Page 8 of 23
FM10.{4-5,28} | Code of Medical Ethics & Professional Misconduct — SDL Guide
Learning Objectives
- Describe the key provisions of the NMC Code of Medical Ethics Regulations 2002 regarding conduct, etiquette, and ethics in medical practice
- Define and identify categories of unethical practice including dichotomy (fee-splitting) and canvassing
- Explain the disciplinary mechanism: the Disciplinary Committee, warning notice, penal erasure, and restoration to the register
- Demonstrate familiarity with the legal obligations governing medical practice under the NMC framework
INSTRUCTIONS
The Code of Medical Ethics does not exist to constrain good doctors — it exists because medicine's power can be misused, and the profession has an obligation to the public to police itself. For a doctor who intends to practise with integrity, most of the Code's requirements will feel obvious. But understanding the Code in detail — including its specific prohibitions, the categories of misconduct, and the consequences of violation — is essential not only to avoid inadvertent breaches but to recognise and respond appropriately when you encounter ethical violations by colleagues.
References
- KSN Reddy — Essentials of Forensic Medicine & Toxicology (textbook)
- BV Subrahmanyam — Modi's Medical Jurisprudence and Toxicology (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A senior orthopaedic surgeon at a private hospital has an informal arrangement with two diagnostic imaging centres: for every patient he refers for MRI, he receives a 'referral fee' — a percentage of the imaging cost paid to him, without the patient's knowledge. The patient pays the full MRI fee, the imaging centre profits, and the surgeon receives an undisclosed payment. When challenged by a junior colleague, the surgeon shrugs: 'Everyone does it. It's how private practice works.' But the junior colleague knows this is wrong. She has just studied the NMC Code of Medical Ethics Regulations 2002. This arrangement is dichotomy — illegal fee-splitting — and it is specifically prohibited as professional misconduct. Understanding why this is wrong, and what the consequences are, is what this module is about.
WHY THIS MATTERS
The NMC Code of Medical Ethics Regulations 2002 is the operational document that defines the boundaries of acceptable professional conduct for every registered medical practitioner in India. It is not merely aspirational — it has regulatory force under the NMC Act 2020. Violations can result in formal disciplinary action by the State Medical Council or EMRB, including warning notices and penal erasure from the medical register. For a medical student about to join professional practice, knowing what the Code prohibits — advertising, canvassing, dichotomy, covering unqualified practitioners, issuing false certificates — is a practical requirement. Ignorance of the Code is not a defence before a disciplinary body.
RECALL
Before we begin:
- In the previous module (me3-nmc), we learned that the EMRB is the NMC board responsible for ethics and registration. What disciplinary powers does the EMRB exercise? What is the relationship between EMRB and State Medical Councils in disciplinary matters?
- Think about the word 'infamous' — in common usage, it means 'well known for something bad.' In medical ethics, 'infamous conduct' has a technical meaning. What do you think it means for professional purposes?
- You are referred a patient by a GP colleague who expects a 'cut' from the consultation fee. What is this called, and is it acceptable under the Code of Medical Ethics?
Legal and Professional Context: Why a Code of Ethics Governs Medical Practice
The Code of Medical Ethics represents the professional community's own articulation of the standards to which its members will be held. It differs from general criminal law (which applies to everyone) and civil law (which creates remedies for specific harms) in that it creates obligations specific to the professional role — obligations that arise from the particular trust placed in doctors by patients and the particular power that medical practitioners hold.
The operative framework for Indian medical practitioners is the NMC Code of Medical Ethics Regulations 2002 — the Indian Medical Council (Professional Conduct, Etiquette and Ethics) Regulations 2002, originally made under the MCI and the IMC Act 1956, now adopted and operative under the NMC Act 2020. Although drafted under the predecessor legislation, the Code continues in force and represents the authoritative statement of professional conduct standards for Indian doctors.
The Code operates within a broader legal framework that includes:
- NMC Act 2020 — the primary statute governing medical registration and professional conduct
- Consumer Protection Act 2019 — under which medical services are 'services' and a patient can be a 'consumer' with legal recourse for deficiency of service
- Indian Penal Code — IPC 304A (causing death by negligence), IPC 499 (defamation), and other sections relevant to medical practice
- Indian Evidence Act — governing what a doctor may disclose and the confidentiality of medical records
The Code addresses the doctor in three professional relationships:
1. Towards patients — the primary relationship, governed by duties of care, consent, confidentiality, and referral
2. Towards colleagues — the professional community relationship, governed by rules about consultation, advertising, and collegial conduct
3. Towards society — the public health relationship, governed by duties of notification, public safety, and the responsibilities of a licensed professional
The Code of Medical Ethics 2002: Conduct, Etiquette and Ethics
The NMC Code of Medical Ethics Regulations 2002 is organised around the concept of the registered medical practitioner's duties — what is expected, what is forbidden, and what constitutes a breach serious enough to warrant disciplinary action. The Code uses the concepts of 'conduct,' 'etiquette,' and 'ethics' to capture different dimensions of professional behaviour.
Medical Ethics in the Code refers to the principles governing the doctor-patient relationship: the duties of care and competence, the requirement of informed consent, the obligation of confidentiality, and the responsibilities towards vulnerable patients. The ethical provisions establish the doctor's positive obligations — what they must do.
Medical Etiquette refers to the customs and conventions governing relations between medical practitioners: how to behave towards colleagues, how to conduct consultations and referrals, how to communicate professionally. Etiquette violations (e.g. publicly disparaging a colleague's clinical judgment) may not warrant erasure but breach professional standards.
Conduct — and specifically infamous conduct — is the critical concept for disciplinary purposes. Infamous conduct in a professional respect is conduct that would be regarded by fellow practitioners as disgraceful or dishonourable — the ethical touchstone for erasure from the register. It is not defined exhaustively but is assessed against the standards of the profession itself.
Key positive obligations under the Code:
- Maintaining adequate clinical competence and keeping knowledge up to date
- Obtaining valid informed consent before procedures
- Maintaining confidentiality of patient information, subject to specified exceptions
- Maintaining accurate and complete clinical records
- Referring patients whose conditions are beyond the practitioner's competence
- Reporting notifiable diseases and conditions as required by law
- Treating patients without discrimination on grounds of caste, religion, nationality, or ability to pay in emergencies
- Providing emergency treatment in any emergency situation, regardless of whether payment is guaranteed
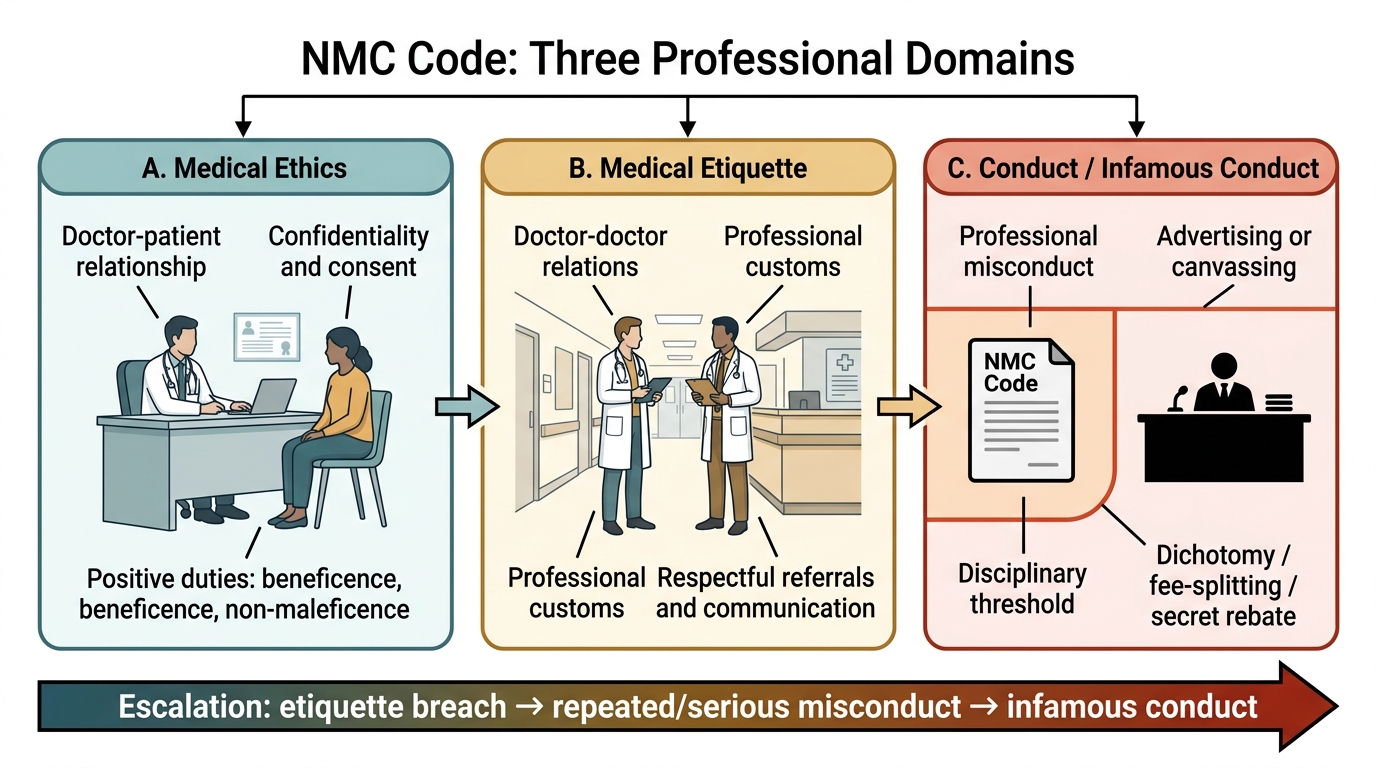
Three Domains of the NMC Code
Unethical Practices and Dichotomy
The Code specifically prohibits a defined set of practices that are categorised as professional misconduct. These are not merely aspirational standards — breach of these specific prohibitions is the most common basis for disciplinary proceedings.
Advertising and canvassing are prohibited. A registered medical practitioner may not advertise their services, skills, or fees in a manner that amounts to 'touting' for patients. The Code permits a limited, factual announcement of change of address, specialisation, or opening of a new practice — but prohibits claims of special expertise, endorsement of products, or any form of commercial promotion of one's practice. Canvassing (actively soliciting patients through intermediaries or by paying commissions to referrers) is specifically prohibited.
Dichotomy is one of the most significant specific prohibitions. Dichotomy (also called fee-splitting or secret rebate) is an arrangement — explicit or implied — by which a practitioner pays or receives a commission, percentage, or other benefit in return for referring a patient to another practitioner, diagnostic facility, pharmaceutical company, or any other service. Dichotomy is prohibited because it creates a conflict of interest between the doctor's financial benefit and the patient's best interest: a doctor who receives a referral fee has a financial incentive to recommend tests, treatments, or specialists based on payment rather than clinical need. The patient, unaware of the arrangement, cannot make an informed choice. Dichotomy includes:
- Paying or receiving 'cuts' for referring patients to consultants or diagnostic centres
- Receiving commissions from pharmaceutical companies for prescribing specific products ('gifts' beyond nominal value)
- 'Ghost surgery' — performing surgery without the patient's knowledge while the named surgeon receives the fee
Covering for unqualified practitioners — the Code prohibits a registered practitioner from lending their name to, prescribing for, or otherwise authorising the practice of medicine by a person who is not registered.
Issuing false certificates — providing medically false certificates (fitness certificates, sick leave certificates, disability certificates, age certificates) for financial gain or as a favour is a specific prohibited act and may also constitute an offence under IPC.
Secret remedies — prescribing or recommending remedies whose composition is not disclosed (proprietary formulations for which the doctor has a financial interest) is prohibited.
| Category | Description | Example | Primary Consequence |
|---|---|---|---|
| Advertising/Canvassing | Commercial promotion of practice or soliciting patients | Paid newspaper advertisement claiming 'best cardiologist in the city' | Warning notice / erasure for repeated violation |
| Dichotomy (fee-splitting) | Paying/receiving commission for referrals | Receiving 20% of diagnostic fee from an MRI centre | Penal erasure — a serious misconduct |
| Covering unqualified practitioners | Allowing non-registered persons to practise under one's name | Signing prescriptions for a quack using one's name | Disciplinary action; possible criminal prosecution |
| Issuing false certificates | Providing medically false documents | Signing false fitness certificate for a fee | Penal erasure; possible IPC prosecution |
| Secret remedies | Prescribing undisclosed proprietary formulations for personal gain | Selling patient homemade capsules of 'special' herbs | Disciplinary action |
SELF-CHECK
An orthopaedic surgeon receives ₹500 for every patient referred to a specific physiotherapy centre, without the patient's knowledge. Under the NMC Code of Medical Ethics 2002, this is best classified as:
A. Acceptable professional custom — referral incentives are not explicitly prohibited
B. Advertising — the doctor is promoting the physiotherapy service
C. Dichotomy (fee-splitting) — an undisclosed commission arrangement that creates a conflict of interest
D. Canvassing — the doctor is soliciting patients for a third party
Reveal Answer
Answer: C. Dichotomy (fee-splitting) — an undisclosed commission arrangement that creates a conflict of interest
This arrangement is dichotomy (fee-splitting). Dichotomy is the receipt or payment of a commission, rebate, or benefit in return for referring a patient to another service. It is specifically prohibited under the NMC Code because it creates a conflict between the doctor's financial interest and the patient's best clinical interest. The patient is unaware of the arrangement and cannot make an informed choice. Advertising refers to self-promotion; canvassing refers to soliciting patients through intermediaries.