Page 9 of 14
FM2.4 | Organ Transplantation Law & Ethics (THOTA) — SDL Guide
Learning Objectives
- Describe the historical context and rationale for the Transplantation of Human Organs and Tissues Act 1994 (THOTA)
- Outline the salient features of THOTA 1994 and its 2011 amendment, including key changes introduced by the amendment
- Describe the living donor and deceased donor (brain-death) pathways under THOTA
- Discuss the ethical issues in organ donation: voluntary consent, equity, commercialisation, and donor protection
INSTRUCTIONS
Organ transplantation saves lives — but it also creates unique opportunities for exploitation. The kidney is a commodity in underground markets; living donors have been coerced or deceived; deceased donor organs have been harvested without proper consent. India's history with organ transplantation abuses in the 1990s directly shaped the legislative response: the Transplantation of Human Organs Act 1994, significantly amended in 2011, which governs everything from who can donate, to how brain death is certified, to the penalties for commercial dealing. As a future doctor, you need to know this Act: you may be part of a brain-death certification team, you may counsel a family considering donation, and you may encounter ethical dilemmas that have no easy answer.
References
- KSN Reddy — Essentials of Forensic Medicine & Toxicology (textbook)
- BV Subrahmanyam — Modi's Medical Jurisprudence and Toxicology (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 42-year-old policeman is admitted to an ICU following a massive road traffic accident and severe traumatic brain injury. After 48 hours of intensive care, he shows no brainstem reflexes, has no respiratory effort on the ventilator, and the CT scan shows catastrophic bilateral hemispheric destruction. His wife and two adult children are devastated. The neurologist gently raises the possibility of organ donation. The intensivist, the hospital's transplant coordinator, and the family all turn to you — the registrar — to understand what happens next. Who certifies brain death? What does consent require? Can the family refuse? Can organs be procured? What law governs all of this, and how does it protect the donor, the recipient, and the doctor?
WHY THIS MATTERS
India faces a massive and widening gap between organ demand and supply. Approximately 200,000 patients develop end-stage renal disease annually; an estimated 50,000-60,000 need liver transplants; thousands more need hearts, lungs, and pancreata. Against this, only around 15,000-17,000 transplants are performed per year, with deceased donor rates far below those in comparable nations. The deficit is a product of multiple factors: inadequate organ donation infrastructure, low brain-death certification rates in ICUs, and public trust deficits shaped by historical commercial exploitation. The legal framework — THOTA 1994 as amended in 2011 — is the attempt to create a system that is safe for donors, fair for recipients, and transparent enough to earn public confidence. Understanding THOTA is essential for every doctor in any clinical setting where organ donation may arise.
RECALL
Recall from fp1: brain death is the irreversible cessation of all functions of the entire brain including the brainstem, and is legally recognised as death in India under THOTA. The criteria for brainstem death (absent brainstem reflexes, apnoea test with PaCO2 ≥60 mmHg, exclusion of reversible causes) are the medical standard that the THOTA certification board applies. Also recall from fp2: the manner-of-death classification — a brain-dead patient died of a natural or accidental cause; the organ donation process follows after death is certified, not as a cause of death. From Year 1 ethics and communication: the four principles of medical ethics (Beauchamp and Childress) — autonomy, beneficence, non-maleficence, and justice — these will be applied directly to the ethical analysis of organ donation in this module.
The Medicolegal Context: Why Organ Transplantation Needs Legal Regulation
Modern organ transplantation began in India in the 1970s, with renal transplantation at CMC Vellore and AIIMS pioneering the field. For the first two decades, there was no specific legislation. The consequences were severe: by the early 1990s, a commercial kidney market had emerged in India — particularly in Tamil Nadu — where poor, often illiterate individuals were recruited, paid (or sometimes unpaid), and coerced into donating kidneys for wealthy Indian and foreign recipients. The 'kidney scandals' of the early 1990s — documented extensively by investigative journalists and medical researchers — revealed that some hospitals were effectively operating commercial organ farms. Donors reported being deceived about the nature of the procedure, given inadequate follow-up care, and paid amounts that were far less than promised.
The Indian government's response was the Transplantation of Human Organs Act 1994 (THOTA) — one of the first developing-country statutes specifically addressing organ donation. The Act established the legal framework for transplantation, created the concept of 'near-relative' living donation, banned commercial trade, and crucially, created a legal definition of brain death to enable deceased donor transplantation. Brain death had been used clinically since the 1960s (following the Harvard Medical School criteria, 1968) but had no legal recognition in India before THOTA.
The global context for organ regulation includes the Declaration of Istanbul (2008) — an international consensus document on transplant tourism and commercialisation — and WHO's guiding principles on human cell, tissue, and organ transplantation. India's THOTA and its 2011 amendment align with these international standards.
Provided image
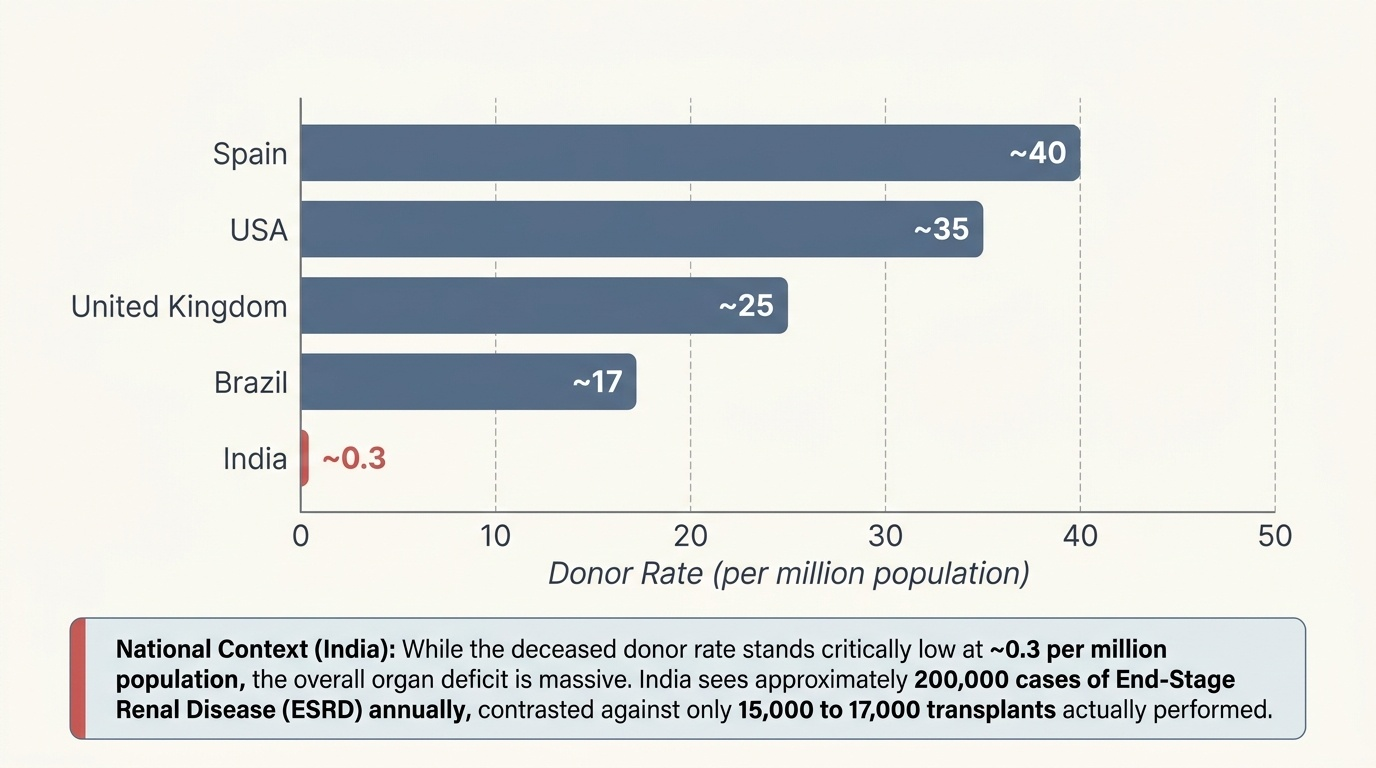
The scale of India's organ deficit (key epidemiological facts from Reddy's FM&T):
- Approximately 200,000 new end-stage renal disease cases per year
- Deceased donor rate: approximately 0.1-0.5 per million population (compared to 30-40 per million in Spain or USA)
- The low deceased-donor rate means living donors (predominantly related) constitute the majority of all transplants in India
- NOTP and NOTTO were created under the 2011 amendment specifically to improve deceased donor rates through better coordination
THOTA 1994 and the 2011 Amendment: Key Provisions
The Transplantation of Human Organs and Tissues Act 1994 (THOTA) is the primary legislation governing organ and tissue donation and transplantation in India. It applies to all registered hospitals performing transplantation. Key provisions of the original 1994 Act and the important changes introduced by the 2011 amendment are described below.
Original THOTA 1994 — key provisions:
- Legal recognition of brain death as a valid basis for organ procurement (Section 2(c) definition of 'brain death')
- Certification of brain death by a four-doctor board (doctor in charge of the hospital/nominee, doctor in charge of the patient, a neurologist or neurosurgeon, and a government-appointed medical officer)
- Living donation permitted only to near-relatives (defined as spouse, son, daughter, father, mother, brother, sister)
- Registration of hospitals for transplantation (hospitals must be authorised)
- Prohibition of commercial trade in human organs — criminal offence (imprisonment + fine)
- Consent for donation must be voluntary and free of coercion
THOTA 2011 Amendment — key changes:
1. Expanded definition of 'near relative': the 2011 amendment added grandparents and grandchildren to the near-relative definition, enabling a wider range of related living donors
2. Introduction of NOTP (National Organ Transplant Programme): a national coordination framework under the Ministry of Health and Family Welfare, with the NOTTO (National Organ and Tissue Transplant Organisation) as the apex registry for deceased donor organ allocation
3. Swap (paired exchange) transplantation: the 2011 amendment explicitly permitted swap transplantation — when a near-relative donor is ABO-incompatible with their intended recipient, two incompatible pairs can exchange donors. This is a practical solution to blood group incompatibility without resorting to commercial procurement
4. Inclusion of tissues: the Act's scope was extended explicitly to include tissues (eyes, skin, bone marrow, blood vessels, heart valves) in addition to solid organs
5. Enhanced penalties for commercial dealing: penalties for commercial trading in organs were substantially increased
6. Expanded role of the authorisation committee: better oversight mechanisms for non-relative living donation
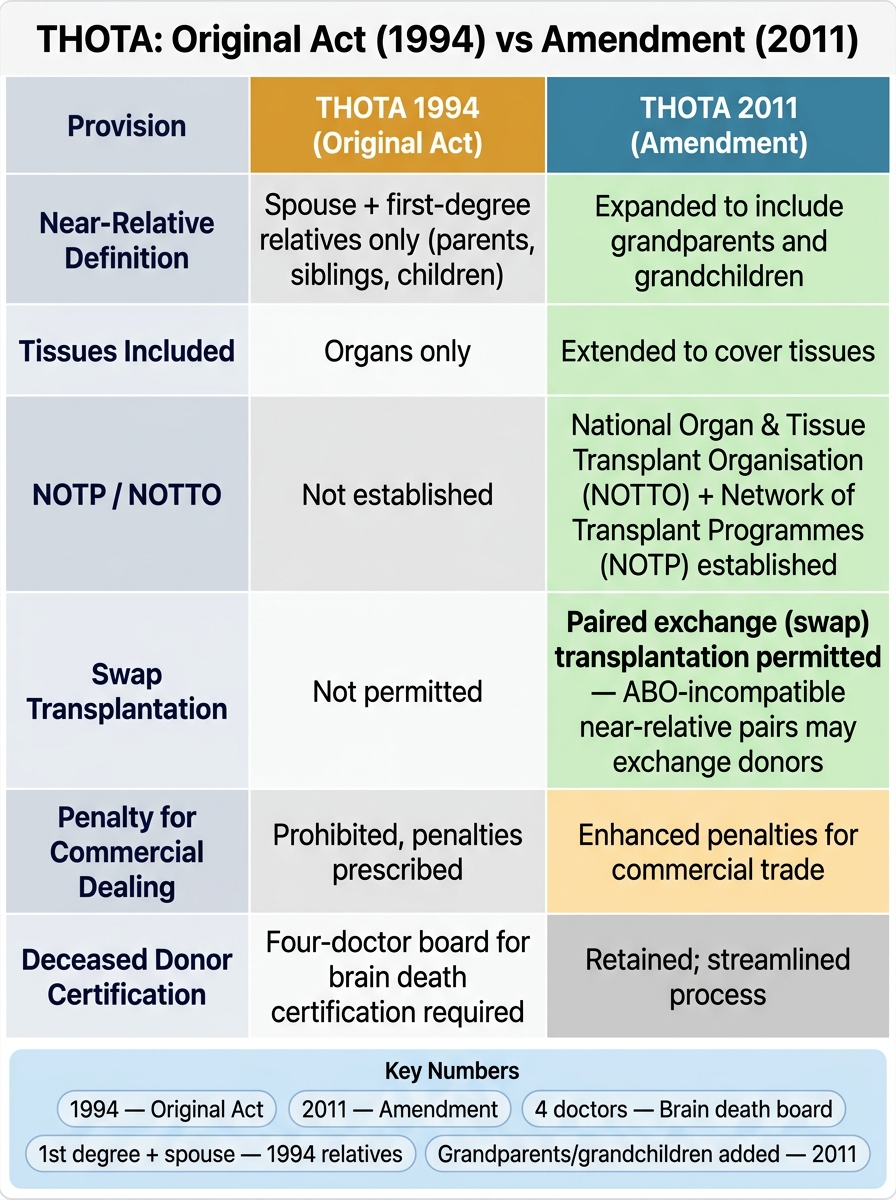
THOTA 1994 vs 2011 Amendment: Key Legislative Changes
Key THOTA numbers to remember:
- Original Act year: 1994
- Amendment year: 2011
- Brain death certification: four-doctor board
- Original near relatives: spouse + first-degree relatives only
- 2011 addition: grandparents + grandchildren
SELF-CHECK
Under THOTA as amended in 2011, which of the following was a NEW provision introduced by the amendment that was NOT present in the original 1994 Act?
A. Prohibition of commercial trade in human organs
B. Legal recognition of brain death for organ procurement
C. Swap (paired exchange) transplantation
D. Requirement of a four-doctor board for brain death certification
Reveal Answer
Answer: C. Swap (paired exchange) transplantation
Swap (paired exchange) transplantation — where two ABO-incompatible near-relative donor pairs exchange donors — was introduced by the 2011 amendment and was not present in the original 1994 Act. The prohibition of commercial trade, legal recognition of brain death, and the four-doctor board requirement were all part of the original 1994 Act. The 2011 amendment also expanded the near-relative definition, established NOTP/NOTTO, extended the Act to cover tissues, and enhanced penalties.
Living and Deceased Donor Pathways Under THOTA
THOTA provides for two distinct donor pathways, each with specific legal requirements for consent, certification, and process.
Living Donor Pathway
Living organ donation is permitted only from:
1. Near relatives (as defined in THOTA post-2011: spouse, son, daughter, father, mother, brother, sister, grandparents, grandchildren) — these require consent from the donor and approval by the hospital's transplant team, but do NOT require approval from the Authorisation Committee
2. Non-relatives (donors with an 'emotional relationship' — e.g. a close friend) — these require approval by the Authorisation Committee (a regulatory body set up under the Act) to ensure the donation is voluntary and not commercial
3. Swap donors — near-relative pairs in ABO-incompatible situations can exchange; this requires Authorisation Committee approval
The living donor must:
- Be ≥18 years of age (mentally competent adults)
- Give free, voluntary, informed consent — no coercion, no payment, no deception
- Undergo medical assessment to confirm fitness for donation (the donor's health must not be significantly compromised by the donation)
- Have the risks of donation (surgical risk, long-term functional impact) explained in full
Deceased Donor (Brain-Dead) Pathway
Deceased donor organ procurement is only possible after formal brain death certification under THOTA:
1. The patient must be on mechanical ventilation (the heart is still beating)
2. A known irreversible structural cause of brain damage must be identified
3. Reversible causes must be excluded (hypothermia, metabolic derangements, drugs)
4. Brainstem death testing must be performed (absent brainstem reflexes + apnoea test — see fp1)
5. Testing must be performed and confirmed by two independent sets of evaluations at an appropriate interval, certified by the four-doctor board
After brain death certification:
- The family is informed and consent for organ donation is requested — under current Indian law, family consent is required (there is no presumed consent or opt-out system in India, unlike Spain or the UK)
- If consent is given, the NOTTO regional registry is notified and organ allocation begins
- The transplant team manages organ procurement while the ventilator continues
- After procurement, the ventilator is switched off and a death certificate is issued
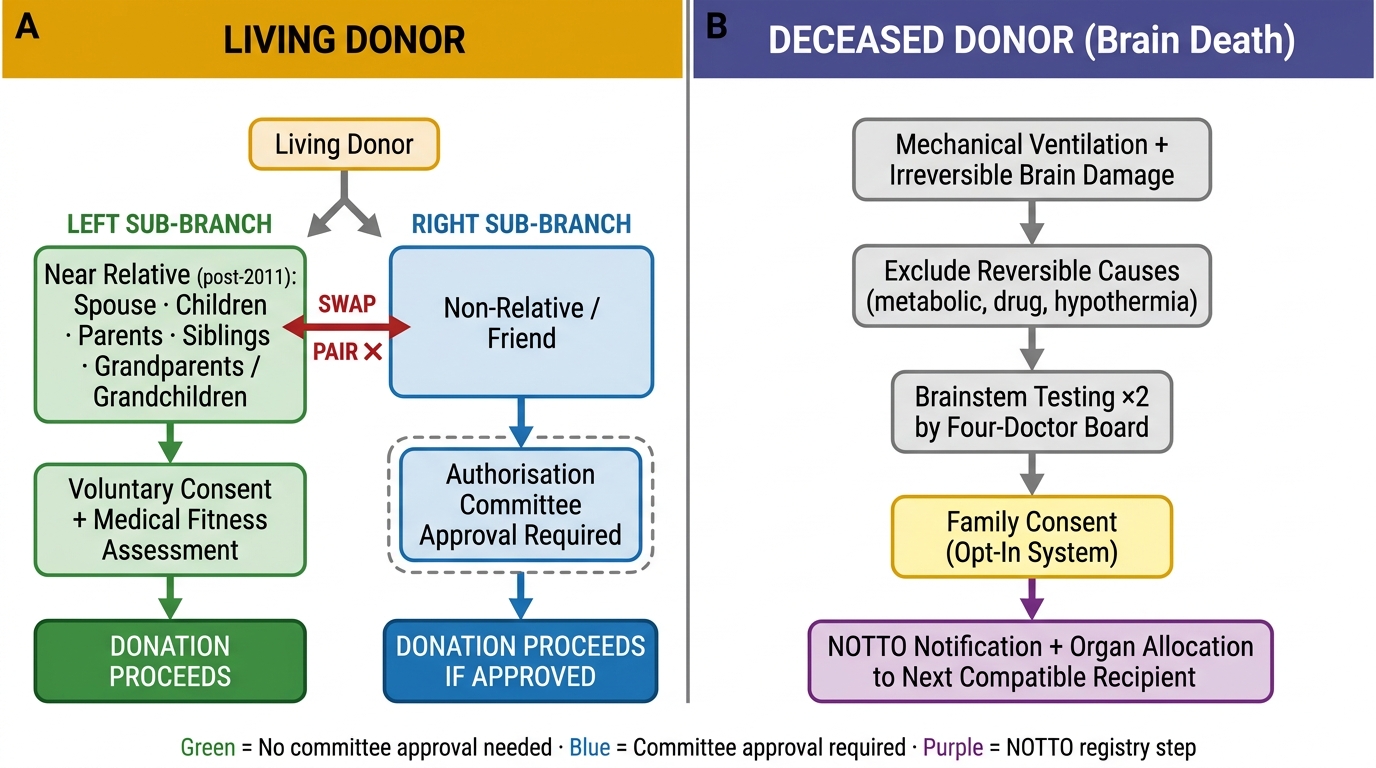
Organ Donation Pathways Under THOTA 1994 (Amended 2011)
- Living donors: near-relatives do not need Authorisation Committee approval; non-relatives do
- Deceased donors: brain death + four-doctor board + family consent (opt-in system in India)
- NOTTO manages the allocation registry — organs go to the next compatible patient on the waiting list, not to the highest bidder
SELF-CHECK
A 32-year-old man wishes to donate a kidney to his best friend of 20 years who is on dialysis. They are not related. Under THOTA 2011, what is required before this donation can proceed?
A. No special approval needed — living donation between consenting adults is always permitted
B. Approval from the Authorisation Committee to verify the donation is voluntary and not commercial
C. Brain death certification of the donor
D. Approval from the State Transplant Authority only, not the Authorisation Committee
Reveal Answer
Answer: B. Approval from the Authorisation Committee to verify the donation is voluntary and not commercial
Under THOTA, living donation to a non-relative (even a close friend) requires Authorisation Committee approval to verify that the donation is genuinely voluntary, that no commercial transaction is involved, and that the stated relationship and motive are genuine. This safeguard was introduced specifically to prevent exploitation under the guise of 'friendship'. Near-relatives (as defined in THOTA) do not require Authorisation Committee approval. Brain death certification applies to deceased donors, not living donors. The State Transplant Authority is a broader regulatory body, but the specific approval mechanism for non-relative living donation is the Authorisation Committee.
CLINICAL PEARL
India's opt-in system and the family consent problem. Unlike Spain, Wales, and several other countries that have moved to an 'opt-out' (presumed consent) system — where everyone is presumed to be a donor unless they have previously registered an objection — India retains an opt-in system, meaning family consent is required even if the deceased had signed a donor card or registered as a donor. This creates a significant tension: a doctor who has certified brain death and obtained a donor card cannot proceed without the family's agreement, even though the deceased expressed their wish to donate. Reform advocates argue for an opt-out system to increase the donor pool; opponents raise concerns about informed community consent and cultural/religious sensitivities around body integrity after death. This is a live ethical debate, and you should be able to articulate both positions.
Ethical Issues in Organ Donation: Autonomy, Equity, and Commercialisation
Organ transplantation sits at the intersection of the most fundamental ethical tensions in medicine. A full ethical analysis requires applying the four principles of medical ethics — autonomy (the donor's right to decide), beneficence (benefit to the recipient), non-maleficence (protection of the donor from harm), and justice (equitable allocation) — to a situation where the interests of donor, recipient, and society may conflict.
Autonomy in organ donation:
For living donors, autonomy requires that consent is free and informed — the donor must understand the nature of the surgery, the risks (both immediate and long-term), and their right to withdraw without consequence. The concern is that genuine autonomy is difficult when financial pressure, family obligation, or social coercion shapes the 'decision'. A poor person donating a kidney to pay off debt may sign a consent form, but their autonomy is compromised. THOTA's prohibition on payment and the Authorisation Committee oversight are designed to protect genuine autonomy.
For deceased donors, the ethical question is whether the family's 'veto' power over the deceased's expressed wish to donate respects or undermines the principle of autonomy. The donor registered their choice; overriding it at the family's request is an autonomy violation — but demanding that families surrender a loved one's organs against their wishes at an already traumatic moment is also a significant harm.
Justice and equitable allocation:
Organ allocation in India, coordinated through NOTTO and regional registries, is based on compatibility (ABO, HLA), clinical urgency, and waiting time. The system aims to be fair — but in practice, access to transplantation is heavily stratified by ability to pay for the transplant surgery, post-operative immunosuppression, and the quality of the transplant centre. A poor patient on the government waiting list and a wealthy patient at a private centre may both be listed, but their access to care pre- and post-transplant is not equal. Justice demands attention to these systemic inequities.
Commercialisation and organ trafficking:
The core prohibition of THOTA — the ban on payment for organs — reflects the principle that the human body should not be treated as a commodity. The arguments for legalised compensation for donors are occasionally made (a compensated living donor market, as in Iran, the only country with such a system). The arguments against are stronger: payment inevitably attracts the most economically vulnerable donors, who may make decisions under duress; the concept of truly voluntary informed consent is undermined when financial desperation is the motivating factor; and paid systems have been shown to exploit donors who receive inadequate medical care after donation. THOTA's criminal penalties for organ trading reflect India's formal commitment to the non-commercialisation principle.
Ethical issues specific to living donor surgery:
- The donor is a healthy person undergoing major surgery solely for the benefit of another person; the risk is entirely one-sided in terms of surgical harm (only the donor is harmed; only the recipient benefits in the immediate sense)
- Non-maleficence demands that this risk is minimised (laparoscopic donor nephrectomy has substantially reduced operative morbidity) and that donors are given lifelong follow-up
- The principle of 'first, do no harm' (primum non nocere) is directly challenged by the act of cutting open a healthy person
- This ethical tension is resolved only by the principle of donor autonomy (if truly voluntary) and the weight of benefit to the recipient and society
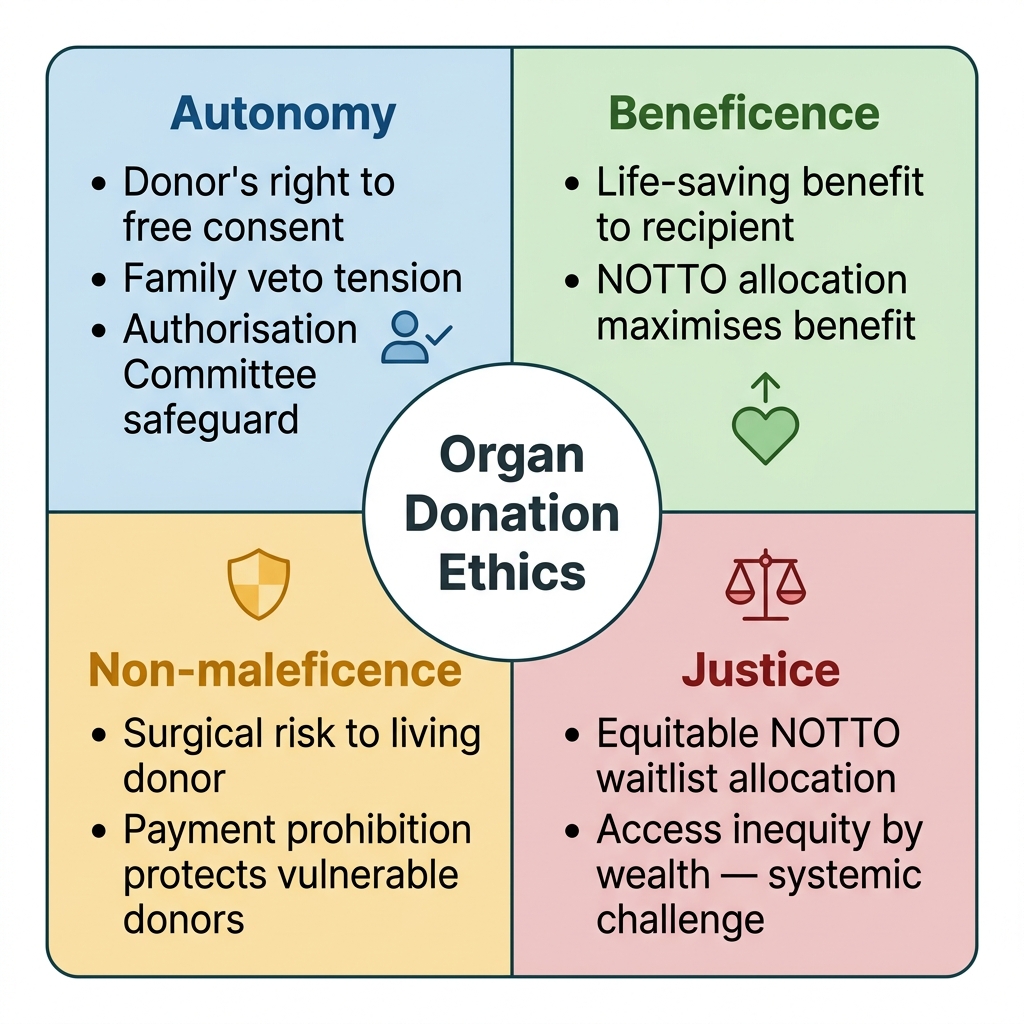
Beauchamp & Childress's Four Principles Applied to Organ Donation Ethics
- Opt-in vs opt-out: India uses opt-in (explicit family consent); no presumed consent
- Payment for organs: prohibited under THOTA; only Iran has a legal compensated living-donor system
- Allocation: NOTTO system prioritises by compatibility + urgency + waiting time — designed for justice
- Non-relative donation requires Authorisation Committee oversight to protect donor autonomy
KEY TAKEAWAYS
The Transplantation of Human Organs and Tissues Act 1994 (THOTA), amended in 2011, is the legal framework governing all organ and tissue transplantation in India. The original Act legalised brain-death-based deceased donor transplantation, established the four-doctor board for brain death certification, limited living donation to near relatives, and criminalised commercial trading. The 2011 amendment expanded the near-relative definition to include grandparents/grandchildren, introduced NOTP and NOTTO for national coordination of deceased donor allocation, permitted swap transplantation for ABO-incompatible near-relative pairs, and extended the Act to include tissues. Living donation requires free, voluntary, informed consent; non-relative donation requires Authorisation Committee approval. India operates an opt-in consent system — family consent is required even if the deceased registered as a donor. The core ethical principles governing transplantation are: autonomy (voluntary consent, free from coercion), justice (equitable allocation via NOTTO), beneficence (maximum benefit to recipients), and non-maleficence (donor protection; commercial prohibition). The tension between increasing organ supply and protecting donors from exploitation remains the central ethical challenge in Indian transplantation medicine.
REFLECT
You are the registrar in an ICU. A 28-year-old motorcyclist has been declared brain-dead after a road traffic accident. The brain-death certification has been completed by the four-doctor board. The patient's parents arrive and the transplant coordinator asks for consent to donate his organs. His parents say: 'He told us he wanted to donate his organs — he even registered online.' However, his maternal grandmother (who is present) objects strongly on religious grounds, stating that the body must remain intact for burial. Consider the following: Under THOTA, what is the legal requirement for consent — is the grandmother's veto legally binding? What ethical principles are in conflict here? How would you, as the treating doctor, approach the family in this situation? If the parents consent over the grandmother's objection, is this valid? What are the limits of the transplant team's legal authority? Write a reflective account of how you would navigate this situation.