Page 1 of 9
FM12.1-2 | Specimen Collection, Preservation & Locard's Principle — SDL Guide
Learning Objectives
- Enumerate and classify the biological specimens collected at medicolegal autopsy and crime scene investigations (FM12.1)
- Describe the appropriate method of collection, preservative agent, container, and labelling for each specimen type (FM12.2)
- Explain Locard's Exchange Principle and its practical implications for trace-evidence recovery
- Apply chain-of-custody documentation standards from collection to dispatch to FSL
- Interpret a forensic laboratory report in the context of a medicolegal case
INSTRUCTIONS
Forensic specimen collection is the backbone of every medicolegal investigation. Whether you are attending a scene of crime, conducting a medico-legal autopsy, or examining a living victim of violence, your ability to collect the right specimen, preserve it correctly, and hand it over with an unbroken chain of custody determines whether evidence reaches court in an admissible state. A single error — wrong preservative, broken seal, unlabelled container — can render months of forensic analysis inadmissible. This module grounds those decisions in the science and law that make them non-negotiable.
References
- KSN Reddy — Essentials of Forensic Medicine & Toxicology (textbook)
- BV Subrahmanyam — Modi's Medical Jurisprudence and Toxicology (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 28-year-old woman is found unconscious in her flat. Police suspect poisoning. The forensic medical officer arrives and must decide: which specimens to collect, how to preserve them, and how to ensure every container reaches the Forensic Science Laboratory with its evidentiary integrity intact. The officer collects blood in the correct fluoride-oxalate mixture, stomach contents in a plain sealed jar, liver in saturated saline — not formalin — and labels each with case number, exhibit number, site of collection, and their own signature and seal. Three months later, the toxicology report confirms organoarsenic poisoning. The conviction rests, in part, on that officer's knowledge of specimen science. This module is that knowledge.
WHY THIS MATTERS
As a future clinician, you will be called upon to perform medicolegal examinations, assist in autopsies, or examine assault survivors. In every scenario, your competence in specimen collection directly determines the medico-legal outcome. The courts have repeatedly ruled that improperly preserved or unlabelled specimens lack probative value — meaning that the best forensic analysis cannot rescue a broken chain of custody. Beyond legal admissibility, the correct preservative prevents chemical degradation that would yield a false-negative toxicology result. Understanding Locard's Exchange Principle keeps you alert to the trace evidence your own examination might create or destroy. This is not a procedural formality — it is the scientific and legal foundation of forensic evidence.
RECALL
Before proceeding, reflect on what you already know. From your earlier Forensic Medicine sessions, recall:
- The role of the Forensic Science Laboratory (FSL) in India — the government facility that receives and analyses biological evidence and issues reports used in criminal proceedings.
- The difference between a post-mortem examination (autopsy) and a medicolegal examination of the living — the types of specimens that arise from each context differ.
- Basic anatomy of the sites from which forensic specimens are taken — femoral vein for post-mortem blood, subclavian vein, vitreous humour, and visceral organs.
- The concept of chain of custody — the legally mandated record of who handled evidence, when, and in what condition, from scene to court.
If any of these feel uncertain, take a moment to review your notes before continuing.
Locard's Exchange Principle — The Foundation of Trace Evidence
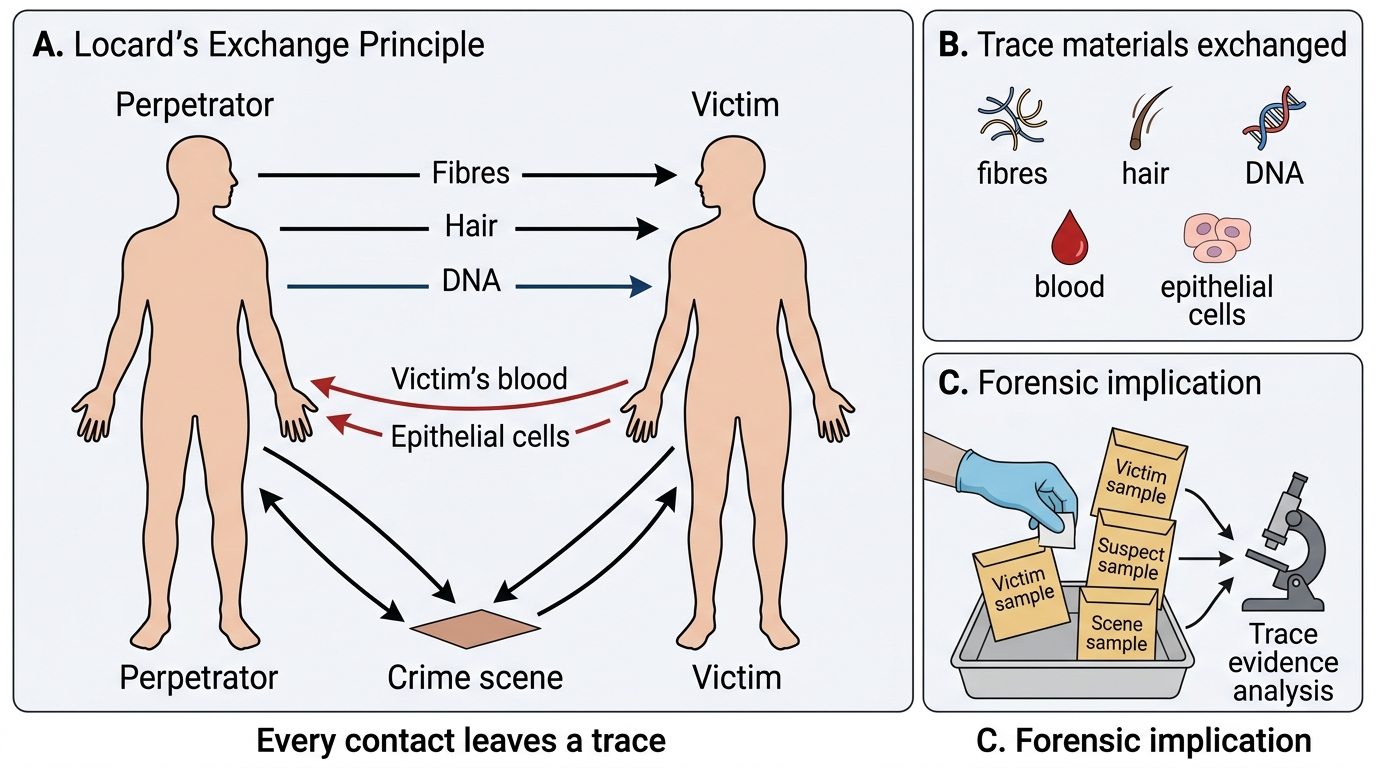
The entire science of trace-evidence investigation rests on a deceptively simple observation made by the French forensic scientist Edmond Locard in the early twentieth century. Locard, who directed the world's first scientific police laboratory in Lyon from 1910 onwards, articulated what is now called Locard's Exchange Principle: "Every contact leaves a trace." The principle holds that whenever two objects — or a person and an environment — come into physical contact, each takes away some material from the other and leaves behind some material in return. This bidirectional transfer is invisible at ordinary scales but detectable with the analytical tools of forensic science: microscopy, serology, DNA profiling, and toxicological assay.
In a homicide investigation, the perpetrator brings fibres from their clothing, skin cells under the victim's nails, boot-print soil on the floor — and leaves the scene carrying the victim's blood or hair. In a poisoning, the ingested compound leaves a metabolite signature in blood, urine, and viscera while the packaging leaves fingerprint and touch-DNA traces. In a sexual assault, semen, saliva, and epithelial cells from both persons exchange in forensically recoverable quantities. The operative word is contact — even transient contact transfers material; there is no such thing as a crime committed without trace evidence, only trace evidence not yet found.
The practical implication for the forensic medical officer is profound: every scene, every body, every surface is a potential donor and recipient of trace material. Your examination must be conducted with this bidirectional awareness — you must collect what the scene offers, and you must avoid depositing your own biological material (hair, DNA, respiratory droplets) onto the scene. This is why personal protective equipment is mandatory: it is not merely infection control — it is Locard's Principle in reverse, protecting the scene from the examiner.
Key term first uses in this block: Edmond Locard (1877–1966, French forensic pioneer); Locard's Exchange Principle (every contact leaves a trace); trace evidence (minute physical/chemical material transferred between objects during contact); FSL (Forensic Science Laboratory).

Forensic Specimen Collection and Dispatch Procedure
SELF-CHECK
Locard's Exchange Principle states that every contact leaves a trace. Which of the following correctly describes the DIRECTIONALITY of this transfer?
A. The victim always deposits material on the perpetrator, never vice versa
B. Transfer occurs only from the perpetrator onto the crime scene
C. Transfer is bidirectional — both objects or persons exchange material with each other
D. Transfer occurs only in soft-tissue contact, not in hard-surface contact
Reveal Answer
Answer: C. Transfer is bidirectional — both objects or persons exchange material with each other
Locard's principle is bidirectional: every physical contact results in an exchange — the perpetrator leaves material on the scene and takes material from it. This bidirectionality is what makes the principle powerful: the investigator looks for what the scene received from the suspect AND what the suspect carried away from the scene. Options A and B describe unidirectional transfer, which is incorrect. Option D is wrong because trace transfer applies to all contact types including footwear on hard floors.
Scientific Basis of Biological Specimens in Forensic Analysis
The medicolegal value of a biological specimen derives from the specific analyte it contains and the stability of that analyte over time. Choosing the wrong specimen or the wrong preservative degrades or destroys the analyte, making the entire collection effort scientifically worthless. The NMC competency FM12.1 enumerates eleven principal forensic specimen types, and every medical student must understand both what each specimen reveals and from where it is obtained.
The eleven specimen types are systematically grouped below:
Body fluids for chemical and serological analysis:
• Blood — the primary specimen for alcohol, drugs, and DNA. Ante-mortem blood is drawn from a peripheral vein; post-mortem blood is best obtained from the femoral or subclavian vein (cardiac blood is unsuitable due to redistribution artefact). Blood also supports ABO/Rh grouping and DNA profiling.
• Urine — valuable for drug metabolites and toxic compound excretion products; typically collected in a plain, clean, sealed container.
• Semen — critical in sexual assault investigations; supports DNA profiling, motility assessment (ante-mortem freshness), and ABO secretor status.
• Saliva — contains epithelial cells and amylase; useful for DNA profiling from bite marks, licked envelopes, and drinking vessels.
• Vaginal smear — obtained by swabbing the posterior fornix; detects spermatozoa, DNA, and lubricant traces in sexual assault cases.
• Faeces — collected in poisoning cases where the toxin is excreted via the gut; also relevant in some infectious disease medicolegal cases.
Solid and semi-solid specimens:
• Skin — excised from contact sites (bite marks, friction surfaces) for epithelial DNA and trace material.
• Nails — clippings or scrapings yield the victim's and possibly the perpetrator's DNA, fibres, soil, and biological material trapped under the nail edges during struggle.
• Tooth pulp — teeth survive decomposition, fire, and extreme environmental conditions far better than soft tissue; pulp yields DNA for identification in decomposed or skeletonised remains.
• Viscera — liver, brain, kidney, and stomach contents are the primary specimens for toxicological analysis in suspected poisoning deaths. Liver is the principal site of drug/toxin metabolism and concentration.
• Skull — submitted for age estimation (skull morphology), identification (facial reconstruction from skull base), and trauma pattern analysis (fracture mechanics).
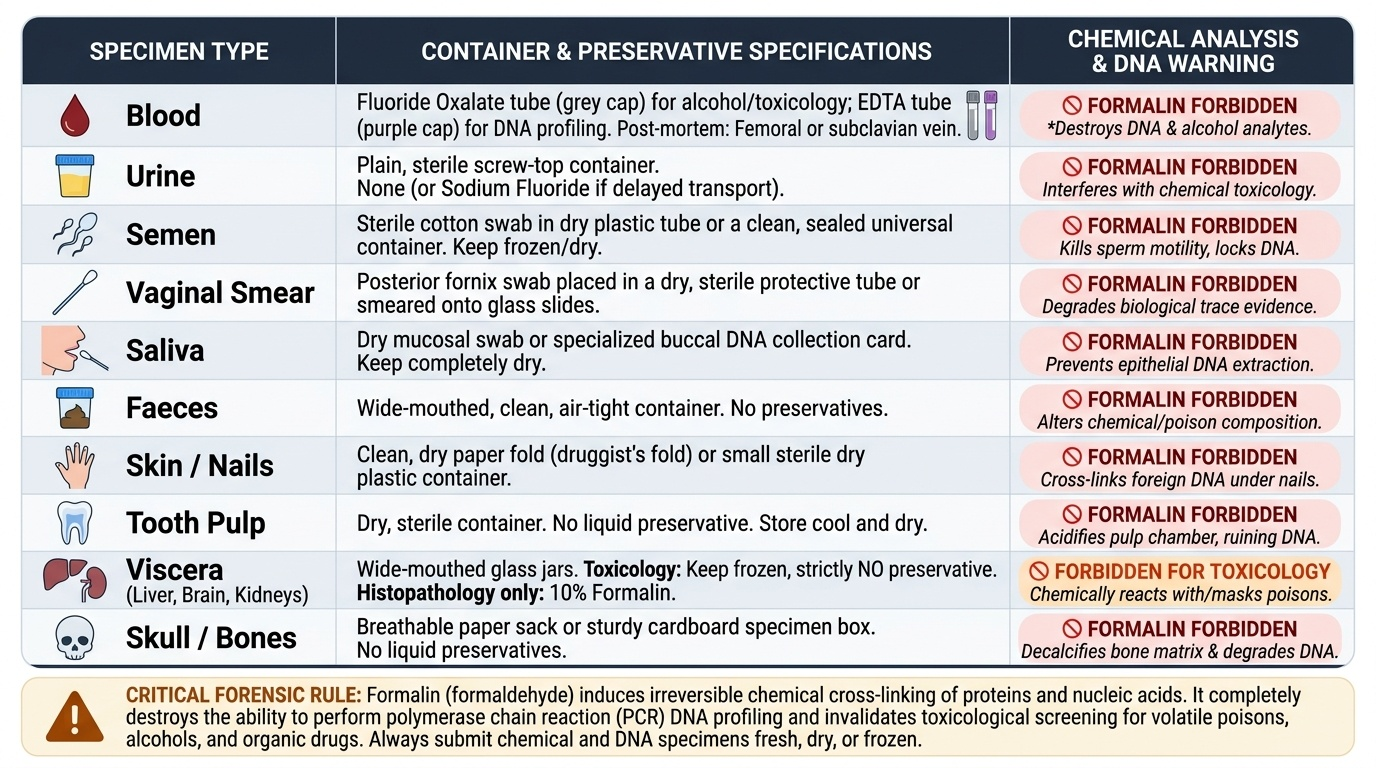
Provided image
| Specimen | Collection Site | Container & Preservative | Principal Purpose | Formalin? |
|---|---|---|---|---|
| Blood (chemical) | Femoral/subclavian vein (PM); peripheral vein (AM) | Fluoride-oxalate tube (NaF + K oxalate) | Alcohol/drug assay, DNA | NEVER |
| Urine | Bladder | Plain, clean sealed container | Drug metabolites | Never |
| Semen/vaginal swab | Posterior fornix / penile swab | Plain swab, sealed tube | Sexual assault DNA | Never |
| Saliva | Oral cavity swabs | Sterile swab, air-dried | DNA, bite marks | Never |
| Faeces | Rectum / collected specimen | Plain sealed container | Toxin excretion | Never |
| Skin/nails | Contact sites, nail scrapings | Sealed paper envelope | DNA, trace | Never |
| Tooth pulp | Extracted tooth | Sealed dry container | ID in decomposed | Never |
| Viscera (liver, brain, kidney) | Autopsy | Saturated NaCl solution (primary); rectified spirit ONLY if NaCl unavailable | Toxicology | ABSOLUTELY NEVER |
| Skull | Autopsy | Dry sealed container | Age/ID/trauma | N/A |
Collection, Preservation & Labelling Methods
The method of collection and the choice of preservative are inseparable decisions — you cannot choose the method without knowing the preservative, because the preservative dictates the container type, which influences the collection technique. The standard authoritative reference for Indian forensic practice is Reddy's Essentials of Forensic Medicine & Toxicology and Modi's Medical Jurisprudence and Toxicology, both of which provide the preservation guidelines summarised here.
Locard's Exchange Principle in Homicide Investigation
Blood collection and preservation requires particular attention because multiple types of blood specimens may be collected from the same case for different purposes. Blood for chemical analysis (including blood alcohol concentration) must be collected into a fluoride-oxalate mixture (sodium fluoride + potassium oxalate). NaF inhibits bacterial glycolysis that would otherwise generate or consume ethanol in the tube, causing false results; oxalate acts as an anticoagulant. At least 10 mL of blood is recommended. Blood for DNA profiling may be collected into EDTA tubes or onto FTA cards (dried bloodstain cards). Blood for ABO grouping uses standard EDTA or plain tubes depending on the method. The forensic practitioner must label each tube with its specific purpose so the laboratory applies the correct analytical protocol.
Viscera preservation is the most frequently misunderstood area and the most common source of error. The following rule is absolute and must be memorised: formalin MUST NEVER be used as a preservative for viscera destined for chemical/toxicological analysis. Formalin (formaldehyde in water) is a fixative that cross-links proteins — it is used for histopathological tissue preservation where cellular architecture must be preserved. However, it chemically modifies and destroys the volatile and non-volatile toxic compounds that the chemical analyst is seeking to detect. The correct preservative for viscera (liver, brain, kidney, stomach contents) is saturated sodium chloride solution (saturated NaCl). If saturated NaCl is not available at the scene, rectified spirit (95% ethanol) may be used as a substitute, but this is the exception — rectified spirit is alcohol and can interfere with alcohol quantification assays; the laboratory must be informed if rectified spirit was used. Each visceral organ is placed in a separate sealed glass container with sufficient preservative to immerse it completely.
Labelling requirements must be completed before the container leaves the collection site. Every specimen container must bear:
• Case number and FIR number
• Name (if known) or description ("Unknown male, found at...") of the deceased/living subject
• Exhibit number (sequentially assigned)
• Nature of specimen (e.g. "Liver for chemical analysis")
• Date and time of collection
• Name, designation, and signature of the collecting officer
• Counter-signature of the investigating police officer (IO)
After labelling, the container is sealed with wax and the seal is impressed with an official stamp. This wax seal is the physical evidence that the container has not been opened since collection. The absence of an intact wax seal is grounds for challenging admissibility.
SELF-CHECK
A forensic medical officer collects liver, brain, and kidney from a suspected poisoning death. Which preservative should be used for these visceral specimens intended for toxicological analysis?
A. 10% formalin — the standard tissue preservative
B. Rectified spirit (95% ethanol) — always used for viscera
C. Saturated sodium chloride (NaCl) solution — primary preservative for viscera
D. Fluoride-oxalate mixture — the same as blood preservative
Reveal Answer
Answer: C. Saturated sodium chloride (NaCl) solution — primary preservative for viscera
Saturated sodium chloride (NaCl) solution is the primary preservative for visceral specimens (liver, brain, kidney, stomach contents) intended for toxicological/chemical analysis. Formalin (option A) is absolutely contraindicated — it destroys the toxic compounds the laboratory must detect. Rectified spirit (option B) may be used ONLY when saturated NaCl is unavailable — it is the fallback, not the standard, and the laboratory must be informed because it can interfere with alcohol assays. Fluoride-oxalate (option D) is for blood specimens to inhibit glycolysis and prevent enzymatic alcohol degradation.
Chain of Custody, Dispatch & Interpretation of Reports
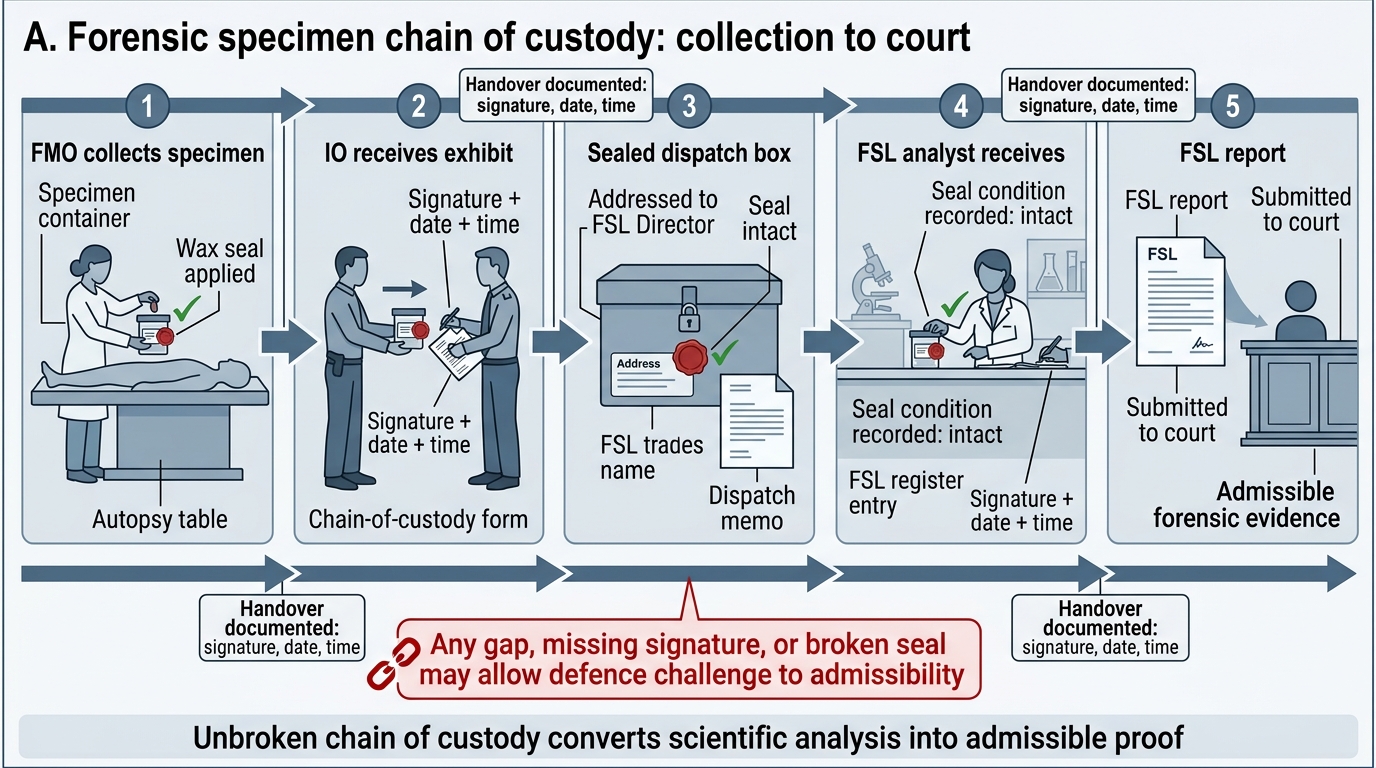
The chain of custody is the continuous, documented record of who had possession of an exhibit, when they received it, in what condition, and to whom they transferred it. In Indian criminal procedure, a break in the chain of custody
Forensic Specimen Chain of Custody
The chain begins the moment the forensic officer collects and seals a specimen at the scene or autopsy table. Every subsequent transfer — from the officer to the investigating officer, from the IO to the FSL reception, from FSL reception to the assigned analyst, from the analyst to secure storage, and ultimately from FSL to court — must be documented with signatures, dates, and times. The sealed wax condition of the container must be verified and recorded at each handover. If the wax seal is found broken or tampered with on receipt, the FSL must note this in writing before proceeding — the exhibit's evidentiary value is already compromised.
Dispatch procedure to FSL follows a standardised protocol. Specimens are placed in a dispatch box (a strong cardboard or wooden box), which is then sealed, addressed to the Director of the concerned FSL, and forwarded through the investigating officer with a covering letter. The covering letter (also called the forwarding letter or Form No. 3 in many states) must specify: the case particulars, FIR details, the nature and number of exhibits, specific tests requested, and the history of the case relevant to guiding the analyst. Without adequate case history, the analyst cannot optimise the analytical approach — for example, knowing that the victim was suspected of arsenic poisoning directs the analyst to run atomic absorption spectroscopy for heavy metals rather than a general toxicology screen.
Interpretation of FSL reports is a clinical and legal skill. The FSL report will state: the condition of the sealed containers on receipt (intact/broken), the methods used, the analytical findings, and an opinion. The forensic medical officer reading this report in a medicolegal context must understand:
• A negative toxicology result does NOT prove absence of a toxic substance — it proves absence above the detection threshold of the method used. Many poisons are not part of routine screening panels and require specific targeted assays.
• Reference ranges for drug and ethanol concentrations must be interpreted in the context of post-mortem redistribution — post-mortem blood concentrations of many drugs are higher than ante-mortem concentrations due to leakage from tissues, gastric re-diffusion, and microbiological changes.
• The FSL opinion is advisory, not conclusive — the court weighs it alongside clinical, pathological, and circumstantial evidence. The forensic medical officer may be called as an expert witness to explain the report.
Chain-of-custody documentation and the FSL report together constitute the forensic evidence trail — the link between the crime scene and the courtroom. Every physician who practices forensic medicine must be conversant with both.
SELF-CHECK
The defence counsel in a murder trial argues that the toxicology evidence should be excluded. Which single finding provides the strongest ground for challenging admissibility of the FSL report?
A. The FSL report was signed by an analyst rather than the Director
B. The wax seal on the specimen container was found broken on receipt at the FSL
C. The specimens were collected at night rather than during daylight hours
D. The FSL used atomic absorption spectroscopy rather than chromatography
Reveal Answer
Answer: B. The wax seal on the specimen container was found broken on receipt at the FSL
A broken wax seal on receipt at the FSL is the strongest ground for challenging admissibility because it demonstrates a potential break in the chain of custody — the container may have been opened, and the specimen may have been contaminated, substituted, or tampered with between collection and analysis. Options A, C, and D describe procedural variations that do not break the chain of custody: analyst vs Director signatures do not invalidate the report; time of collection is irrelevant to admissibility; and choice of analytical method is a scientific decision within the FSL's discretion.
CLINICAL PEARL
The formalin trap: The single most dangerous error in forensic specimen handling is preserving viscera in formalin for chemical analysis. Formalin is the correct preservative only for histopathological specimens — tissue sections going to the pathology laboratory to study cellular architecture. It is catastrophically wrong for toxicology specimens: formaldehyde reacts with aldehydes, ketones, and amino groups of toxic compounds, destroying them chemically. The resulting "negative" toxicology report is not a true negative — it is an analytical artefact of the wrong preservative. In examinations and in practice, the rule is: saturated NaCl → viscera for toxicology; formalin → histopathology only. Write it, remember it, never confuse it.
KEY TAKEAWAYS
This module has covered two interconnected competencies that underpin all forensic laboratory work:
Locard's Exchange Principle: Every contact leaves a trace — bidirectional transfer of physical and biological material occurs in every contact event. The forensic examiner's task is to preserve, collect, and document this trace evidence before it is lost or contaminated.
Forensic specimen types (FM12.1): Eleven principal specimens — blood, urine, semen, faeces, saliva, skin, nails, tooth pulp, vaginal smear, viscera, and skull — each collected from specific sites and valuable for specific analytes.
Collection, preservation, labelling (FM12.2):
• Blood (chemical analysis): NaF + potassium oxalate (fluoride-oxalate) tube
• Viscera (toxicology): saturated NaCl solution — NEVER formalin
• All containers: labelled with case number, exhibit number, specimen type, date/time, collector's signature, and IO counter-signature; sealed with wax stamp
Chain of custody: The unbroken documented record from collection to court. A broken seal = inadmissible evidence. The covering letter to FSL must include case history and specific tests requested.
Interpreting FSL reports: A negative result means below the detection threshold of the method used, not absolute absence. Post-mortem redistribution inflates many drug concentrations; this must be accounted for in interpretation.
REFLECT
Consider the following scenario: You are assisting at an autopsy of a suspected poisoning death. You discover that the previous medical officer, in a hurry, preserved all visceral specimens in formalin because it was the only fixative available. The police are pressing for immediate dispatch to the FSL.
Reflect on these questions:
1. What will the toxicological analysis yield from these formalin-preserved specimens, and why?
2. What are your obligations at this point — can you dispatch these specimens? Should you document the error?
3. Are there any remaining specimen sources (vitreous humour, urine, blood from a peripheral vessel) that might still yield valid toxicological data?
4. How does this scenario illustrate why Locard's Exchange Principle must be paired with rigorous collection methodology — finding a trace is only useful if you can prove it was collected correctly?