Page 11 of 20
FM5.6,FM14.10 | Weapons of Medico-legal Importance — SDL Guide (Part 2)
Weapon Examination: Method, Documentation, and Chain of Custody
When a weapon is submitted to the forensic physician as a medico-legal exhibit, it must be examined with the same systematic rigour as a clinical specimen, and the chain of custody must be strictly maintained. A weapon that has passed through multiple hands without documented continuity cannot be admitted as reliable evidence in court.
The systematic weapon examination follows a standardised protocol covering:
Identification and labelling: the weapon should arrive sealed in a tamper-evident container with a label showing case number, description, date and time of seizure, and the name of the officer who seized it. This label is the beginning of the chain-of-custody record. The forensic physician should note whether the seal is intact before opening and document any breach.
Type and general description: state the type of weapon (sharp-edged, sharp-pointed, blunt), its general category (knife, axe, lathi, etc.), and its condition (new, used, corroded, cleaned, damaged).
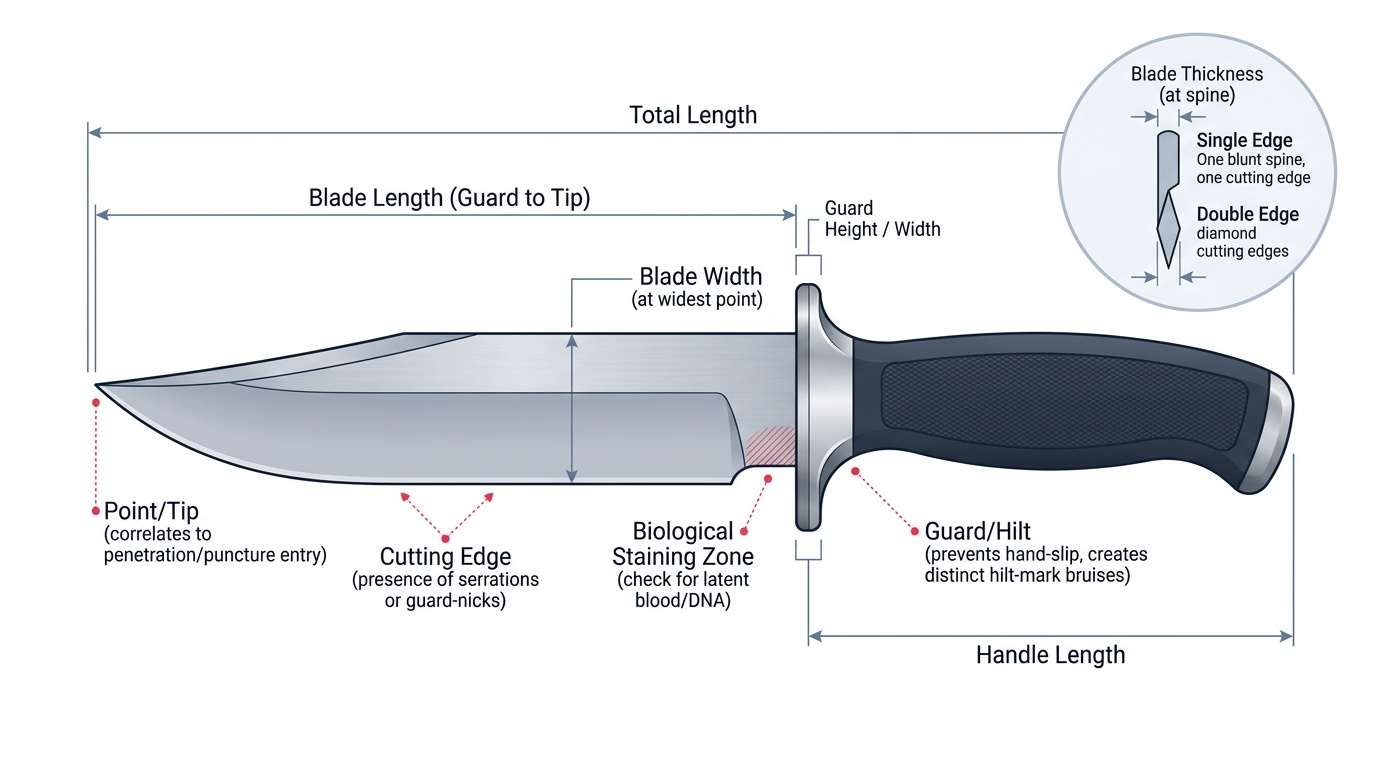
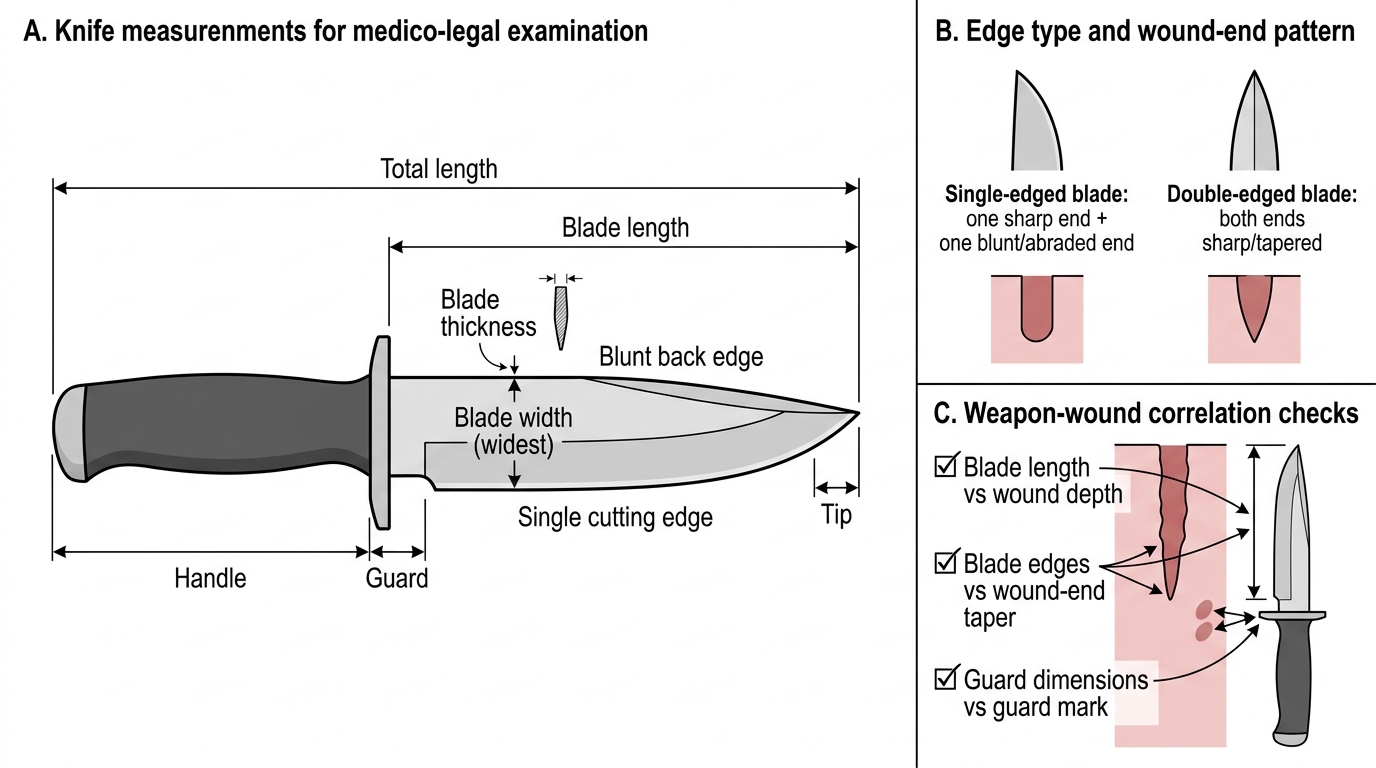
Measurements: total length; blade length (for sharp weapons) from guard to tip; blade width at widest point; blade thickness; handle length and material. These measurements are critical for correlating the weapon with wound dimensions (e.g. the blade length should equal or exceed the stab wound depth).
Blade/edge characteristics: sharpness of the edge and point; number of edges (single or double); presence of a grind bevel; serrations; nicks or damage to the edge; curvature of the blade. These features determine the wound geometry the weapon is capable of producing.
Biological staining: presence, distribution, colour, and estimated age (fresh vs dried) of blood or tissue staining on the blade, handle, or guard. Do NOT clean or wipe the weapon — biological material is preserved for DNA analysis and blood group serology. Document the staining before any sampling.
Other markings: serial numbers, manufacturer's marks, inscriptions, and any distinctive identifying features that may link the weapon to a specific source or owner.
Repackaging and chain of custody: after examination, the weapon is re-sealed, relabelled (noting the forensic physician's name, examination date, and case number), and returned to the police or submitted to the forensic science laboratory with the weapon report.
Provided image
The weapon-to-wound correlation is the centrepiece of the examination. For a knife stab wound, the physician checks: does the blade length match or exceed the wound depth? Does the number of blade edges (single vs double) match the taper pattern of the wound ends? Does any guard mark at the wound perimeter match the hilt dimensions of the submitted weapon? Each of these three checks either corroborates or contradicts the submitted weapon as the causative instrument.
Medico-Legal Measurements of a Knife
SELF-CHECK
A knife is submitted as a medico-legal exhibit. The victim has a stab wound 3 cm long on the skin surface with one tapered end and one squared end, and 7 cm deep tracking into the lung. The submitted knife has a blade length of 5 cm. What is the MOST accurate medico-legal observation about the weapon-wound connection?
A. The weapon is consistent with the wound — blade length 5 cm is sufficient to cause the wound
B. The weapon CANNOT be the weapon that caused the wound because the blade (5 cm) is shorter than the wound depth (7 cm)
C. The wound depth and blade length are unrelated in forensic analysis
D. A 5 cm blade can cause a 7 cm deep wound if the blow also compresses the chest wall
Reveal Answer
Answer: D. A 5 cm blade can cause a 7 cm deep wound if the blow also compresses the chest wall
Option D is correct and is a genuine forensic point: compressibility of soft tissue during a stab means the effective depth of penetration can exceed the blade length. When the chest wall is compressed at the moment of impact, the blade can penetrate further than its physical length. This is documented in Reddy's and Modi's and is an important medico-legal principle that prevents the erroneous conclusion that a weapon cannot have caused a wound because the apparent wound depth exceeds the blade length. The medico-legal opinion should note this possibility rather than stating the weapon cannot be the cause.
Weapon Report: Connecting Weapon to Wound in the Medico-legal Opinion
The weapon report is the formal document connecting the forensic physician's weapon examination findings to the injury findings from the MLC or post-mortem report. It is structured, objecttive, and follows the same principles of calibrated language as all medico-legal opinions.
A complete weapon report contains the following components:
Preamble: case reference number, date and place of examination, names of police officer and institution submitting the exhibit, and the forensic physician's identity and designation.
Description of weapon: a systematic description following the examination protocol above (type, dimensions, blade characteristics, biological staining, identifying marks).
Injury description (summary): a brief reference to the injuries documented in the MLC or post-mortem report that are being correlated with this weapon.
Opinion on weapon-wound connection: this is the central section of the weapon report. The opinion must address:
1. Whether the weapon is capable of producing the described wound type (e.g. 'a single-edged knife of these dimensions is capable of producing a stab wound with the described dimensions and wound geometry').
2. Whether the wound characteristics are consistent with production by this specific weapon (dimensions, blade geometry, guard mark correlation).
3. Whether the biological material on the weapon is consistent with the victim (pending laboratory serology and DNA results).
4. Any negative findings that would make the weapon an unlikely candidate for causing the described injuries (e.g. a blade too short to reach the depth of injury without tissue compression).
Standard language: 'In my opinion, the wound described [wound details] is CONSISTENT WITH being caused by the submitted weapon [weapon description], provided the wound depth discrepancy is accounted for by tissue compression at the time of impact. The biological staining on the blade is consistent with blood and awaits laboratory confirmation.' Never state 'this weapon caused the wound' — state 'this weapon is consistent with having caused the wound, subject to laboratory confirmation.'
The weapon report is an expert document that will be read in court, cross-examined upon, and may be challenged by defence experts. Precision of description, calibrated language, and strict objectivity are essential.
SELF-CHECK
You are writing the weapon report for a gandasa submitted in a homicide case. The victim has a chop wound on the left parietal region with bone notching of the skull. Which statement is the MOST appropriate for the opinion section of the weapon report?
A. The gandasa is the murder weapon that caused the death of the deceased
B. The chop wound with bone notching is consistent with being caused by a heavy sharp weapon such as the submitted gandasa; laboratory examination of the biological staining is recommended
C. The wound is consistent with being caused by a blunt weapon only — not a gandasa
D. No opinion can be given without laboratory confirmation of blood group
Reveal Answer
Answer: B. The chop wound with bone notching is consistent with being caused by a heavy sharp weapon such as the submitted gandasa; laboratory examination of the biological staining is recommended
Option B correctly uses calibrated language: 'consistent with' connects the wound type (chop wound with bone notching, characteristic of a heavy sharp weapon) to the weapon class and the specific submitted exhibit, and appropriately calls for laboratory confirmation of the biological staining rather than stating a conclusion that exceeds what the physical examination alone supports. Option A states a causal conclusion that belongs to the court, not the forensic examiner. Option C is wrong — a gandasa is a heavy sharp weapon that produces chop wounds, not purely blunt injuries. Option D incorrectly withholds the opinion that can be given from physical examination.