Page 14 of 20
FM14.{1,9} | Medico-legal Examination & Reporting of Injuries — SDL Guide (Part 2)
Writing the Medico-legal Certificate: Structure and Language
The medico-legal certificate for an injured person has a standard structure that is required by law and custom in Indian medical practice. Deviating from this structure — for example, by omitting the opinion section or failing to number injuries — reduces the document's utility and legal reliability.
The required sections of the MLC are:
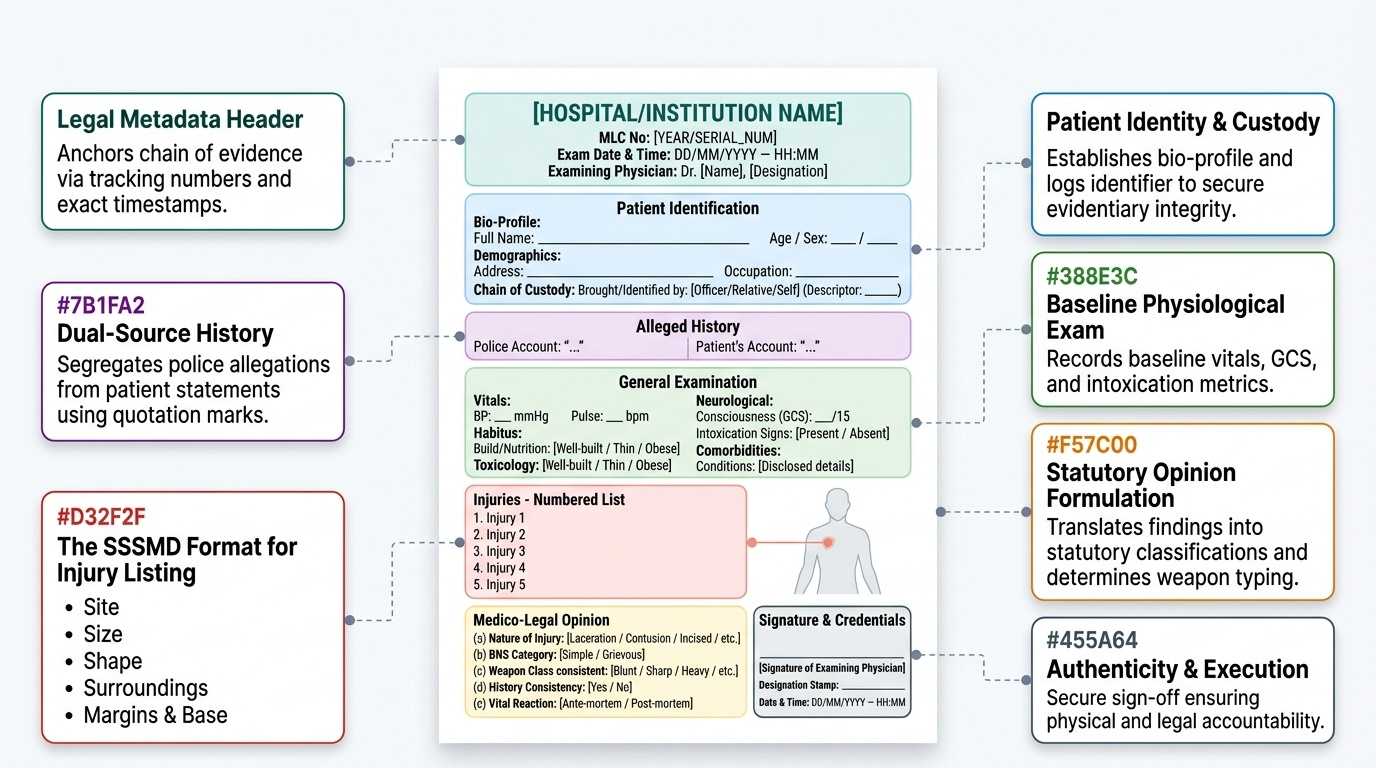
Header: hospital/institution name; MLC reference number; date, time, and place of examination; name and designation of the examining doctor.
Patient identification: full name, age, sex, address, occupation. Method of identification (brought by police/self/relative — describe the identifier).
Alleged history: recorded from the police version and separately from the patient's version where they differ. Use quotation marks or clearly attributed phrasing. This section records what is alleged, not what the doctor has verified.
General examination: vital signs (BP, pulse, temperature, respiratory rate), level of consciousness (GCS), nutritional/build status, any intoxication (alcohol smell, behaviour), relevant comorbidities if disclosed.
Injuries (numbered list): each injury is described separately with the SSSMD format:
- Site: exact anatomical location with distance from landmarks
- Size: length × width in centimetres (depth for stab wounds)
- Shape: geometric description (linear, oval, stellate, triangular)
- Surroundings: bruising, abrasion collar, soiling, clothing tear at injury site
- Margins and base: character of wound edges, presence/absence of tissue bridges, wound depth, base characteristics, and vital reaction (ante-mortem status)
Opinion: the medico-legal opinion section connects the findings to statutory and circumstantial categories. It should state: (a) nature of each injury (wound type); (b) BNS category (simple hurt, grievous hurt — specifying the sub-category); (c) weapon class consistent with the injuries; (d) whether the injuries are consistent with the alleged mechanism; (e) any finding of ante-mortem/post-mortem significance; (f) prognosis if relevant to BNS Category 8 certification.
Signature, designation, and date/time: the examining physician must sign the MLC personally. Countersignature or senior endorsement may be required by some institutions but does not transfer responsibility to the countersigner — the examining doctor retains primary liability for the content.
Provided image
SELF-CHECK
In the MLC, an injury is described as 'a wound on the left arm, approximately 3 cm, with clean edges.' What TWO critical pieces of information are missing from this description that would be required for a legally sound MLC?
A. The patient's occupation and the police station reference number
B. The exact anatomical site (distance from landmarks) and whether tissue bridges are present or absent (wound type characterisation)
C. The patient's blood group and X-ray results
D. The name of the weapon and the alleged assailant
Reveal Answer
Answer: B. The exact anatomical site (distance from landmarks) and whether tissue bridges are present or absent (wound type characterisation)
The description is inadequate in two critical respects: (a) the site is vague — 'left arm' is insufficient; the medico-legal standard requires distance from anatomical landmarks (e.g. '5 cm above the left elbow on the anterior aspect'); and (b) the wound type is not characterised — 'clean edges' suggests an incised wound (no tissue bridges), but this must be explicitly stated as 'no tissue bridges visible on examination' to distinguish it from a laceration. Without these two elements, the MLC cannot support a specific weapon-class opinion or a BNS injury category determination.
Applied MLC Practice: Integrating Findings into a Complete Report
In simulated or supervised clinical environments, the medico-legal examination skill requires integrating all prior knowledge into a coherent clinical document. Consider the following worked case, which integrates findings from the opening scenario:
Case: Female, 19 years, brought by police at 02:15 hours. Police version: alleged assault by partner at home with hands and a wooden stick.
General examination: conscious, oriented, GCS 15/15, BP 110/70, pulse 88/min, no alcohol smell, visibly distressed.
Injuries found on systematic head-to-toe examination:
- Laceration, right eyebrow: site — right eyebrow, lateral third, 0.5 cm from lateral canthus. Size — 2 cm × 0.3 cm × 0.2 cm depth. Shape — linear. Surroundings — bruising extending 1.5 cm around wound. Margins — irregular, tissue bridges present at wound base. Ante-mortem: active bleeding, vital reaction present.
- Abrasion, left cheek: site — left cheek, 3 cm below the left orbit. Size — 2 cm × 1 cm. Shape — irregular. Surroundings — mild surrounding redness. Margins — surface skin disruption, no gap, no deep haemorrhage. Ante-mortem: vital reaction present.
- Contusion, right forearm: site — right forearm, posterior aspect, 8 cm above the right wrist. Size — 3 cm × 2 cm. Shape — oval. Surroundings — nil. Skin intact, subcutaneous haemorrhage, purplish discolouration. Ante-mortem.
- Contusion, left forearm: site — left forearm, posterior aspect, 6 cm above the left wrist. Size — 4 cm × 2 cm. Shape — oval. Ante-mortem.
Opinion: 1. Laceration right eyebrow — blunt force injury, simple hurt (BNS S115); consistent with blunt cylindrical weapon. 2. Abrasion left cheek — blunt force/friction injury, simple hurt (BNS S115). 3 & 4. Bilateral posterior forearm contusions — blunt force injuries; the bilateral posterior forearm location is consistent with defence wounds sustained while raising both forearms to ward off blows with a blunt weapon. This pattern is consistent with the alleged homicidal assault.
This integrated opinion demonstrates the application of wound type classification, BNS categorisation, and circumstantial injury pattern interpretation in a single MLC document. The defence wound finding is a significant additional observation that corroborates the victim's account and informs the police investigation.
SELF-CHECK
A patient presents with a stab wound to the left chest, 2 cm surface entry, 8 cm deep, tracking into the pleural cavity with haemothorax. Applying the BNS framework, what is the MOST appropriate statutory category and what is the basis for this classification?
A. Simple hurt (BNS S115) — depth alone does not determine category
B. Grievous hurt, BNS S118 Category 7 (fracture of bone) — rib fractures are common in stab wounds
C. Grievous hurt, BNS S118 Category 8 (endangers life) — the stab wound has penetrated the pleural cavity causing haemothorax, which endangers life
D. Culpable homicide (BNS S100) — all penetrating chest wounds constitute culpable homicide
Reveal Answer
Answer: C. Grievous hurt, BNS S118 Category 8 (endangers life) — the stab wound has penetrated the pleural cavity causing haemothorax, which endangers life
A stab wound penetrating the pleural cavity and causing haemothorax endangers life — meeting the first criterion of BNS S118 Category 8 ('any hurt which endangers life'). The physician should document the basis: penetrating thoracic injury with haemothorax confirmed on examination/imaging, which without intervention is life-threatening. Category 7 (fracture) requires an actual confirmed fracture — not assumed. Category 8 based on 'endangers life' is the correct provision here. Culpable homicide (S100) requires causing death — the patient is alive, so this is premature and incorrect.