Page 5 of 20
FM6.2,FM14.11 | Firearm & Blast Wound Ballistics — SDL Guide
Learning Objectives
- Explain the biomechanical basis of firearm wound production — temporary cavity, permanent cavity, fragmentation
- Classify entrance wounds by range (contact, near-contact, close, intermediate, distant) and describe the distinguishing features of each
- Describe and differentiate exit wounds from entrance wounds and explain atypical presentations
- Classify blast injuries into primary, secondary, tertiary, and quaternary mechanisms with characteristic injury patterns
- Outline the systematic clinical examination and documentation protocol for gunshot wounds
- Describe the collection, preservation, and dispatch of trace evidence including GSR
- Formulate a medico-legal opinion on range of fire, direction, and manner of death from wound evidence
INSTRUCTIONS
The ability to examine a gunshot or blast wound and translate physical findings into a reliable medico-legal opinion is one of the most consequential forensic skills a physician can possess. In homicide investigations, your opinion on whether a wound is a contact shot or a distant shot — a suicide shot or a homicide shot — can determine whether a person is charged with murder. In disaster response, understanding blast injury classification determines triage priorities. This module builds the analytical framework for both: systematic wound examination leading to range estimation, entrance-exit differentiation, and blast injury classification, grounded in the biomechanics of how bullets and pressure waves cause tissue damage.
References
- KSN Reddy — Essentials of Forensic Medicine & Toxicology (textbook)
- BV Subrahmanyam — Modi's Medical Jurisprudence and Toxicology (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 28-year-old woman is found dead in her home. The scene shows a single gunshot wound to the right side of the head. The police ask: was this suicide or homicide? You examine the wound: it is 10 mm in diameter, circular, with a distinct abrasion collar, charred and everted skin margins, a zone of soot blackening extending 2 cm around the wound, and the hair is singed. There is no exit wound. The bullet is recovered from the left parietal region. Answer these questions and you solve the case: What is the range of fire? Which direction did the bullet travel? Is the wound consistent with a self-inflicted shot? The answers are all in the wound — if you know how to read it.
WHY THIS MATTERS
Gunshot wound analysis is one of the most heavily litigated areas of forensic medicine in India. Defence counsel regularly challenges the forensic physician's opinion on range of fire, because the same wound could support 'fired during a struggle at close range' (possibly accidental or self-defence) versus 'fired from distance while the victim was stationary' (premeditated murder). The distinction rests on precise examination findings. Blast injuries have acquired additional significance in the context of explosive device investigations — forensic physicians at disaster sites must distinguish primary blast lung from other injuries to guide both immediate triage and subsequent investigation. Competency FM6.2 directly underpins the court-credible opinion on suicide vs homicide, and FM14.11 (bullet/cartridge interpretation) is tested in post-graduate entrance examinations. Getting range estimation wrong is not just an academic error — it can send an innocent person to prison or allow a murderer to walk free.
RECALL
From FM6.1 (previous module):
• Range = distance between muzzle and target at time of firing
• Propellant residue: black powder deposits heavy soot; smokeless powder produces GSR particles (lead+barium+antimony by SEM-EDX)
• Rifled vs smooth-bore: rifled weapons produce entrance wounds with a single bullet; smooth-bore (shotguns) produce pellet patterns
• Caliber and muzzle velocity: high-velocity rifle rounds versus lower-velocity pistol rounds differ in tissue destruction
From Year-1 pathology and anatomy:
• Wound types: abrasion (epidermis), contusion (haemorrhage), laceration (blunt tearing), incised wound (sharp edges)
• Skin anatomy: epidermis over dermis; the dermis's collagen produces the abrasion collar (Fisch ring) around an entrance wound
• Organ vulnerability: lung > spleen > liver > kidney in blast tolerance (blast lung is the primary visceral target)
Wound Ballistics: How a Bullet Causes Tissue Damage
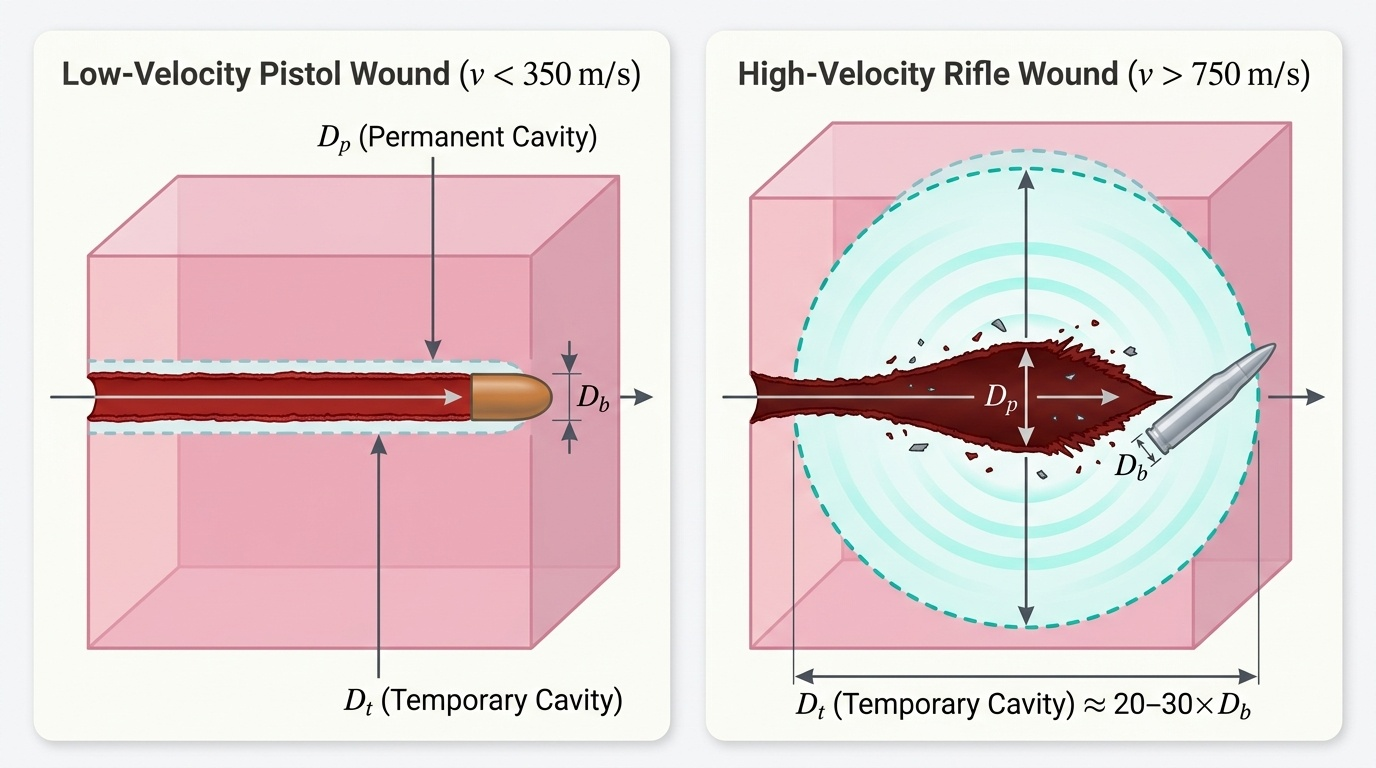
Wound ballistics is the science of what happens to a bullet after it enters the body — how it transfers kinetic energy, what it disrupts, and why the resulting wound has the characteristics it does. Without understanding wound ballistics, range estimation and wound interpretation are guesswork rather than science. The key concept is kinetic energy transfer: a bullet does damage in proportion to the energy it deposits in tissue (KE = ½mv²). A high-velocity rifle bullet travelling at 900 m/s carries four times the kinetic energy of the same bullet travelling at 450 m/s — and wounds accordingly.
When a bullet enters tissue, it creates two cavities. The permanent cavity is the actual tissue that is crushed, lacerated, and destroyed along the bullet track — the physical hole. This is determined primarily by bullet diameter and the extent of bullet deformation (a hollow-point expands and creates a larger permanent cavity). The temporary cavity is a transient radial displacement of tissue caused by the supersonic pressure wave ahead of the bullet — tissue is pushed outward momentarily, then springs back. In low-velocity pistol wounds (<350 m/s), the temporary cavity is small and clinically insignificant in elastic tissues like muscle. In high-velocity rifle wounds (>750 m/s), the temporary cavity can be 20–30 times the bullet diameter and causes severe disruption of inelastic tissues (liver, spleen, brain) even beyond the permanent track.
Yaw and tumbling are secondary ballistic phenomena. Yaw is the sideways tilt of the bullet off its long axis; tumbling is rotation around the bullet's midpoint. These increase the bullet's effective cross-section in tissue, enlarging the permanent cavity and depositing more energy. A bullet that yaws 90° (travels sideways) deposits nearly all its energy and typically produces no exit wound.
Fragmentation — the bullet breaking into multiple pieces — multiplies wound tracks in tissue and greatly increases tissue destruction. Hollow-point and soft-point bullets are designed to fragment or deform. Military FMJ bullets are less prone to fragmentation but yaw at greater depths in tissue, explaining the 'dumdum wound' effect seen in some rifle wounds despite FMJ design.
For the forensic physician, the practical lesson is: a large internal injury out of proportion to the small entrance wound indicates a high-velocity weapon or an expanding/fragmenting bullet — this finding is itself medico-legally significant in determining weapon class and, therefore, intent.
Provided image
Entrance Wounds: Range Classification and Features
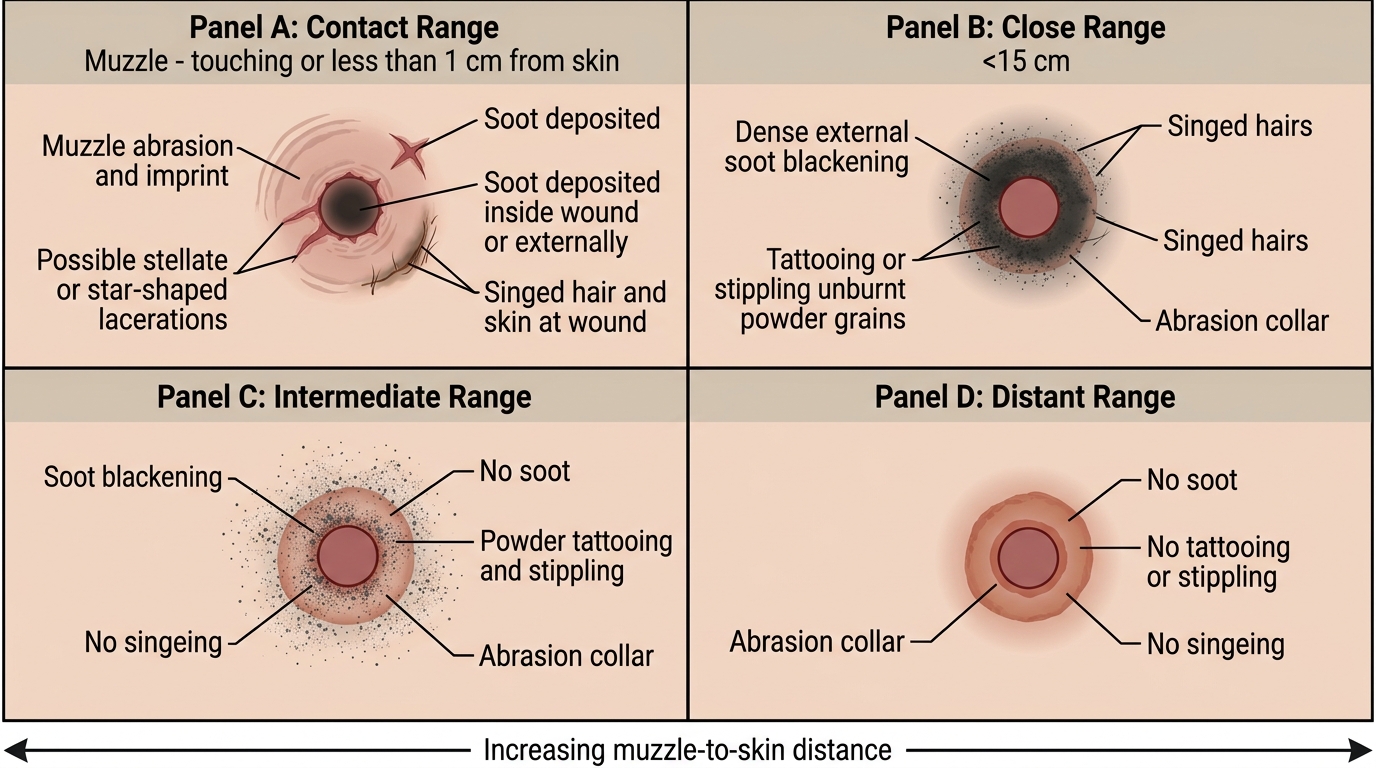
Range estimation is the central forensic task in gunshot wound analysis, and it is performed by examining the entrance wound for the products of combustion that are deposited at varying distances from the muzzle. The key diagnostic features — blackening (sooting), fouling, tattooing (stippling), singeing, and the abrasion collar (Fisch ring) — each have a different deposition radius, and their presence or absence defines the range category. The classification below follows Reddy's reference values, which should be treated as approximate ranges dependent on the specific weapon and cartridge.
Contact wound (muzzle pressed against or within 1 cm of skin): The entire discharge products enter beneath the skin. The wound shows heavy blackening on the deep aspect of the wound margins and underlying subcutaneous tissue (not the external skin surface), because all soot and gases pass through the wound. In hard contact wounds (muzzle pressed firmly against skin over bone, such as the skull), the rapid entry of gas with no escape causes the gas to tear the skin in a star-shaped (cruciform) laceration. There may be a muzzle imprint/abrasion around the wound from the weapon pressing against the skin during recoil. The barrel itself may show soot blowback. The wound may appear deceptively small externally; internal examination reveals heavy sooting of the wound track.
Near-contact wound (1–2 cm): Heavy blackening visible on the external wound surface, tattooing of the surrounding skin, possible singeing.
Close range (up to approximately 15 cm, per Reddy's): Blackening of the skin surface plus tattooing (mechanical embedding of unburned and partially burned powder particles in the skin that cannot be wiped away) plus possible singeing of hair. The abrasion collar is present in all rifled-weapon entrance wounds regardless of range.
Intermediate range (approximately 15–60 cm per Reddy's): Tattooing (stippling) is present without blackening. Blackening requires proximity because soot particles are large and settle quickly; tattooing particles are smaller and travel further. Singeing may be absent. The abrasion collar remains present.
Distant range (beyond approximately 60 cm per Reddy's): Only the abrasion collar (Fisch ring) remains — no blackening, no tattooing, no singeing. The wound is a clean, punched-out hole with the narrow ring of abrasion around its margin caused by skin being dragged forward by the bullet and then scraped by its rotating surface.
Firearm Entrance Wounds by Range
| Range | Distance (approx.) | Blackening | Tattooing | Singeing | Abrasion Collar |
|---|---|---|---|---|---|
| Contact | <1 cm | Internal surface only (or star laceration) | Absent externally | Present | Present |
| Near-contact | 1–2 cm | External surface, heavy | Present | Present | Present |
| Close | <15 cm | External surface | Present | May be present | Present |
| Intermediate | 15–60 cm | Absent | Present (unwiped) | Absent | Present |
| Distant | >60 cm | Absent | Absent | Absent | Present only |
Important caveats: These distances are approximate and vary with the specific weapon, barrel length, type and load of propellant, and atmospheric conditions. Always qualify range estimates in reports. Intermediate ranges can shift by a factor of 2–3 depending on the weapon. The forensic physician must arrange test firings with a similar weapon and ammunition if a precise range opinion is required for court.
SELF-CHECK
A 40-year-old man is found dead with a gunshot wound to the right temple. Examination reveals: a circular 9 mm wound, abrasion collar present, no external blackening, no tattooing, no singeing. What range category is indicated, and what is the key evidence?
A. Contact range — the abrasion collar and absence of blackening are characteristic of a hard contact wound
B. Close range (<15 cm) — the abrasion collar with tattooing indicates close-range firing
C. Distant range (>60 cm) — abrasion collar only, without blackening or tattooing, indicates distant range
D. Intermediate range (15–60 cm) — tattooing without blackening is the hallmark
Reveal Answer
Answer: C. Distant range (>60 cm) — abrasion collar only, without blackening or tattooing, indicates distant range
The absence of blackening, tattooing, and singeing, with only the abrasion collar present, indicates distant range firing (>60 cm per Reddy's classification). At distant range, all combustion products have dispersed before reaching the target — only the mechanical action of the bullet's rotation on the skin margin produces the abrasion collar (Fisch ring). This range finding is significant for manner-of-death determination: a distant-range wound to the temple cannot be self-inflicted (the victim cannot hold a weapon >60 cm from their own head) and is strong evidence of homicide.
Exit Wounds and Atypical Wound Patterns
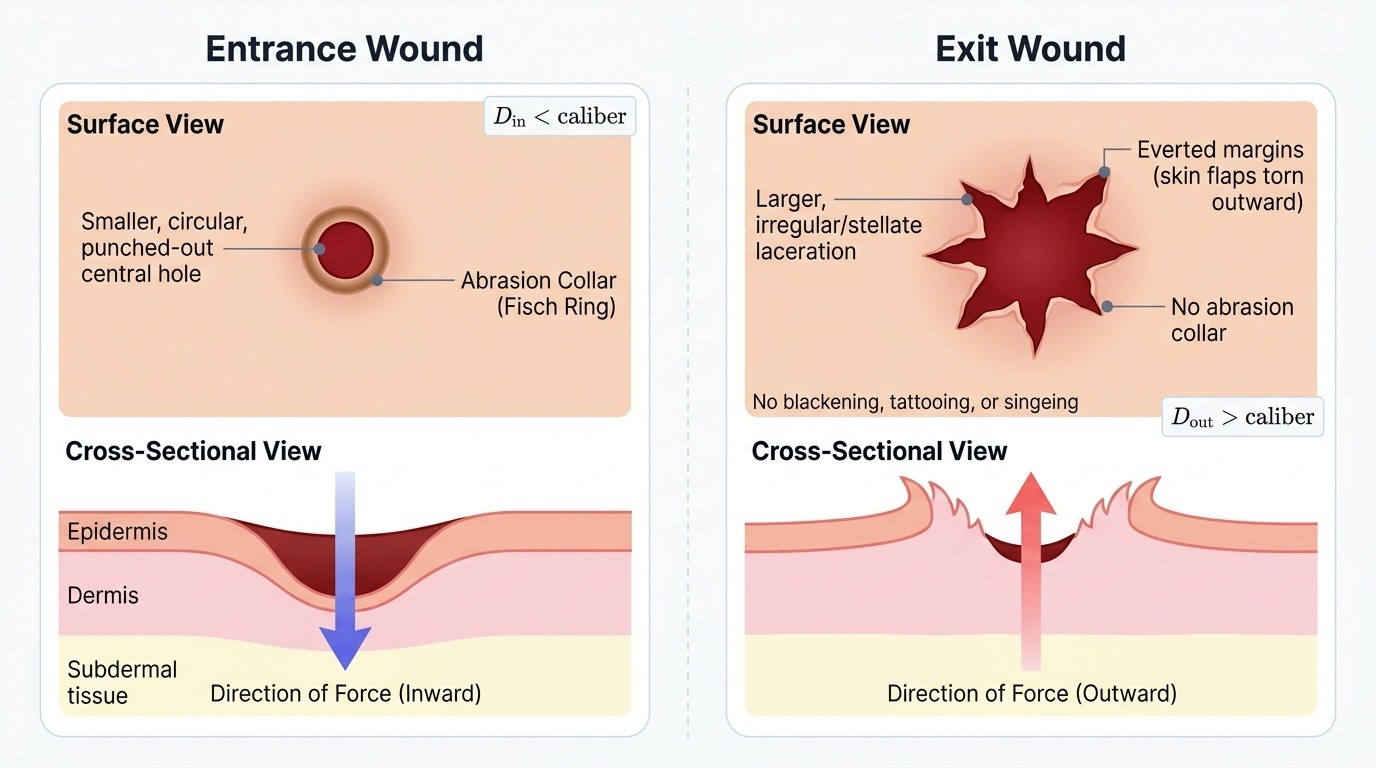
When a bullet retains sufficient energy to pass entirely through the body, it produces an exit wound. Distinguishing entrance from exit wounds is one of the most critical and most frequently contested forensic determinations — an error here can reverse the reconstruction of a shooting completely. The fundamental differences arise from the direction of force: at entrance, the bullet is entering tissue, compressing skin inward and producing a neat punch-out; at exit, the bullet is pushing outward, tearing the skin from inside and producing an irregular everted tear with no combustion products.
The typical entrance wound is smaller than the bullet caliber (skin recoils), circular or oval (depending on angle of incidence), punched-out with slightly inverted margins, and surrounded by an abrasion collar (Fisch ring) — a narrow ring of dried, brownish abrasion caused by the bullet's rotating surface stretching and abrading the epidermis as it enters. There are no abrasion collar equivalents at the exit.
The typical exit wound is larger than the entrance wound (because the bullet may have deformed, yawed, or pushed tissue ahead of it), irregular in shape with everted (outward-pointing) margins, has no abrasion collar, and shows no blackening, tattooing, or singeing (because exit wounds are the downstream end of the wound track, distant from the weapon discharge). Exit wounds may be stellate, slit-like, or grossly irregular depending on bullet deformation and tissue type.
Provided image
Atypical wound patterns are high-yield examination topics:
- Supported exit wound (shored exit): when the skin at the exit site is pressed against a firm surface (belt, floor, clothing seam) at the moment of bullet exit, the support prevents the skin from everting freely. The result is an exit wound that is smaller than expected and has an irregular abrasion collar from the supporting surface — it can closely mimic an entrance wound. Recognition requires scene information (position of body, what the exit side contacted).
- Tangential (graze) wound: bullet passes along the skin surface, producing an elongated trough with a leading edge (irregular, abraded) and a trailing edge (undermined); no complete perforation; useful for inferring direction of travel.
- Ricochet wound: bullet that has struck an intermediate surface before reaching the body has lost velocity, may be deformed or tumbling — the wound is irregular, larger than expected for the caliber, and may have the bullet at an oblique angle in tissue.
- Re-entry wound: bullet exits the body and re-enters (e.g., passing through an arm into the trunk) — two entrance wounds and either two exits or a bullet in the body; the sequence must be inferred from wound track directions.
| Feature | Typical Entrance | Typical Exit |
|---|---|---|
| Size | Smaller (skin recoil) | Larger |
| Shape | Circular/oval, punched-out | Irregular, slit-like, stellate |
| Margins | Inverted | Everted |
| Abrasion collar | Present | Absent |
| Blackening/tattooing | Present (range-dependent) | Absent |
| Soiling | From propellant/GSR | Absent |