the prevention of custodial torture and the conduct of medical examinations in custody. Key requirements:
- Two medical examinations per day for every person in custody (on admission and daily while in custody) by a government medical officer
- Pre-custody examination (before the person enters police custody) to document baseline status and any pre-existing injuries
- Post-custody examination (immediately on release from custody) to document any injuries acquired during custody
- Video recording of custodial interrogation periods (police custodial violence prevention)
- Custodial death protocol: the NHRC must be notified within 24 hours of any death in custody; a post-mortem examination is mandatory; the report must be submitted to the NHRC within 24 hours
- The examining medical officer must be independent from the custodial authority — preferably a government medical officer with no administrative subordination to the police
| Feature | Istanbul Protocol (International) | NHRC Guidelines 1997 (India) |
|---|---|---|
| Scope | All forms of torture globally | Indian custodial settings |
| Examination frequency | Acute ≤72 h; historical as available | Two examinations per day in custody |
| Custodial death | Document and report | Notify NHRC within 24 h; mandatory PM |
| Video recording | Recommended | Required for interrogation periods |
| Report recipients | Survivor + legal representative + human rights body | NHRC + court + survivor |
| Consistency language | Standardised 4-level scale | Mirrors Istanbul Protocol approach |
Legal architecture — India:
- Protection of Human Rights Act 1993 — established the NHRC; gives it powers to inquire into complaints of human rights violations; can summon medical records and order investigations
- IPC 330 — voluntarily causing hurt to extort confession; applies to custodial interrogators who use violence
- D.K. Basu guidelines (Supreme Court 1997) — 11 specific requirements including written arrest memo, medical examination every 48 hours, and informing a relative — these guidelines, though not yet a statute, are binding on police under Article 21
Istanbul Protocol Examination Sequence
SELF-CHECK
Under NHRC 1997 guidelines, how many medical examinations per day must be conducted for a person in police custody, and what is the timeframe for notifying NHRC of a custodial death?
A. One examination per day; NHRC notification within 72 hours
B. Two examinations per day; NHRC notification within 24 hours
C. One examination per day; NHRC notification within 48 hours
D. Two examinations per day; NHRC notification within 72 hours
Reveal Answer
Answer: B. Two examinations per day; NHRC notification within 24 hours
NHRC 1997 guidelines require two medical examinations per day for persons in custody. In the event of a custodial death, the NHRC must be notified within 24 hours, and a mandatory post-mortem examination must be conducted with the report submitted to NHRC within 24 hours.
Method and Documentation: Examining the Torture Survivor
The systematic examination of a person who has been tortured or is alleged to have been tortured in custody requires a structured approach that simultaneously serves clinical care and evidence documentation. The reliability of the medicolegal report depends entirely on the thoroughness and precision of the examination itself.
Setting up the examination is the first practical step. The examination must occur in a private room, without custodial officers present. The survivor must be informed that the purpose is both medical and medicolegal, and that findings will be documented for potential use in human rights or legal proceedings. The survivor's consent must be obtained — if the survivor refuses examination, this refusal must itself be documented. An interpreter should be used if language is a barrier.
History-taking in torture cases follows the Istanbul Protocol structure:
- Torture narrative: The survivor's account should be recorded in their own words, including the types of torture methods used, their sequence, their frequency, the duration of each episode, and the period in custody during which they occurred. Note: the examiner does not evaluate credibility — that is the judicial function; the examiner records what is stated.
- Somatic complaints: Current symptoms — pain (location, character, severity), sleep disturbance, appetite, bowel/bladder function, sexual function.
- Psychological complaints: Nightmares, flashbacks, hypervigilance, avoidance behaviours, mood — preliminary screen for PTSD.
- Past medical history: Pre-existing conditions that may affect injury interpretation.
Physical examination must be systematic, head to toe. Key points for torture-specific injuries:
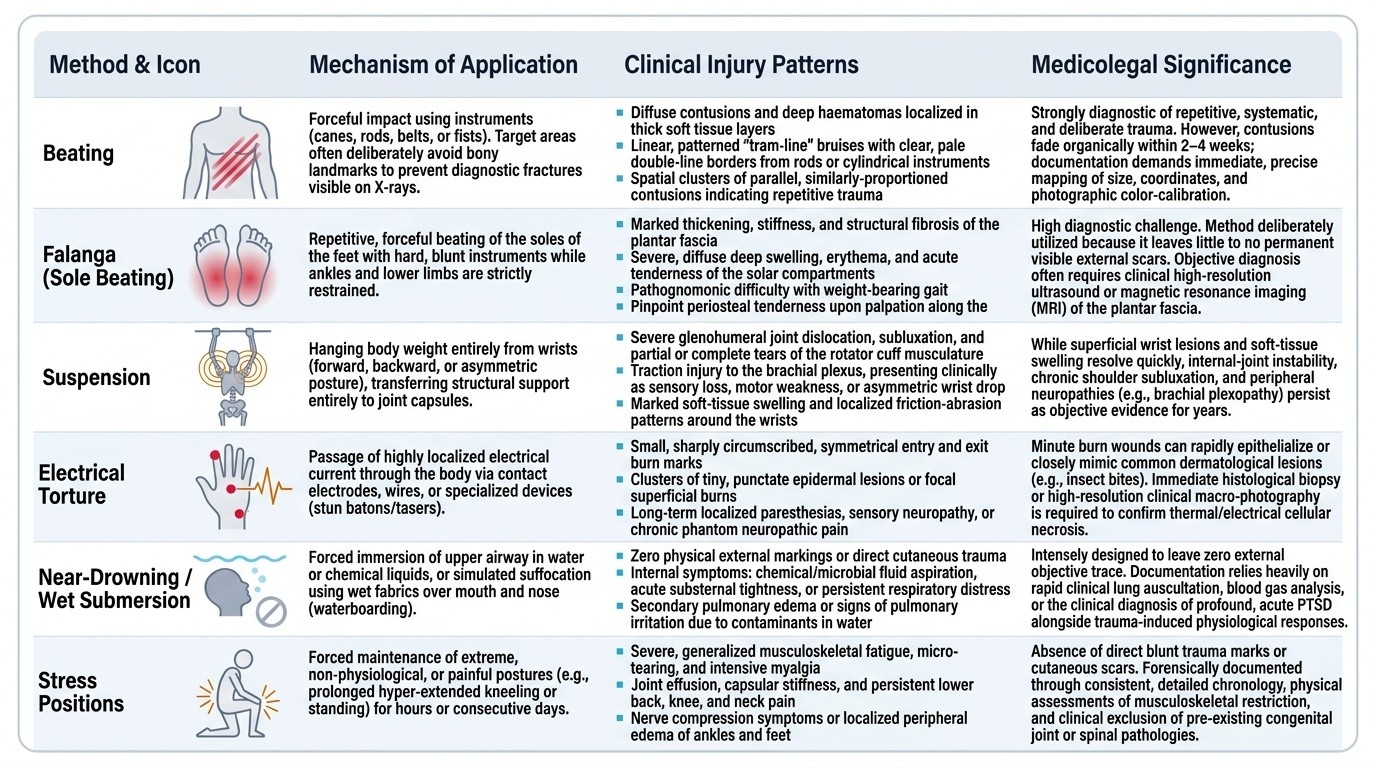
- Beating injuries: contusions over soft tissue areas (avoiding bony prominences — suggesting deliberate avoidance of fracture-causing impacts that would show on X-ray); linear patterned bruises from canes, belts, or rods; grouped, parallel, similarly-sized contusions suggesting repeated instrument use.
- Falanga (beating of the soles of the feet): a common torture method precisely because it leaves minimal visible evidence. Look for diffuse swelling and tenderness of the plantar surface, thickened plantar fascia, difficulty weight-bearing, periosteal tenderness over metatarsals. X-ray may show periosteal reaction.
- Suspension injuries: shoulder girdle tenderness, brachial plexus stretch signs (diminished sensation/motor power in ulnar/radial distribution), wrist marks if suspended by bound wrists.
- Electrical torture: small, circular, punched-out entry wounds (1–2 cm), usually in sensitive areas (genitals, soles, gums, fingertips); exit marks or diffuse tissue damage; burns may heal leaving depigmented scars.
- Near-drowning, suffocation, stress positions: may leave NO visible marks — the absence of physical signs does not negate the torture allegation; psychological documentation then becomes the primary evidence base.
- Sexual torture: detailed external genital/anal examination; injuries must be documented with the same precision as for forensic sexual assault examination; chain of custody for any samples.
Psychological assessment is a mandatory component of the Istanbul Protocol examination. Preliminary clinical assessment should screen for:
- Post-Traumatic Stress Disorder (PTSD): hyperarousal, re-experiencing (flashbacks, nightmares), avoidance; these are expected sequelae of systematic torture
- Depression: hopelessness, anhedonia, cognitive slowing
- Somatic symptoms: unexplained chronic pain, headaches, gastrointestinal complaints — 'souvenir pain' (persistent pain that outlasts the healing of physical injuries) is a documented sequela of torture
Injury dating uses the same principles as general forensic wound assessment; additionally, the examiner should note whether injuries at different stages of healing are consistent with torture alleged on different dates in the custody narrative.
Provided image
Applied Practice: Professionalism, Rehabilitation, and the Medicolegal Report
The forensic physician examining a torture survivor demonstrates professionalism not merely through technical accuracy but through the entire interaction — how the examination is conducted, how findings are communicated, what referrals are arranged, and how the medicolegal report is prepared and protected. Each of these dimensions has both ethical and legal weight.
Provided image
Demonstrating professionalism with survivors of torture and human rights violations (FM9.4) involves recognising that the person before you has experienced severe, deliberate harm by agents of authority — often the very same type of authority that may be present outside the examination room. This creates a profound vulnerability and a professional obligation to create conditions of safety and trust:
- Communication: Explain every step of the examination before performing it. Avoid unexpected or sudden physical contact. Use a calm, unhurried tone. Acknowledge suffering without projecting — do not tell the survivor how they 'must be feeling.'
- Privacy and dignity: Examination always without custodial officers present; use a gown or draping as clinically appropriate; never expose more of the body than is necessary for the examination.
- Confidentiality and its limits: Inform the survivor that findings will be documented and shared with courts, NHRC, and potentially their legal representative — this is not optional, and it must be explained before examination begins, not after.
- Avoiding re-traumatisation: Do not press for graphic torture details beyond what is forensically necessary; if the survivor dissociates, becomes highly distressed, or terminates the examination, respect this and document it.
- Psychological first aid: Even within the examination, simple measures (water, a moment to compose themselves, acknowledging their courage in providing information) reduce immediate distress.
Rehabilitation referral is a clinical obligation. Torture survivors require:
- Psychiatric/psychological consultation — PTSD treatment (trauma-focused CBT, EMDR where available), antidepressant therapy if indicated
- Pain management for chronic souvenir pain — multi-disciplinary pain clinic referral
- Physiotherapy for musculoskeletal sequelae (falanga, suspension injuries)
- Social work support — addressing detention-related social disruption, family support, legal aid linkage
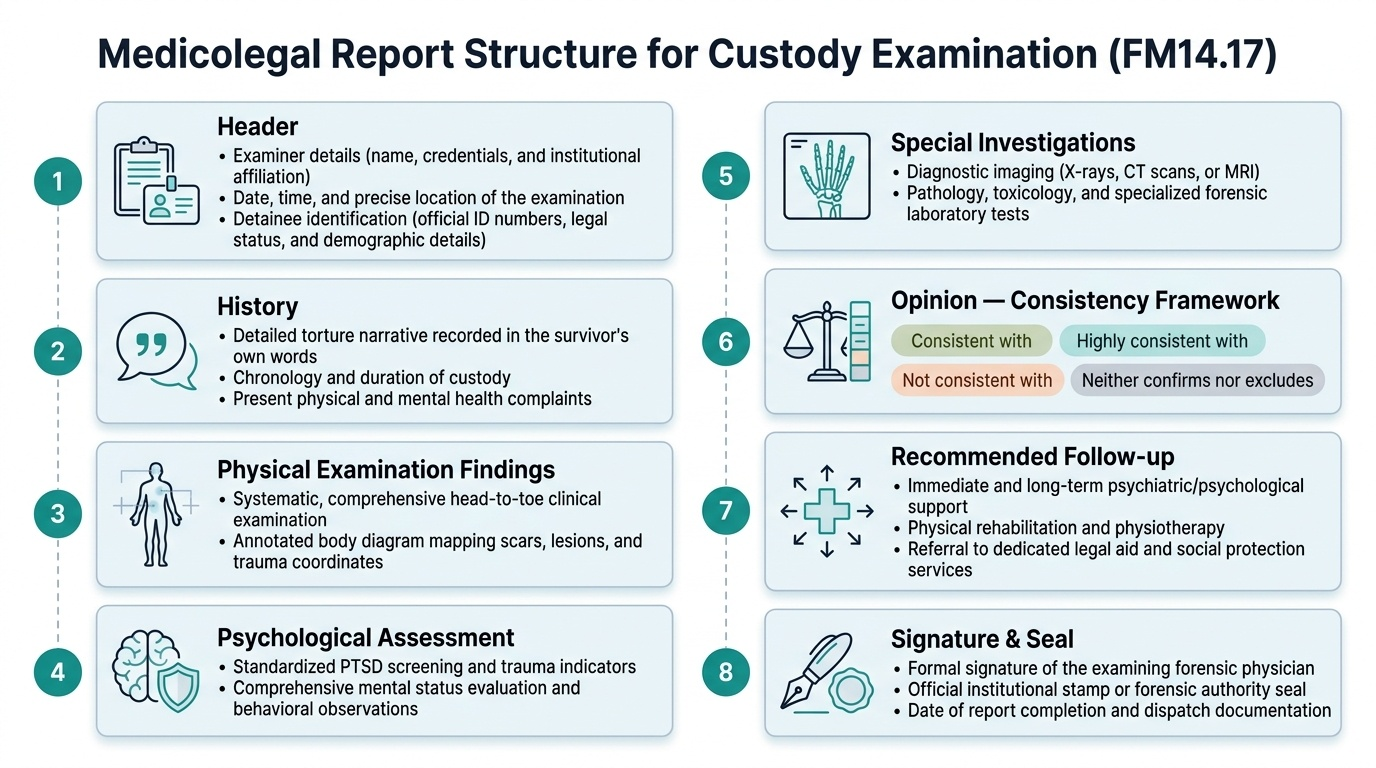
Preparing the medicolegal report for court or NHRC (FM14.17) follows a standardised format. The report must include:
1. Header: Name, designation, and institutional affiliation of the examining doctor; date, time, and place of examination; identification of the person examined (name, age, sex, custody number if applicable); who referred the person for examination
2. History section: Torture narrative (in survivor's words with quotation marks), duration of custody, alleged perpetrators, types of torture alleged, present complaints
3. Physical examination findings: Systematic head-to-toe findings with all injuries precisely described (anatomical location, dimensions in cm, shape, colour, margins, associated findings); body diagram annotated; fundoscopic findings; neurological findings if relevant
4. Psychological assessment findings: Brief mental status examination; preliminary PTSD screen results; referral recommended
5. Special investigations: X-ray findings (fractures, periosteal reaction), CT/MRI if performed, pathology results
6. Opinion section — the most important part of the report:
- For each alleged torture method, state whether the physical and/or psychological findings are: (a) consistent with the allegation, (b) highly consistent with or typical of the allegation, (c) not consistent with the allegation, or (d) neither confirm nor exclude (when no visible injury is expected)
- The examiner must NOT conclude guilt or innocence — only consistency between findings and allegations
- State any alternative explanations considered and whether they are plausible
7. Recommended follow-up: psychiatric referral, physiotherapy, legal aid
8. Signature, date, seal
Handling conflicts with custodial authorities is a practical skill: if an officer attempts to enter the examination room, the doctor states clearly that international standards (Istanbul Protocol) and NHRC guidelines require examination without custodial presence. If the officer insists, this must be recorded in the report as an interference with the examination. If threatened, the doctor documents this and reports to the relevant medical regulatory body and NHRC. The examining doctor's independence is non-negotiable — compromising it compromises the entire evidentiary value of the report.
CLINICAL PEARL
The consistency framework is the backbone of the medicolegal opinion. Use the Istanbul Protocol's four-level language precisely: (1) 'Consistent with' — the injury could have been caused by the alleged torture but is not specific to it; (2) 'Highly consistent with' — the injury is typical of the alleged mechanism and unusual in other contexts (e.g. falanga causing diffuse plantar swelling without surface marks); (3) 'Not consistent with' — the findings actively contradict the allegation; (4) 'Neither confirm nor exclude' — for methods leaving no physical mark (near-drowning, stress positions). Never write 'patient was tortured' as a conclusion — the medical report establishes the evidential foundation; the tribunal draws the legal conclusion.
SELF-CHECK
A torture survivor shows bilateral plantar swelling with difficulty weight-bearing but NO skin break or external bruising on the soles. X-ray shows periosteal reaction on metatarsals. Using Istanbul Protocol language, how should this be categorised in the medicolegal opinion?
A. Not consistent with torture — no visible marks on skin
B. Highly consistent with falanga (sole beating), as this injury pattern is typical of this specific torture method
C. Consistent with accidental injury only
D. Cannot be commented upon without a confession
Reveal Answer
Answer: B. Highly consistent with falanga (sole beating), as this injury pattern is typical of this specific torture method
Falanga (beating of the soles) characteristically produces deep plantar fascia and periosteal injury with minimal or absent external skin marks — this is precisely what makes it a preferred method (it is hard to detect on casual examination). The combination of bilateral plantar swelling, weight-bearing difficulty, and periosteal reaction on metatarsals, in a person alleging custody beatings, is 'highly consistent with falanga' per the Istanbul Protocol — this injury pattern is typical of this specific method and unusual in accidental contexts.
KEY TAKEAWAYS
Torture, Custody Examination & Human-Rights Protocols — Key Points:
- Torture definition (UNCAT 1984): severe physical or mental suffering intentionally inflicted by or with acquiescence of a public official — requires both severity AND state-actor involvement.
- Istanbul Protocol (1999): UN Manual on Effective Investigation and Documentation of Torture — international gold standard; requires comprehensive history, full physical examination, psychological assessment, and a structured opinion using four-level consistency language.
- NHRC 1997 Guidelines (India): two medical examinations per day for all persons in custody; pre- and post-custody examinations; custodial death notification within 24 hours; mandatory post-mortem; video recording of interrogation periods.
- Indian legal framework: Protection of Human Rights Act 1993 (NHRC), IPC 330 (hurt to extort confession), IPC 304 (culpable homicide if death), Article 21 Constitution (right to personal liberty), D.K. Basu guidelines (1997).
- Professionalism with survivors: examination in private without custodial officers; no re-traumatisation; psychological first aid; full explanation before examination; rehabilitation referral (psychiatric, physiotherapy, social work).
- MLR structure (FM14.17): header, torture narrative, physical examination, psychological assessment, special investigations, opinion section (consistency framework), referrals, signature.
- Opinion language: 'Consistent with' / 'Highly consistent with' / 'Not consistent with' / 'Neither confirms nor excludes' — never conclude guilt; establish the evidential foundation only.
- Falanga: minimal visible marks despite deep plantar injury — a classic trap; periosteal reaction on metatarsal X-ray is the key finding.
REFLECT
Imagine you have completed a careful examination of a torture survivor in custody, and your findings are highly consistent with the methods he has alleged. As you write the report, the senior police officer in charge of the case approaches you privately and says: 'Doctor, for everyone's benefit, can you just write that there are no marks of violence? This man is dangerous.' Reflect on: What is at stake for the survivor if you comply? What are your legal obligations and the professional consequences of compliance versus non-compliance? How would you respond to the officer, and what would you document? What support systems (legal, professional, human rights mechanisms) are available to you in this situation?