Page 4 of 15
FM4.2-3,FM14.4 | Age & Dental Identification & Age Estimation — SDL Guide
Learning Objectives
- Describe deciduous and permanent dental eruption patterns and their role in age estimation
- Apply Gustafson's method (6 criteria) for adult age estimation from teeth with correct scoring and regression formula
- Identify key epiphyseal fusion sites and their forensic significance for age determination, using Indian reference values
- Document bite marks and apply dental record matching principles for identification
- Prepare a medicolegal age estimation report that meets legal standards (Juvenile Justice Act 2015, POCSO 2012)
INSTRUCTIONS
Age estimation is among the most legally consequential skills in forensic medicine. The difference between a subject being 17 years and 11 months versus 18 years and 1 month can determine whether a case proceeds before a Juvenile Justice Board or a regular criminal court — with dramatically different consequences for the accused. Similarly, whether a victim is below or above 18 years shapes the charges framed under POCSO. The forensic doctor is asked to perform this assessment without documentary evidence, using only biological markers. This module provides the scientific framework and practical skills for that assessment, integrating dental and skeletal methods with the procedural requirements of FM14.4.
References
- KSN Reddy — Essentials of Forensic Medicine & Toxicology, Ch 4 (textbook)
- BV Subrahmanyam — Modi's Medical Jurisprudence and Toxicology, Ch 3 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 17-year-old boy is arrested in connection with a robbery in which a guard was killed. The defence lawyer argues the accused is a juvenile (under 18) and should be tried by the Juvenile Justice Board rather than a sessions court — a claim that, if accepted, would dramatically reduce the possible sentence. No birth certificate exists. The court issues a requisition for medical age determination. You are the forensic officer on call. You have the boy in front of you, a consent form, and a request for an X-ray of his wrist and clavicle. What you write in the next two hours will shape the trajectory of this case — and this person's life.
WHY THIS MATTERS
Age estimation is demanded in three major categories of Indian forensic practice. First, criminal cases involving juveniles under the Juvenile Justice (Care and Protection of Children) Act 2015 — where the 18-year threshold determines criminal versus juvenile jurisdiction. Second, sexual assault cases under POCSO Act 2012 — where the victim's age below 18 years is an essential element of the offence and aggravated provisions. Third, civil matters including disputed marriage age, employment age, insurance claims, and missing person identification. In each category, the forensic doctor provides the only objective biological evidence of age when documentary records are absent, fraudulent, or contested. This skill is therefore practised not only in medical colleges but in government hospitals, district courts, and JJ boards across India.
RECALL
Recall from Year-1 Anatomy: the dental formula for adult humans is I 2/2, C 1/1, P 2/2, M 3/3 (32 teeth total). Deciduous teeth have no premolars and only 2 molars per quadrant. Epiphyseal plates (growth plates) are cartilaginous zones at the ends of long bones that ossify with age; their appearance on X-ray as a radio-dense line marks active growth, and their fusion marks the end of longitudinal bone growth. Secondary sexual characteristics (pubic hair, breast development, voice change) develop from puberty onward. These biological facts are the raw material from which age estimates are derived.
The Medicolegal Context: Why Age Matters
The legal and professional stakes of age estimation make it a skill that demands both scientific precision and professional restraint. Age estimation is sought formally by magistrates and police officers when documentary evidence (birth certificates, school records) is absent, suspected to be fraudulent, or inconsistent with appearance. The requesting authority is almost always seeking a binary answer — is this person above or below a legal threshold? — but the forensic doctor's scientific obligation is to provide a range, not a binary, and to acknowledge uncertainty explicitly.
Three legislative frameworks create the primary demand for age estimation in India. The Juvenile Justice (Care and Protection of Children) Act 2015 mandates that when the age of a person in conflict with the law is disputed and documents are unavailable, medical examination must be ordered. A person found to be below 18 years is tried by the Juvenile Justice Board with a maximum consequence of 3 years in a reform facility; a person found to be above 18 is tried in regular court with adult sentencing. The POCSO Act 2012 establishes 18 years as the age of consent for sexual activity; a victim below 18 triggers aggravated offence provisions. The Indian Contract Act 1872 and Hindu Marriage Act 1955 set minimum ages for contract capacity and marriage respectively — both contested in civil courts when birth documents are fraudulent.
The forensic doctor must understand the legal consequence of the age range reported. If the estimated range straddles the legal threshold (e.g., 16–20 years), the report must state this explicitly and note that the threshold cannot be excluded — it is for the court, not the doctor, to make the final legal determination. A doctor who reports a single age without uncertainty, in order to give the court a 'clean answer,' is providing a false sense of precision and exposing themselves to professional and legal challenge.
Formally, Juvenile Justice Board procedures require radiological evidence (X-ray of wrist, clavicle, and pelvis) supplemented by dental examination. The examining doctor must produce a written report that can be placed before the Board, and may be summoned to give oral evidence.
Governing Principles of Age Estimation
Age estimation in forensic medicine rests on two categories of biological markers: developmental markers (features that appear or change with growth — erupting teeth, appearing ossification centres, developing secondary sexual characteristics) and degenerative markers (features that change with ageing — Gustafson's dental changes, skull suture closure, pubic symphysis degeneration). Developmental markers are more reliable and precise in children and young adults; degenerative markers take over in adults above 25–30 years where development is complete.
The most fundamental governing principle is that biological age does not equal chronological age. A malnourished child may show skeletal development consistent with an age 2–3 years younger than their actual birth date. An obese child may show advanced bone age. Chronic illness, endocrine disorders (hypothyroidism, growth hormone deficiency, precocious puberty), and genetic conditions all shift the relationship between biological and chronological age. The forensic doctor's report gives an estimated age range based on biological markers; it is a statement about biological development, not a certificate of birth date.
A critical methodological rule for Indian practice: always use Indian population reference tables for both dental eruption and epiphyseal fusion data. Western atlases (Greulich-Pyle for bone age, Anderson and Popovich for dental age) were derived from North American and European populations that differ in both timing and variability from South Asian populations. Reddy's Essentials of Forensic Medicine provides Indian population-based reference data that is the standard of care in Indian forensic practice. Using Greulich-Pyle without adjustment in an Indian examination is a methodological error that could be challenged in court.
The output of any age estimation must be a range (e.g., '18–22 years') with a stated confidence level, not a single point estimate. The width of the range reflects the precision of the available biological markers: dental methods in adults carry ±3.6 years (Gustafson's), radiological epiphyseal fusion can achieve ±1–2 years at key sites in adolescents, but degenerative markers in adults over 40 may yield ranges of ±5–10 years.
Dental Eruption Patterns and Their Forensic Use
The deciduous (primary) dentition consists of 20 teeth (5 per quadrant: 2 incisors, 1 canine, 2 molars) and erupts between 6 months and 2.5 years of age. Eruption begins with the mandibular central incisors (~6 months) and ends with the second deciduous molars (~24–30 months). The deciduous dentition is complete by about 2.5 years of age and provides a reliable age indicator in infants and toddlers where dental eruption follows a predictable sequence with relatively low individual variation.
The permanent dentition consists of 32 teeth (8 per quadrant: 2 incisors, 1 canine, 2 premolars, 3 molars) and begins erupting around 6 years of age. The sequence and approximate ages for the Indian population are:
| Tooth | Mandible (lower) | Maxilla (upper) |
|---|---|---|
| Central incisor (I1) | 6–7 yr | 7–8 yr |
| Lateral incisor (I2) | 7–8 yr | 8–9 yr |
| Canine (C) | 9–10 yr | 11–12 yr |
| First premolar (P1) | 10–12 yr | 10–11 yr |
| Second premolar (P2) | 11–12 yr | 10–12 yr |
| First molar (M1) | 6–7 yr | 6–7 yr |
| Second molar (M2) | 12–13 yr | 12–13 yr |
| Third molar (M3/wisdom) | 17–21 yr | 17–21 yr |
In forensic practice, dental eruption is most useful for age estimation between 6 and 21 years — the range spanning the first permanent molar eruption to wisdom tooth completion. Below 6 years, deciduous eruption provides reliable staging. Above 21 years, all permanent teeth are present (or absent due to decay/extraction) and eruption patterns are no longer useful; Gustafson's degenerative method takes over for adults.
Forensic limitations: eruption timing is influenced by race (South Asian populations may erupt slightly earlier), nutrition, fluoride exposure, and dental disease. Missing teeth due to extraction must be differentiated from unerupted teeth; X-ray is essential for unerupted teeth. Wisdom tooth (third molar) eruption has the widest age range (17–21 years) and the greatest inter-individual variability, making it the least precise dental age indicator, but its forensic significance is high precisely because its eruption straddles the legally critical 18-year threshold.
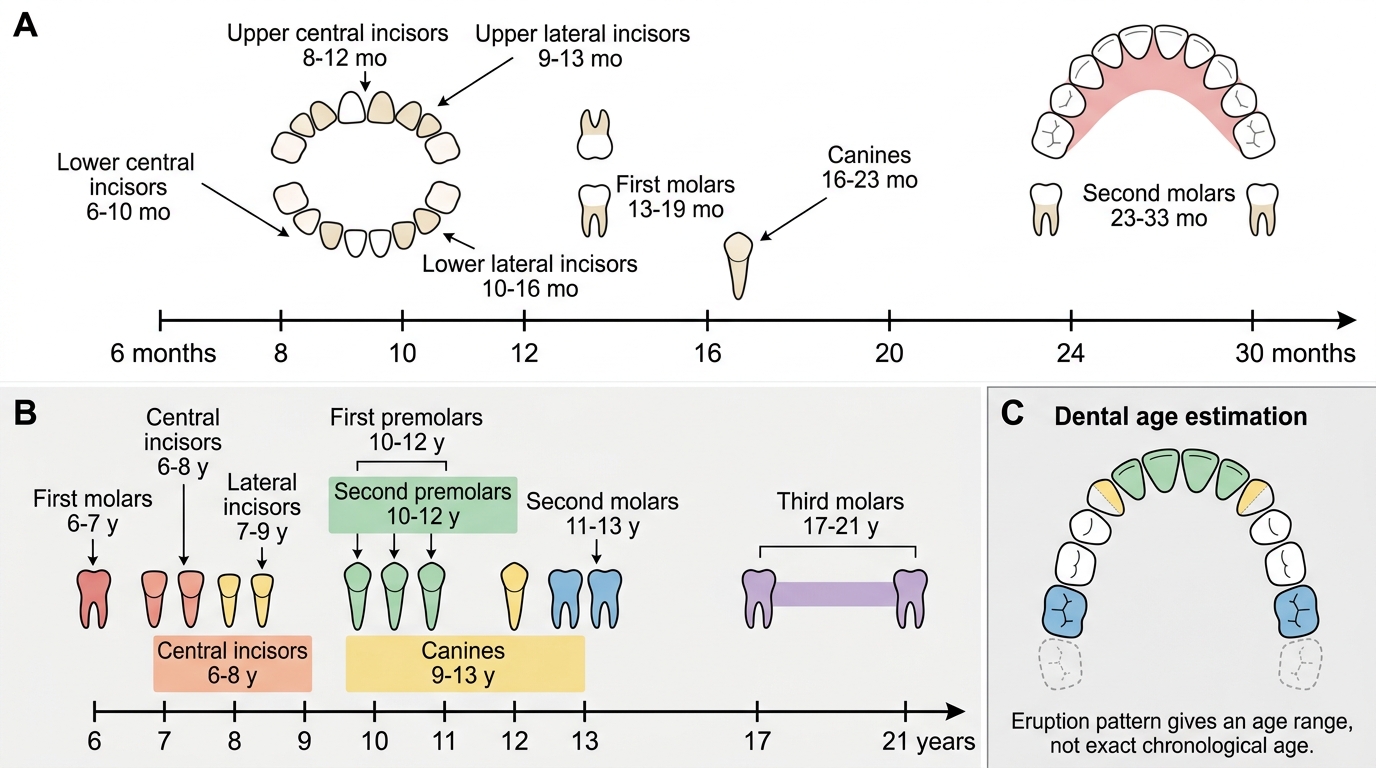
Dental Eruption Timeline for Age Estimation
SELF-CHECK
A 14-year-old boy presents for dental examination. His mandibular first molars are fully erupted, central and lateral incisors are permanent, canines are erupting, and third molars are not yet visible clinically or on X-ray. Which statement about dental age estimation is MOST accurate?
A. The absence of third molars confirms the boy is under 17 years
B. The pattern of eruption is consistent with an age of approximately 11–14 years
C. Dental eruption alone can confirm the exact chronological age
D. Third molars must be fully erupted before any age estimate can be made
Reveal Answer
Answer: B. The pattern of eruption is consistent with an age of approximately 11–14 years
The pattern described — erupted permanent incisors and first molars, erupting canines, no third molar visible — is consistent with approximately 9–14 years. The absence of third molars (wisdom teeth) indicates age is likely below 17, but cannot confirm exact age as third molars may be absent due to agenesis. Dental eruption gives a range, not an exact age. The other options are either too definitive or incorrect.