Page 14 of 23
FM10.20 | Therapeutic Privilege, Misadventure & Professional Secrecy — SDL Guide
Learning Objectives
- Define and explain therapeutic privilege, describing its ethical basis and why it is largely rejected in modern bioethics
- Define malingering and distinguish it from factitious disorder and conversion disorder
- Define therapeutic misadventure and distinguish it from medical negligence
- Describe the principles governing professional secrecy and human experimentation ethics
INSTRUCTIONS
This module covers five legally and ethically significant concepts under FM10.20 that arise at the intersection of clinical practice, medical law, and research ethics. Each of these concepts — therapeutic privilege, malingering, therapeutic misadventure, professional secrecy, and human experimentation — presents a distinct type of challenge to the doctor: a situation where the appropriate action is not obvious, where professional duties may appear to conflict, or where legal and ethical considerations must be carefully distinguished. Accurate knowledge of these concepts is essential for the forensic medicine practitioner.
References
- KSN Reddy — Essentials of Forensic Medicine & Toxicology (textbook)
- BV Subrahmanyam — Modi's Medical Jurisprudence and Toxicology (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Three patients arrive at your hospital within the same hour. The first — a 65-year-old woman with terminal pancreatic cancer — is being treated by a colleague who has not told her the full prognosis, believing the truth would 'destroy her hope.' The second — a 30-year-old man — is claiming severe back pain after a minor road accident and demanding compensation from the transport company; his physical findings are inconsistent with his complaints. The third — a 50-year-old man — experienced a cardiac arrest while under anaesthesia for a routine hernia repair; the anaesthetist followed all protocols correctly but the patient did not survive. These three cases involve three different ethical and legal categories: the first is a case of potential therapeutic privilege; the second is a case of possible malingering; the third is a case of therapeutic misadventure. None of these is simple, and each requires precise conceptual clarity to handle correctly — both clinically and legally.
WHY THIS MATTERS
The five concepts in this module represent the grey zones of medical practice — situations where the right action is contested, where the law is specific, and where imprecise language can result in serious professional and legal consequences. A doctor who confuses therapeutic misadventure with negligence may either unfairly implicate a colleague in a legal proceeding or fail to recognise a genuine case of negligence that requires reporting. A doctor who invokes therapeutic privilege as a routine justification for withholding information will routinely violate patients' autonomy in a manner that is no longer ethically or legally defensible. A doctor who cannot distinguish malingering from conversion disorder may cause direct harm to a patient whose symptoms are neurological, not feigned. Precision in these areas is not pedantry — it is clinical and legal safety.
RECALL
Before we begin:
- From me2 (Bioethics), you know the four principles. Therapeutic privilege creates a tension between two of them — which two? And which principle has priority in modern ethical frameworks?
- From me5 (Rights and Duties), you know that professional secrecy is not absolute and has defined exceptions. Can you name three of those exceptions?
- What is the legal significance of the distinction between medical negligence and therapeutic misadventure? Why would it matter to a doctor, to a patient's family, and to a court?
Legal and Professional Context: Complex Ethical Territories in Practice
The five concepts covered in this module occupy a space where clinical practice, medical ethics, and law intersect in non-obvious ways. Each concept involves a situation where a simplistic application of rules would produce either an unjust or a professionally harmful outcome. Understanding the precise definition, ethical status, and legal consequences of each is part of the forensic medicine practitioner's core competency.
From a legal standpoint, these concepts are significant because:
- Therapeutic privilege — if invoked incorrectly — can constitute a violation of patient autonomy and form the basis of a complaint under the Consumer Protection Act 2019 or the NMC Code
- Malingering — if alleged without adequate evidence — can expose the doctor to claims of defamation (IPC 499) and professional misconduct; conversely, failing to identify genuine malingering in a compensation context may harm third parties
- Therapeutic misadventure — if misclassified as negligence — can result in unjust legal proceedings against a practitioner who acted correctly; if misclassified as misadventure when negligence was present — can deny a victim their legal remedy
- Professional secrecy and human experimentation have direct statutory frameworks that impose obligations and constraints that cannot be ignored
The overarching principle connecting all five concepts is that the doctor's duty of care — to the patient, to society, and to the integrity of the profession — requires the ability to reason precisely about complex situations rather than to apply rules mechanically. This module provides the conceptual vocabulary for that precision.
Therapeutic Privilege: Scope, Limits and Ethical Status
Therapeutic privilege (sometimes called 'therapeutic exception') refers to a doctor's claimed right to withhold material information from a patient on the grounds that disclosure would be harmful to the patient — for example, that telling a patient their diagnosis of terminal cancer would cause severe psychological distress that would compromise their remaining quality of life.
Historically, therapeutic privilege was widely invoked as a justification for medical paternalism. The reasoning was: 'I know what is best for this patient; full disclosure would harm them; therefore I am justified in withholding the information.' This reasoning reflects the beneficence-dominated model of medicine that prevailed before the modern emphasis on patient autonomy.
In contemporary medical ethics, therapeutic privilege is largely rejected as a general justification for non-disclosure. The reasons are clear:
1. Withholding diagnosis or prognosis prevents the patient from making informed decisions about their life — about treatment choices, about family arrangements, about their remaining time. The harm of the withholding (loss of autonomous choice, betrayal of trust) frequently outweighs the harm of disclosure.
2. The assessment that 'disclosure would harm the patient' is typically made by the doctor without asking the patient what they actually want. This is paternalistic and substitutes the doctor's judgment for the patient's own expressed preferences.
3. Modern evidence on truth-telling in cancer and terminal illness consistently shows that patients generally want accurate information and that withholding it causes additional psychological harm when patients discover the truth has been kept from them.
When therapeutic privilege may be legitimately invoked (narrow circumstances):
- When there is genuine reason to believe that disclosure would cause immediate, severe psychological decompensation (e.g. a patient with severe, currently uncontrolled psychiatric illness)
- As a temporary deferral — 'we'll discuss the full details when you feel stronger' — not as permanent concealment
- Therapeutic privilege is NOT legitimate when invoked for the doctor's convenience, the family's preferences (over the patient's), or because the doctor is uncomfortable delivering bad news
The legal position in India: The right to informed consent in Indian law (as interpreted through the Consumer Protection Act 2019 and case law) places a strong obligation on the doctor to disclose material information. The 'therapeutic privilege' defence is not codified in Indian statute and is viewed sceptically by consumer courts. Routine invocation of therapeutic privilege as a reason for non-disclosure can constitute a deficiency of service.
| Concept | Definition | Legal/Ethical Status in India | Practical Implication for Doctors |
|---|---|---|---|
| Therapeutic privilege | Doctor withholds information claiming disclosure would harm patient | Largely rejected; not a statutory defence; viewed sceptically by Consumer Courts | Disclose fully; only defer in narrow, documented circumstances |
| Malingering | Conscious, voluntary feigning or exaggeration of symptoms for external gain | Medicolegally significant; must be documented carefully | Assess objectively; document discrepancies; avoid accusatory language |
| Therapeutic misadventure | Adverse outcome from correctly performed treatment; inherent risk materialised | Not negligence; must be distinguished from negligence clearly | Document procedure compliance; state risk had been disclosed |
| Professional secrecy | Duty of confidentiality for patient information | Ethical obligation; not absolute; defined exceptions exist | Apply exception criteria before any disclosure |
| Human experimentation | Research on human subjects | Governed by Nuremberg Code, Declaration of Helsinki, ICMR guidelines | Voluntary informed consent is the absolute requirement |
SELF-CHECK
Under contemporary bioethics and Indian medical law, which of the following is the MOST accurate statement about therapeutic privilege?
A. Therapeutic privilege is a well-established legal defence that protects doctors from liability when they withhold information in a patient's best interest
B. Therapeutic privilege is recognised as a legitimate exception to informed consent in the NMC Code of Medical Ethics 2002
C. Therapeutic privilege is largely rejected as a general justification for non-disclosure because it substitutes the doctor's judgment for the patient's right to make informed decisions
D. Therapeutic privilege applies whenever a patient's family requests that the patient not be told a serious diagnosis
Reveal Answer
Answer: C. Therapeutic privilege is largely rejected as a general justification for non-disclosure because it substitutes the doctor's judgment for the patient's right to make informed decisions
Therapeutic privilege is largely rejected in contemporary bioethics because it elevates the doctor's paternalistic assessment over the patient's autonomy and right to informed consent. In Indian law, it is not codified as a statutory defence and is viewed sceptically. The family's preferences are not a legitimate basis for invoking therapeutic privilege — the obligation runs to the patient, not the family. Option B is incorrect — the NMC Code does not recognise therapeutic privilege as an exception to informed consent.
Malingering: Definition, Detection and Medicolegal Significance
Malingering is the voluntary, conscious fabrication or exaggeration of physical or psychological symptoms for the purpose of obtaining an external secondary gain. The key characteristics are: the behaviour is conscious (the person is aware they are fabricating); it is voluntary (not compelled by neurological or psychological processes outside their control); and the motivation is external (financial compensation, avoiding military service, obtaining drugs, avoiding legal consequences, securing disability benefits).
Malingering must be distinguished from two related conditions that share superficial features but are fundamentally different:
Factitious Disorder (Munchausen syndrome): The patient consciously fabricates or induces symptoms, but the motivation is internal — to assume the sick role, to receive medical attention and care. There is no external material gain sought. The patient wants to be a patient. This is a recognised psychiatric diagnosis (DSM-5, ICD-11) and requires empathetic management, not accusation.
Conversion Disorder (Functional Neurological Symptom Disorder): The patient presents with genuine neurological symptoms (paralysis, sensory loss, movement disorders, non-epileptic seizures) that are not explained by neurological disease. The symptoms are unconscious — the patient is not deliberately fabricating. Conversion disorder is a legitimate psychiatric/neurological condition; it is not malingering and must not be treated as such. Misdiagnosis as malingering when conversion disorder is present causes direct patient harm.
IMPORTANT: The key differentiator is consciousness of fabrication and external gain for malingering; internal motivation/sick role for factitious disorder; and unconscious symptoms for conversion disorder.
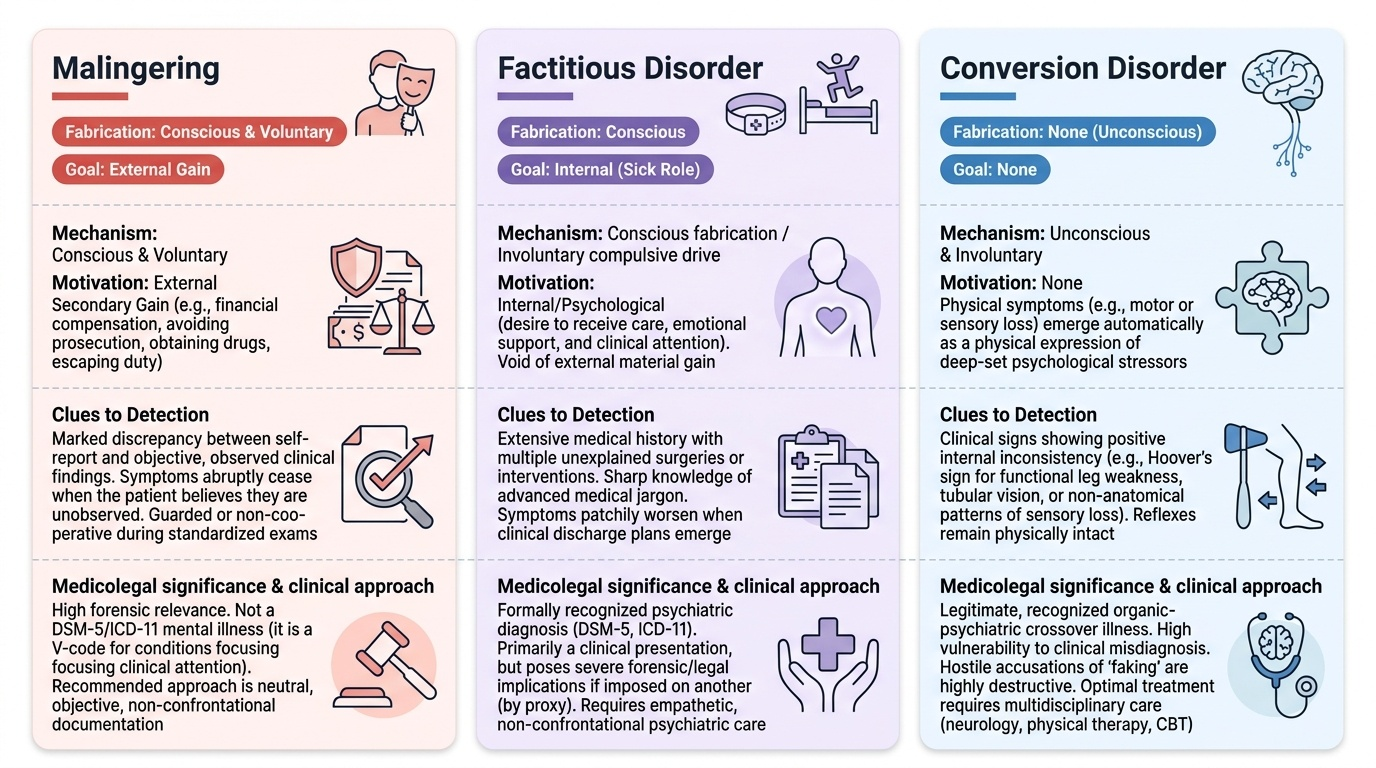
Provided image
Detection of malingering in clinical practice:
- Inconsistency between reported symptoms and objective findings
- Symptoms that vary with observation status (worse when observed, better when the patient believes they are unobserved)
- Inconsistency with the known natural history of the claimed condition
- Specific tests (Hoover sign, Waddell signs for back pain, specific neurological tests for conversion disorder)
- Collateral history from family and employers; review of medical records
Medicolegal significance: Malingering is most commonly encountered in compensation claims, military service evasion, and criminal proceedings. A doctor asked to assess a person for medicolegal purposes must:
- Document all objective findings carefully and specifically
- Note any inconsistencies between reported symptoms and objective findings
- Use careful, measured language — describe the objective findings, note the inconsistencies, and avoid labelling the person as a 'malingerer' in the report without establishing all the elements
- Be aware that a wrong diagnosis of malingering when factitious disorder or conversion disorder is present constitutes a failure of the doctor's duty of care