Page 5 of 9
FM14.{7,19} | Forensic Lab Skills: Blood Grouping & DNA Exhibits — SDL Guide
Learning Objectives
- Demonstrate the correct technique to perform ABO and Rh-D blood grouping on a fresh blood specimen (FM14.7)
- Interpret agglutination results using the forward-grouping and reverse-grouping format and assign the correct ABO and Rh-D blood group
- Describe the principles of blood group determination from forensic stains using mixed agglutination and absorption-elution methods
- Collect, preserve, seal, and dispatch specimens for DNA fingerprinting using multiple laboratory formats — fresh blood (EDTA), buccal swab, FTA card, semen/saliva swab, tooth, and bone (FM14.19)
- Complete chain-of-custody documentation for DNA exhibits and ensure proper dispatch to the forensic laboratory
INSTRUCTIONS
Two of the most practically important forensic laboratory skills for a medical student are blood grouping and DNA exhibit collection. Blood grouping from a stain can link a suspect to a crime scene or exclude an accused from paternity. DNA profiling from a properly collected and preserved exhibit can individualise evidence with a discriminating power of one in several billion. Both skills depend on correct technique — a laboratory result from an improperly collected or preserved sample may be unusable, and an exhibit whose chain of custody is broken may be inadmissible. This module develops both competencies through a structured understanding of the underlying science, the technical procedure, and the documentation requirements.
References
- KSN Reddy — Essentials of Forensic Medicine & Toxicology (textbook)
- BV Subrahmanyam — Modi's Medical Jurisprudence and Toxicology (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Scene 1: A bloodstain is found on a knife recovered from the scene of a stabbing. The victim's blood group is A-positive. The suspect claims the blood is theirs (they cut themselves accidentally). Crime scene blood grouping will test this claim — if the stain is Group B, neither the victim nor the suspect is the source, and the investigation expands. If it is Group A, it is consistent with the victim but does not exclude the suspect if they are also Group A. Scene 2: A disputed paternity case — the child, the alleged father, and the mother each provide blood samples. DNA profiling will determine with near-certainty whether biological paternity exists. To reach the FSL in a usable state, both the blood group stain and the DNA exhibits must have been collected, preserved, and dispatched following the exact procedure outlined in this module.
WHY THIS MATTERS
ABO and Rh blood grouping is one of the oldest, most widely used, and most easily performed forensic biological tests. Unlike DNA profiling, which requires sophisticated laboratory equipment, blood grouping can be performed at any equipped pathology laboratory using standardised reagents. For this reason, it remains a frontline forensic test in resource-constrained settings and is routinely performed by medical officers at district level. DNA exhibit collection, meanwhile, is a technique that any physician involved in sexual assault examination, autopsy, or scene investigation may be required to perform — and doing it correctly the first time is critical, because a degraded or contaminated exhibit yields unusable results that cannot be recovered. These are genuinely practical skills with direct patient and justice impact.
RECALL
Consolidate the prior knowledge that underpins this module:
- From Physiology (Year 1): The ABO blood group system — antigens on red blood cell (RBC) surfaces, antibodies in serum, the concept of agglutination (clumping of RBCs when antigen meets complementary antibody). The Rh system — the D antigen as the clinically most significant Rh antigen, Rh-positive vs Rh-negative.
- From lab1-specimens (this cluster): Blood preservation for DNA analysis uses EDTA (not NaF/oxalate, which is for chemical/alcohol analysis) — the preservative choice depends on the downstream analytical purpose.
- From lab3-advances: STR profiling is the standard DNA profiling method — it requires nuclear DNA from nucleated cells. Fresh blood, saliva, semen, and tissue are good sources; dried blood on an FTA card and tooth pulp yield viable DNA even after transport or long storage.
- From lab2-professionalism: Chain-of-custody documentation principles — exhibit labelling, wax sealing, and signature logs that apply equally to DNA exhibits.
Legal and Professional Context of Forensic Lab Skills
Blood grouping and DNA exhibit collection arise in a specific and well-defined set of medicolegal contexts. Understanding the legal purpose of each examination determines the choice of technique, the standard of documentation required, and the professional obligations of the performing clinician.
Provided image
ABO and Rh blood grouping in forensic contexts:
Blood group determination from stains or biological samples is performed in three principal medicolegal settings:
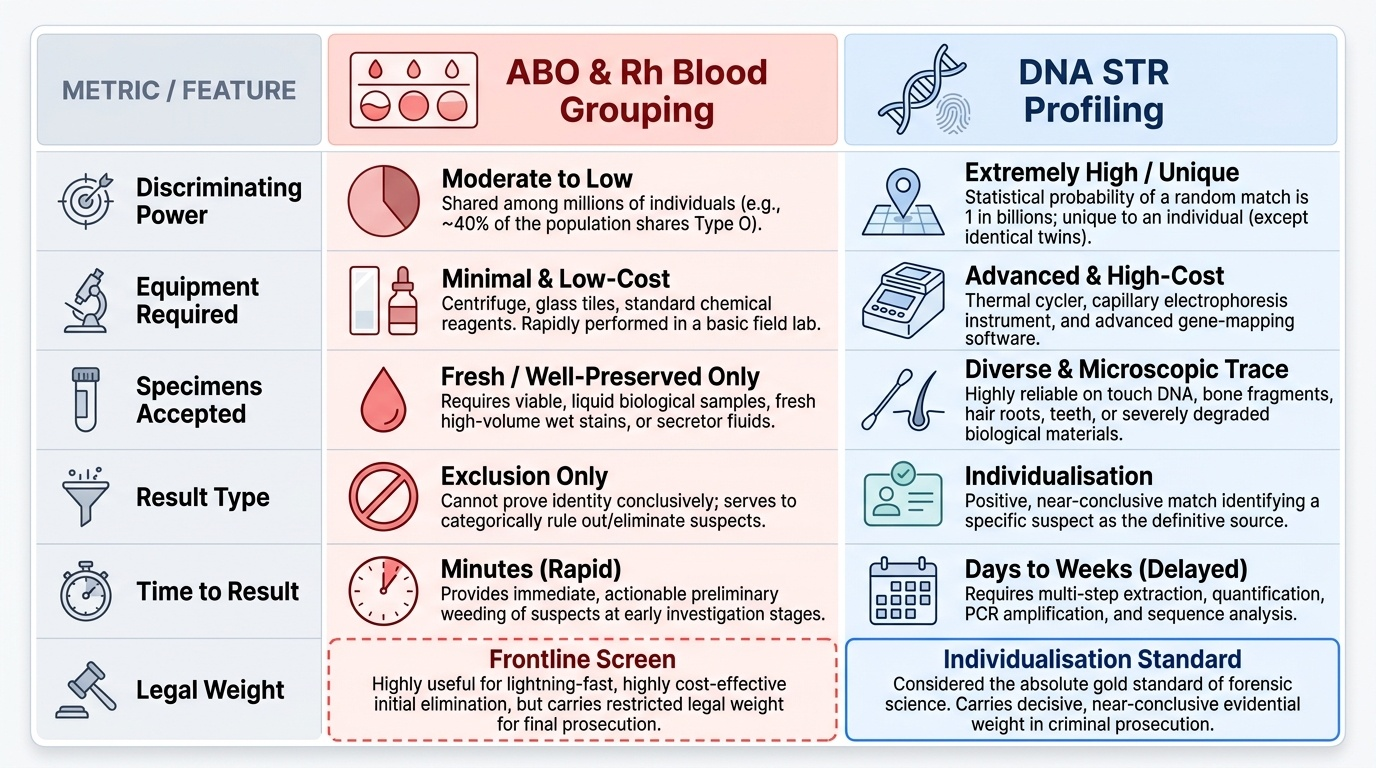
• Crime scene investigation: Blood, semen, or saliva stains at the scene may be typed to include or exclude individuals as potential sources. Blood grouping of a scene stain does not individualise — it cannot tell you whose blood it is, only whose it is not (exclusion) or that it is consistent with a known individual. This distinction matters legally: inclusion via blood grouping is probabilistic (the suspect cannot be excluded), whereas inclusion via DNA profiling is near-conclusive.
• Sexual assault investigation: Semen grouping (using ABO secretor typing) in sexual assault cases can exclude the accused if his blood group is different from the secretor type detected in the semen.
• Paternity and kinship disputes: Before DNA profiling became routine, blood grouping was the primary biological method for paternity exclusion. It cannot prove paternity but can exclude an alleged father with certainty if he lacks the genetic markers that the child must have inherited. Today, DNA profiling is standard, but blood grouping may still be used as a preliminary screen or in resource-limited settings.
DNA exhibit collection in forensic contexts:
FM14.19 requires competence in collecting, preserving, sealing, and dispatching exhibits specifically for DNA fingerprinting. This arises in:
• Sexual assault examinations — vaginal, anal, and oral swabs; penile swabs from the accused
• Homicide and assault — blood, hair roots, skin under fingernails, saliva on bite marks
• Unidentified body identification — tooth pulp, bone marrow, blood from the body, and reference DNA from family members
• Disputed biological relationships — blood samples from all parties with documented informed consent
In all these contexts, the forensic medical officer performing specimen collection is creating a legal exhibit. The professional obligation is the same as for any medicolegal exhibit: the technique must be technically correct and the documentation must support admissibility.
Governing Principles: ABO and Rh Blood Group Systems
The ABO blood group system is governed by Landsteiner's Law, formulated by Karl Landsteiner in 1901, which states: if an antigen is present on an individual's red blood cells, the corresponding antibody will be absent from their serum; conversely, if the antigen is absent, the antibody will be present. This law is the logical basis for both the typing technique and the interpretation of results. There are four ABO phenotypes:
- Group A: A antigen on RBC, anti-B antibody in serum
- Group B: B antigen on RBC, anti-A antibody in serum
- Group AB: both A and B antigens on RBC, neither anti-A nor anti-B in serum (universal recipient for red cells)
- Group O: neither A nor B antigen on RBC, both anti-A AND anti-B in serum (universal donor for red cells; these individuals have the H antigen in abundance)
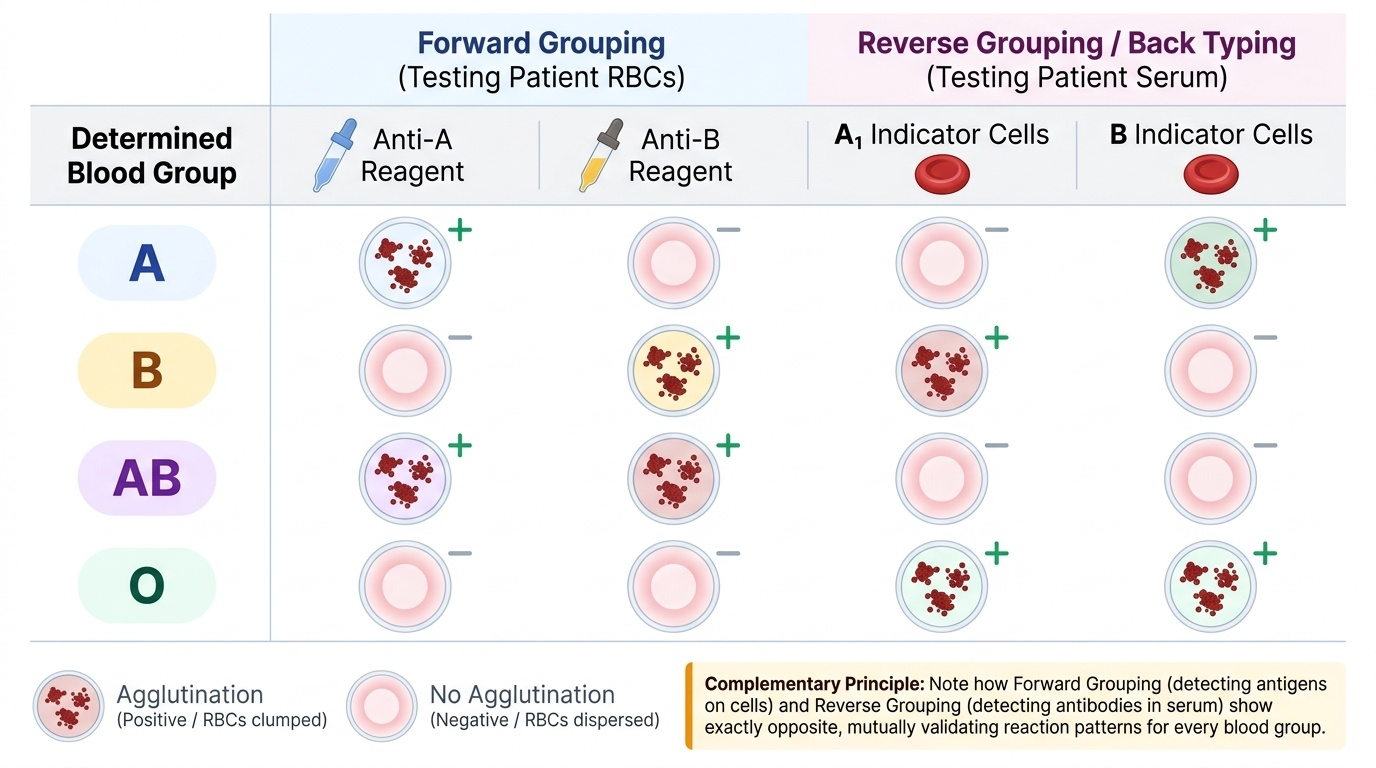
This dual prediction — that serum and cell typing must be complementary — is why blood grouping is performed using both forward grouping (testing RBCs with known antisera) and reverse grouping (also called back grouping — testing serum with known group A and B cells). The two results must be concordant; discordance indicates a technical error or a rare subgroup and must be investigated before a group is reported.
The Rh blood group system in clinical and forensic practice is primarily concerned with the D antigen (sometimes called Rh factor). D-positive individuals (Rh-positive) carry the D antigen on their RBCs; D-negative individuals lack it. Unlike ABO antibodies, anti-D does not occur naturally — it is only found in Rh-negative individuals who have been exposed to Rh-positive blood through transfusion or pregnancy. In forensic blood grouping, Rh-D typing provides an additional discriminating factor alongside ABO: approximately 85% of the Indian population is Rh-positive, so Rh-D typing alone has limited exclusion power but contributes to combined probability calculations.
Forensic blood group determination from dried stains requires modified methods because the stain contains neither intact RBCs nor viable serum — only antigens absorbed onto the substrate. Two methods are used:
• Mixed agglutination method: The stain material is scraped and added to a known typing antiserum (e.g. anti-A). If A antigen is present in the stain, the antiserum binds to it. Group A indicator cells are then added; they agglutinate around the stain particles if anti-A has bound, confirming Group A antigen. The result is read microscopically.
• Absorption-elution method (absorption-inhibition): In absorption-inhibition, the stain is incubated with a known antiserum of known titre; if antigen is present in the stain, it absorbs (reduces) the antibody, and the reduced titre is detected. In the elution variant, the absorbed antibody is then eluted off the stain by heating and detected with indicator cells. This method is more sensitive and preferred for older or smaller stains.
Provided image
| Blood Group | Anti-A + RBCs | Anti-B + RBCs | Serum + A cells | Serum + B cells |
|---|---|---|---|---|
| A | Agglutination (+) | No agglutination (−) | No agglutination (−) | Agglutination (+) |
| B | No agglutination (−) | Agglutination (+) | Agglutination (+) | No agglutination (−) |
| AB | Agglutination (+) | Agglutination (+) | No agglutination (−) | No agglutination (−) |
| O | No agglutination (−) | No agglutination (−) | Agglutination (+) | Agglutination (+) |
ABO secretor status adds a significant dimension to forensic grouping: approximately 80% of the population are ABO secretors — they secrete ABO antigens in body fluids other than blood, including saliva, semen, tears, and vaginal secretions. This means that forensic testing of semen or saliva can yield an ABO group even in the absence of blood, provided the donor is a secretor. Non-secretors (approximately 20%) produce ABO antigens on their RBCs but not in secretions — their semen or saliva cannot be ABO-typed.
SELF-CHECK
A woman of blood group B presents for a sexual assault examination. A vaginal swab reveals semen. Secretor typing shows the semen is from a Group O secretor. The accused, whose blood is Group A, argues the semen could be his. This argument is:
A. Potentially valid — blood grouping cannot definitively exclude individuals
B. Definitively excluded — a Group A secretor cannot produce Group O semen
C. Invalid — semen secretor typing is unreliable and should not be used for exclusion
D. Valid only if confirmed by ABO forward grouping of the accused's blood
Reveal Answer
Answer: B. Definitively excluded — a Group A secretor cannot produce Group O semen
The accused's blood group is A, meaning he has the A antigen on his RBCs. If he is a secretor (80% probability), his semen would contain A antigen and would type as Group A in secretor typing — not Group O. A Group A individual cannot produce Group O secretions because they carry the A antigen in their secretions. The semen from this assault typed as Group O is therefore inconsistent with a Group A secretor. This is a valid exclusion. Option A is incorrect in this context — secretor typing CAN definitively exclude a Group A individual from having left Group O secretions. Option C is incorrect; secretor typing is a validated and accepted forensic technique. Option D is incorrect — the forward grouping of the accused is additional confirmation, but the exclusion is already complete from the information given.
Method and Documentation: Blood Grouping Technique & DNA Exhibit Collection
Standard ABO and Rh-D blood grouping technique on fresh blood (FM14.7):
The tile or slide method is commonly used in forensic settings for its simplicity and speed, though tube agglutination remains the reference standard for equivocal results.
Equipment: Clean glass slide or white tile; anti-A serum (blue), anti-B serum (yellow), anti-D serum (clear/colourless); Group A indicator cells, Group B indicator cells (for reverse grouping); applicator sticks (one per reaction to prevent cross-contamination); sample blood in EDTA.
Procedure — Forward Grouping:
1. Place one drop of anti-A serum in the first section of the tile.
2. Place one drop of anti-B serum in the second section.
3. Place one drop of anti-D serum in the third section.
4. Add one small drop of the blood sample to each antiserum using a fresh applicator for each addition (do NOT use the same stick across sections).
5. Mix each section gently with the flat end of the applicator stick.
6. Rock the tile gently and observe for agglutination (clumping visible to the naked eye) within 2 minutes. In the anti-D section, agglutination visible at 1-2 minutes at room temperature indicates Rh-positive; absence of agglutination indicates Rh-negative (confirm by testing with a control).
Procedure — Reverse Grouping (mandatory accompaniment to forward grouping):
7. In a separate tube, centrifuge the blood to separate serum.
8. Add one drop of patient serum to a drop of Group A indicator cells.
9. Add one drop of patient serum to a drop of Group B indicator cells.
10. Centrifuge gently and read for agglutination.
11. Compare reverse grouping result with forward grouping — they must be concordant per Landsteiner's Law.
Documentation: Record the forward grouping result (agglutination/no agglutination for each antiserum), the reverse grouping result, the Rh-D result, and the assigned blood group with the operator's signature, date, and case/exhibit number.
DNA exhibit collection for fingerprinting (FM14.19) — multiple laboratory formats:
Fresh blood for DNA profiling is collected into an EDTA (purple/lavender) tube — not the NaF/oxalate tube used for blood alcohol. EDTA chelates calcium, inhibiting clotting, and does not interfere with DNA extraction or PCR. At least 5-10 mL of venous blood is adequate for STR profiling from an ante-mortem living subject. In a post-mortem setting, blood from the femoral vein is preferred.
FTA Card Specimen Collection for Forensic DNA Profiling
| Specimen Format | Collection Method | Preservation | Storage/Transport | Forensic Use |
|---|---|---|---|---|
| Fresh blood (EDTA) | Venous phlebotomy | EDTA tube; refrigerate | Cold chain; −20°C for long-term | Full STR profile |
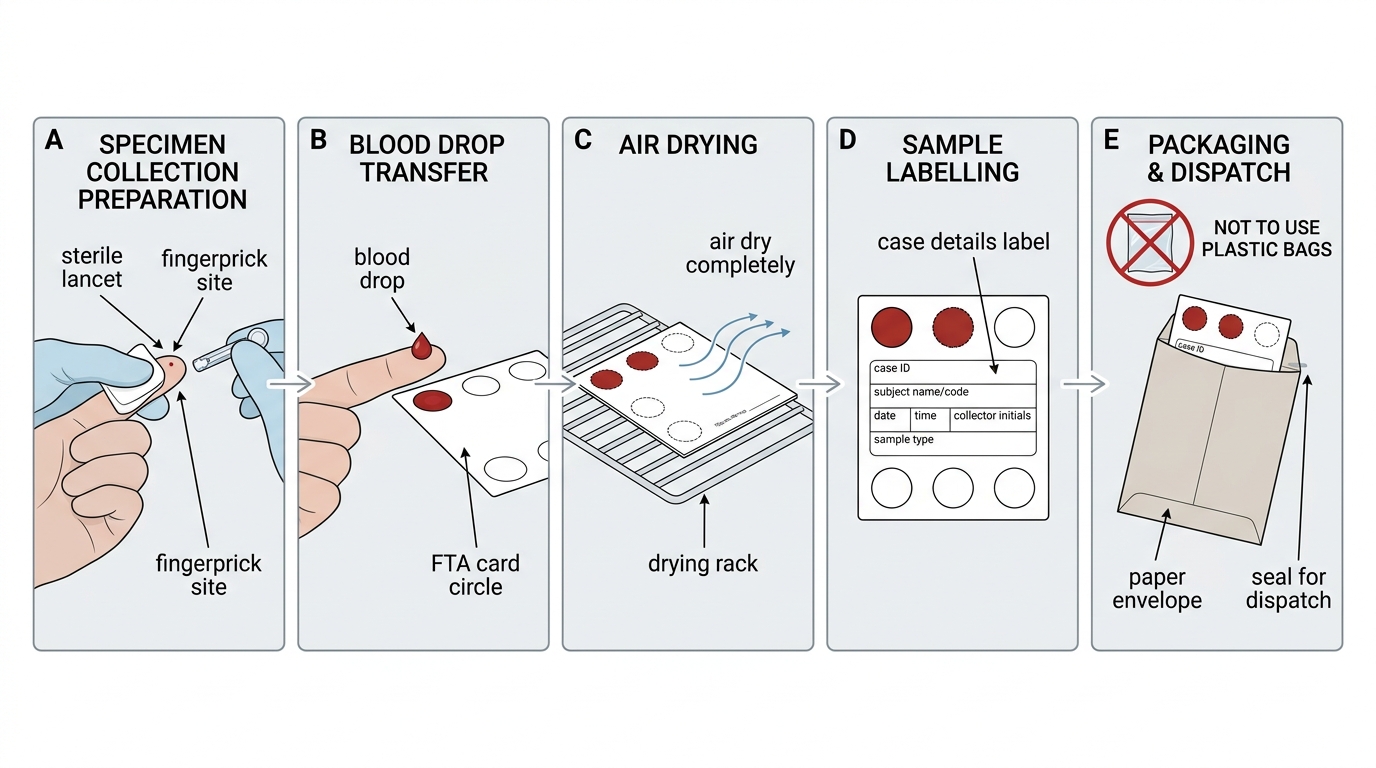
| FTA card (dried blood spot) | Lancet fingerprick onto FTA card; air-dry | Air-dried card in paper envelope | Room temperature; stable indefinitely | STR profile; archive |
| Buccal (cheek) swab | Sterile swab rubbed vigorously on buccal mucosa; air-dry | Air-dried swab in paper envelope | Room temperature; use soon or freeze | Reference sample for living person |
| Semen/vaginal swab | Posterior fornix swab; penile swab; air-dry | Air-dried swab in paper envelope | Room temperature; freeze for long-term | Sexual assault — individualise contributor |
| Tooth (for pulp) | Extract tooth aseptically; seal in dry container | Dry, sealed container | Room temperature | Decomposed/burned remains ID |
| Bone (marrow/cortex) | Excise 5-10 g cortical or trabecular bone aseptically | Sealed, clean container; freeze | −20°C | Skeletal remains ID |
Key rule across all DNA exhibit formats: air-drying (where applicable) before sealing is mandatory. Wet biological specimens sealed in plastic containers develop bacterial growth that degrades DNA within days. Paper envelopes allow moisture escape while protecting from contamination. Swabs must never be stored wet in sealed plastic bags. The exhibit is then labelled with case number, exhibit number, nature of specimen, date/time of collection, and collector's signature.
SELF-CHECK
A forensic medical officer collects a buccal swab from a living accused as a reference DNA sample. After collection, the best way to store and dispatch the swab to the FSL is:
A. Place the wet swab immediately in a sealed plastic zip-lock bag to preserve moisture
B. Air-dry the swab completely, then place in a paper envelope, label with case details, seal, and dispatch
C. Fix the swab in 10% formalin to preserve the cells for laboratory analysis
D. Refrigerate the wet swab at 4°C in a sealed glass tube for up to 7 days before dispatch
Reveal Answer
Answer: B. Air-dry the swab completely, then place in a paper envelope, label with case details, seal, and dispatch
A buccal swab must be air-dried before storage and dispatch. Wet biological specimens in sealed plastic containers develop bacterial growth within hours, and bacterial enzymatic activity degrades genomic DNA rapidly, potentially rendering the exhibit unusable for STR profiling. Air-drying halts this process; a paper envelope is then used (not plastic) because it allows residual moisture to escape while protecting from contamination. Option A (wet swab in plastic bag) creates the ideal environment for bacterial degradation of DNA — this is the most common error. Option C (formalin) is absolutely contraindicated for DNA specimens as it cross-links DNA (as it does proteins), preventing PCR amplification. Option D (refrigeration wet) may delay but does not prevent degradation and is not standard for buccal swabs.
Applied Practice: Reading Results, Troubleshooting & Chain of Custody
The ability to correctly read and interpret blood grouping results, troubleshoot discrepancies, and complete chain-of-custody documentation for DNA exhibits transforms technical knowledge into forensic practice. Each of these three competencies is developed here.
Troubleshooting ABO Forward-Reverse Discrepancy
Reading agglutination results correctly:
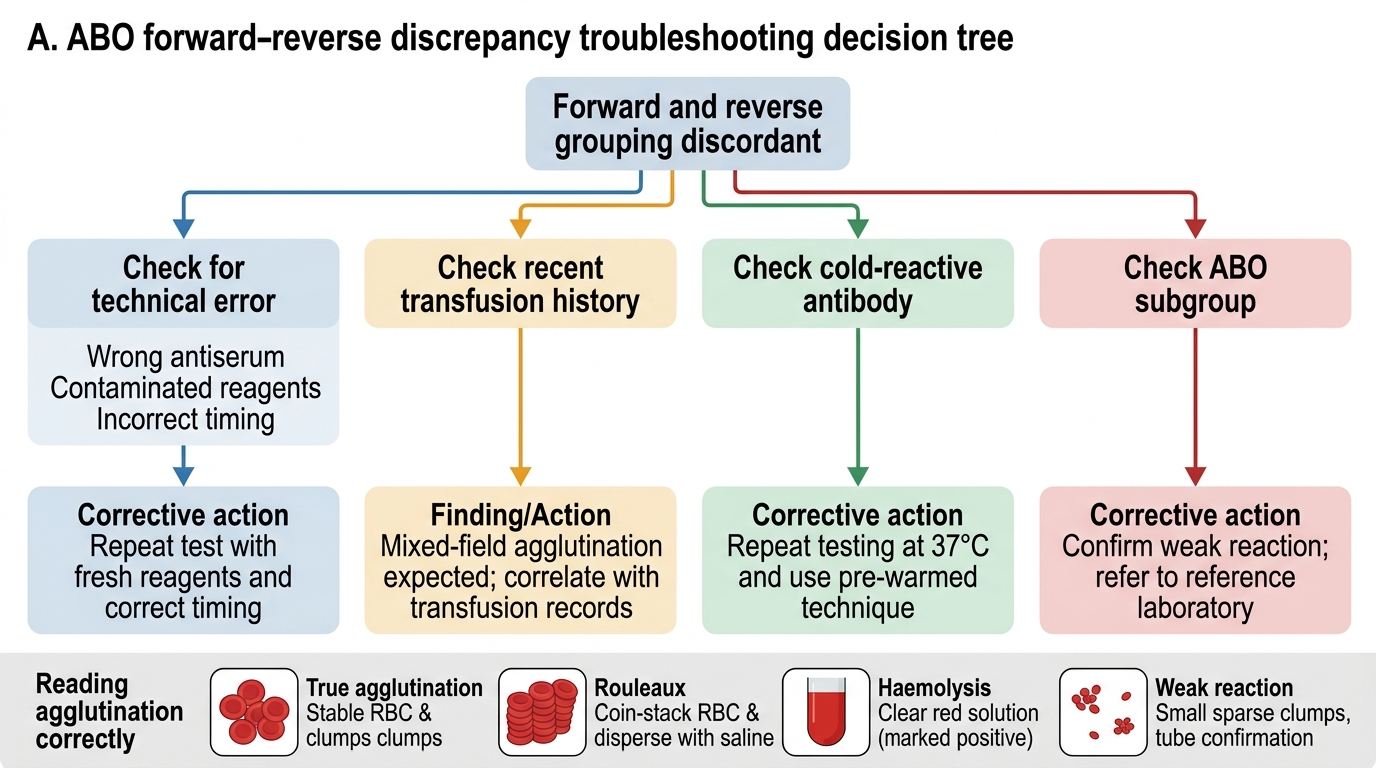
Agglutination in blood grouping is the visible clumping of red blood cells caused by cross-linking of surface antigens with their complementary antibodies. Correct reading requires distinguishing true agglutination from artefacts:
• True agglutination: large, stable, visible clumps that do not disperse when the mixture is re-rocked. Under a low-power microscope, discrete clumps of bound cells are visible.
• Rouleaux formation (false positive): RBCs stacking in coin-like columns under high plasma protein concentration; disperses with saline dilution — not true agglutination.
• Haemolysis (a positive result that looks negative): complement-mediated lysis of RBCs may cause the reaction to appear as a clear solution rather than a red cloudy one — this is a positive result and must not be read as 'no reaction'.
• Weak reactions: some blood group subgroups (A subgroups, B subgroups) produce weaker agglutination than the main phenotype. Weak reactions should be confirmed by tube method before reporting.
Troubleshooting ABO discrepancies:
Forward-reverse concordance is mandatory. Common causes of discrepancy:
• Technical error (most common): wrong antiserum used, contaminated reagents, inadequate mixing, reading too early or too late
• Cold-reactive antibodies: autoantibodies active at room temperature causing unexpected reactions in serum
• Recent blood transfusion: the patient's circulating red cells include donor cells, producing a mixed-cell population with mixed results in forward grouping
• ABO subgroups: weakly-expressed A or B antigens on RBCs that do not react with standard antisera at room temperature
All discrepancies must be resolved and documented before a group is reported. In a forensic context, an unresolved discrepancy means the grouping result is not reportable, and the exhibit may need to be retested.
Chain-of-custody completion for DNA exhibits:
The chain-of-custody form for a DNA exhibit records, at minimum:
• Exhibit number and description (e.g. "Exhibit 4: Buccal swab — accused Ramesh Kumar, sealed paper envelope")
• Date and time of collection; name, designation, and signature of collector
• Investigating officer's counter-signature confirming receipt
• Each subsequent transfer: from collector → IO → FSL reception — each transfer documented with signatures and dates
• Condition of the exhibit on receipt at each stage (envelope intact and sealed, wax seal present)
For DNA exhibits, an additional documentation requirement is the consent form when collecting from a living person for a non-criminal purpose (paternity, immigration, kinship). Voluntary, informed consent for DNA sampling must be documented in writing before collection. In criminal investigations, the law (BNSS) permits compelling a sample from an accused on court order; in that case, the court order document replaces the consent form in the chain-of-custody record.
Cross-contamination prevention in DNA exhibits:
DNA exhibits are particularly vulnerable to cross-contamination because PCR amplification can detect infinitesimal amounts of foreign DNA. Preventing contamination requires:
• Each exhibit handled with separate gloves or freshly gloved hands
• Each swab or tube opened once and closed immediately
• Exhibits from different individuals never opened in the same location simultaneously
• The examining doctor providing a reference DNA elimination sample (their own buccal swab) to the laboratory so that any inadvertent transfer of the examiner's own DNA can be identified and excluded from the analysis
SELF-CHECK
During ABO typing, the forward grouping shows Group A (agglutination with anti-A, no agglutination with anti-B). The reverse grouping shows agglutination with both A cells and B cells. This pattern represents:
A. Group O — the serum contains both anti-A and anti-B antibodies
B. A discrepancy — forward grouping suggests Group A but reverse grouping suggests Group O; the discrepancy must be investigated before a group is reported
C. Group A confirmed — reverse grouping agglutination with B cells is expected and confirms Group A
D. A technical error in the forward grouping — the result should be repeated
Reveal Answer
Answer: B. A discrepancy — forward grouping suggests Group A but reverse grouping suggests Group O; the discrepancy must be investigated before a group is reported
The correct answer is a discrepancy. The forward grouping (RBCs agglutinate with anti-A only) is consistent with Group A. For Group A, the reverse grouping should show agglutination with B cells ONLY (because Group A serum contains anti-B), and NO agglutination with A cells. Finding agglutination with BOTH A and B cells in the serum is inconsistent with Group A (it would suggest both anti-A AND anti-B in the serum, i.e. Group O). The forward-reverse results are discordant — this is a discrepancy that must be investigated (technical error, cold-reactive antibody, subgroup, or transfusion) before any blood group can be reported. It is not correct to report Group O (option A) or confirm Group A (option C) when there is a forward-reverse discrepancy. Merely repeating the forward grouping (option D) ignores the root cause.
CLINICAL PEARL
Air-dry before sealing — the single most important DNA exhibit rule: The most common cause of degraded DNA exhibits reaching the FSL is the examiner placing a wet swab in a sealed plastic bag. Plastic + moisture + bacteria = DNA degradation within hours, regardless of subsequent refrigeration. The rule is absolute: every biological swab must be air-dried completely (at room temperature in clean air, away from direct sunlight) before placement in a paper envelope. Paper allows residual moisture to escape. Paper envelopes are then sealed — not with plastic tape (which traps moisture) but with standard envelope gum or a label-seal. This single practice difference preserves or destroys the evidentiary value of the most critical exhibits in sexual assault and homicide investigations.
KEY TAKEAWAYS
This module has developed two practical forensic laboratory skills:
Blood grouping (FM14.7):
• ABO system: Landsteiner's Law — antigen on RBC, complementary antibody in serum (Group A: anti-B; Group B: anti-A; Group AB: neither; Group O: both anti-A AND anti-B)
• Rh-D typing: D antigen — Rh-positive (present) vs Rh-negative (absent); anti-D not naturally occurring
• Technique: forward grouping (test RBCs with anti-A, anti-B, anti-D) PLUS reverse/back grouping (test serum with A and B indicator cells) — results MUST be concordant
• Forensic stain methods: mixed agglutination (microscopic clumps around stain particles) and absorption-elution (for older/smaller stains)
• ABO secretors (~80% of population): ABO typing possible from semen, saliva, vaginal secretions in secretors
DNA exhibit collection (FM14.19):
• Fresh blood: EDTA tube (NOT NaF/oxalate) — at least 5-10 mL venous blood
• FTA card: fingerprick blood spotted and air-dried onto FTA card; room temperature stable; excellent for transport
• Buccal swab: living reference sample; air-dry before paper envelope — NEVER wet in plastic
• Semen/vaginal swab: air-dry before paper envelope; freeze for long-term storage
• Tooth (pulp) and bone: dry container; for decomposed/burned/skeletal remains
• Chain of custody: exhibit number, collector signature, IO counter-signature, sealed paper envelope, wax seal, consent form or court order
• Cross-contamination prevention: fresh gloves per exhibit, no simultaneous opening of different exhibits, examiner's reference elimination swab provided to lab
REFLECT
Work through these applied scenarios:
- You are performing a blood grouping examination on a stain recovered from the crime scene. The mixed agglutination result shows agglutination with anti-A antiserum but not with anti-B. The accused is Group B-positive. What is your conclusion, and how would you phrase this in a medicolegal report — as a finding or as an opinion?
- You are examining a sexual assault survivor and need to collect specimens for DNA profiling. You collect a vaginal swab, but the container available is a sealed plastic tube (designed for urine). You do not have paper envelopes available. What do you do? Does dispatching an inadequately stored swab — even if you document the constraint — fulfill your professional obligation?
- An accused in a paternity dispute refuses to provide a buccal swab voluntarily. The investigating magistrate asks you whether you can compel the collection. What is the legal position, and what documentation would you require before proceeding with a compelled sample?
- Explain why the forensic examiner's own reference DNA (elimination) sample is submitted alongside case exhibits. In what specific scenario would its presence in the analysis results be damaging to the case, and how would the laboratory use it to correct this?