Page 18 of 23
FM10.22-23 | Medical Oaths & the Declaration of Geneva — SDL Guide (Part 2)
Administration of the Oath: Procedure and Indian Practice
The administration of the medical oath at Indian graduation ceremonies is a formal procedure specified by the NMC under the NMC Act 2020. Understanding this procedure is specifically required by the FM10.22 competency ('explain Oath — Hippocrates, Charaka and Sushruta and procedure for administration').
Procedure for administration of the medical oath in India:
At the convocation or graduation ceremony of a medical college:
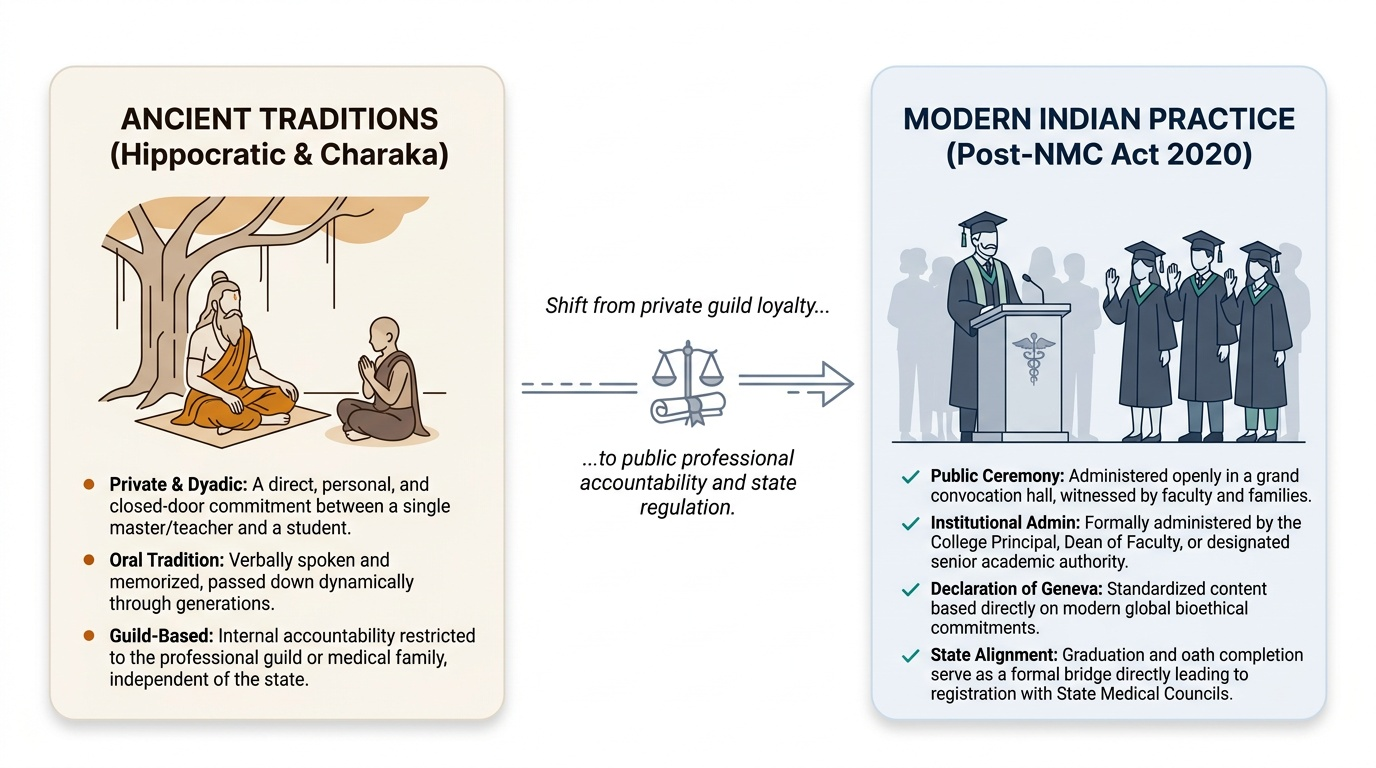
1. Setting: The oath is administered publicly, in the presence of faculty, graduating students, and typically invited guests including family members. The public nature of the ceremony is deliberate — the oath is a social contract, and its public administration makes it witnessed and accountable.
2. Administering authority: The oath is typically administered by the Principal of the medical college, the Dean of the Faculty of Medicine, or another senior faculty member designated for the purpose.
3. Form: The graduates stand (or raise the right hand, as per institutional tradition) and recite the oath — either in unison or as an affirmation (answering 'I do' to each clause read by the administrator).
4. Content: The oath administered is based on the Declaration of Geneva. The exact wording may vary slightly between institutions, but the core commitments of the 2017 Declaration of Geneva are incorporated.
5. Significance in registration: The completion of the graduation ceremony, including the oath, is associated with the conferral of the MBBS degree. Registration then proceeds separately through the State Medical Council (as detailed in me3-nmc).
Historical note on the Hippocratic administration procedure: In the ancient Hippocratic tradition, the oath was administered by the teacher (guru) to the student upon completion of training — a private, dyadic commitment between teacher and student. In the Indian Charaka tradition, the initiation ceremony was similarly conducted by the guru in the guru-shishya setting. The move to a public, institutional ceremony is a modern feature that reflects the shift from guild-based to state-regulated medicine.
Provided image
Applied Practice: Relevance of Oaths to Contemporary Medical Conduct
The Declaration of Geneva is sometimes dismissed as idealistic — a statement of aspirations rather than a practical guide to clinical decision-making. But each of its clauses connects directly to specific clinical and ethical challenges.
'I will put the health and wellbeing of my patient first.'
This is the operative principle in conflict-of-interest situations — when the doctor's financial interest (through fee-splitting, pharmaceutical incentives), time pressure (turning away a complex patient), or personal preferences diverge from the patient's best interest. It is also the basis for the duty of emergency care.
'I will respect the autonomy and dignity of my patient.'
This is the Declaration's incorporation of the principle of respect for autonomy — the basis for informed consent, the duty to explain diagnosis and treatment options, and the obligation to respect a competent patient's refusal.
'I will respect the secrets that are confided in me, even after the patient has died.'
This is professional secrecy — the confidentiality obligation survives the clinical relationship and extends beyond death. Relevant when families request disclosure of a deceased patient's records, or when historical records are sought for legal purposes.
'I will not permit considerations of [personal characteristics] to intervene between my duty and my patient.'
This is the non-discrimination clause — directly applicable in Indian clinical practice where caste, religion, economic status, HIV status, or sexual orientation may create unconscious bias in treatment decisions.
'I will attend to my own health, wellbeing and abilities.' (2017)
This clause makes physician self-care an ethical duty — not merely a personal preference. Impaired physicians put patients at risk; addressing impairment (including burnout, substance use, or mental illness) is an ethical professional responsibility.
'I will not use my medical knowledge to violate human rights and civil liberties, even under threat.' (2017)
In a forensic medicine context, this clause is particularly relevant: a forensic doctor who is asked to certify false injuries, falsify cause of death, or provide a medical opinion under pressure from authorities must refuse — this clause makes that refusal an ethical obligation, not merely a personal choice.
The oath as a living commitment rather than a one-time recitation:
The oath's relevance to contemporary practice lies not in having recited it once at graduation, but in the ongoing question: is what I am doing consistent with what I committed to? This reflective practice — checking one's conduct against one's commitments — is what transforms the oath from a ritual into a living professional orientation.
SELF-CHECK
Which of the following clauses was ADDED to the Declaration of Geneva in the 2017 WMA revision and was NOT present in earlier versions?
A. 'I will respect the secrets that are confided in me, even after the patient has died'
B. 'I will put the health and wellbeing of my patient first'
C. 'I will attend to my own health, wellbeing and abilities in order to provide care of the highest standard'
D. 'I will practise my profession with conscience and dignity'
Reveal Answer
Answer: C. 'I will attend to my own health, wellbeing and abilities in order to provide care of the highest standard'
The physician health clause — 'I will attend to my own health, wellbeing and abilities in order to provide care of the highest standard' — was added in the 2017 WMA revision. The other three clauses were present in earlier versions of the Declaration. The 2017 revision also added the human rights clause: 'I will not use my medical knowledge to violate human rights and civil liberties, even under threat.' These two additions are the distinguishing feature of the 2017 version.
CLINICAL PEARL
The Declaration of Geneva's relevance is most visible in the moments when it is hardest to follow. The physician health clause matters most when a doctor has been working 36-hour shifts and is making decisions at cognitive capacity below their usual standard — and has the internal honesty to acknowledge this and seek relief. The human rights clause matters most when a forensic doctor is pressured by a superior officer to certify injuries that are inconsistent with the claimant's account. The confidentiality clause matters most after a patient has died and their family is demanding access to records the patient would not have wished disclosed. The oath is not for easy days. It is for the hard ones.