Page 8 of 20
FM5.4-5 | Wound Healing, Examination & Certification — SDL Guide (Part 2)
Factors Influencing Wound Infliction and Healing
The ease with which a wound is inflicted and the rate at which it heals are not constant across individuals or circumstances. A comprehensive understanding of these modifying factors is important both for accurate medico-legal certification (explaining unusual healing outcomes) and for addressing negligence claims (where failure to manage a known inhibitory factor may be cited as contributory).
The factors can be grouped into those relating to the wound itself and those relating to the host.
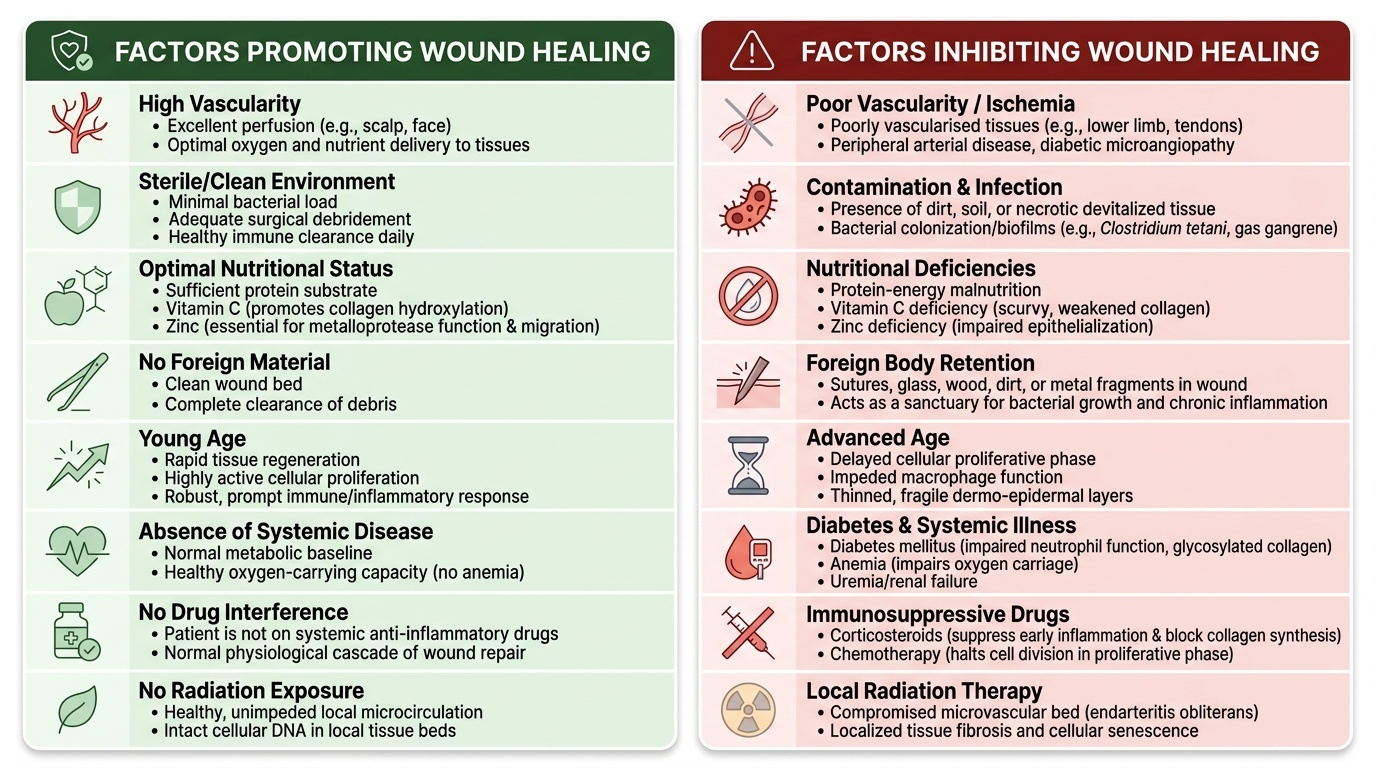
Wound-related factors influencing healing include: the nature of the wound (incised wounds with clean approximated edges heal faster than lacerations with irregular edges); degree of contamination (heavily contaminated wounds — soil, foreign bodies, devitalised tissue — heal slower and are prone to infection, including tetanus and gas gangrene); wound size and tissue loss (larger wounds with tissue deficit must heal by secondary intention, which is inherently slower); and adequacy of debridement (leaving devitalised tissue promotes infection and delays healing).
Host-related factors include: vascularity (wounds in highly vascular areas such as the scalp heal rapidly; wounds in poorly vascularised areas such as the lower leg and diabetic feet heal slowly); age (elderly patients show reduced proliferative capacity and immune response, leading to delayed healing); nutritional status (vitamin C deficiency impairs collagen hydroxylation; zinc deficiency impairs metalloprotease function and epithelial migration; protein deficiency reduces available substrate for repair); systemic disease (diabetes mellitus causes microvascular disease, impaired neutrophil function, and glycosylated collagen — a major healing inhibitor; anaemia reduces oxygen delivery to healing tissue); and medications (corticosteroids suppress inflammation and collagen synthesis; immunosuppressants impair the proliferative phase).
Provided image
CLINICAL PEARL
In medico-legal cases involving delayed wound healing or unexpected complications, the presence of an underlying modifying factor (diabetes, malnutrition, alcoholism, corticosteroid use) does not eliminate the causal link between the initial wound and the eventual outcome — it is an egg-shell skull rule situation in criminal law (the tortfeasor/assailant takes the victim as they find them). However, in cases involving medical negligence, a doctor's failure to identify and address a known healing-inhibiting factor — such as not checking blood glucose in a slow-healing wound, or failing to provide tetanus prophylaxis to a contaminated wound in an unvaccinated patient — can constitute contributory negligence. Document these factors in the MLC.
Wound as Cause of Death: Primary and Secondary Causes
When a wound results in death, the forensic physician must establish and document the causal chain connecting the wound to the death. The distinction between primary (direct) causes and secondary (indirect/remote) causes of death following a wound is fundamental to the medico-legal certificate and the death certificate.
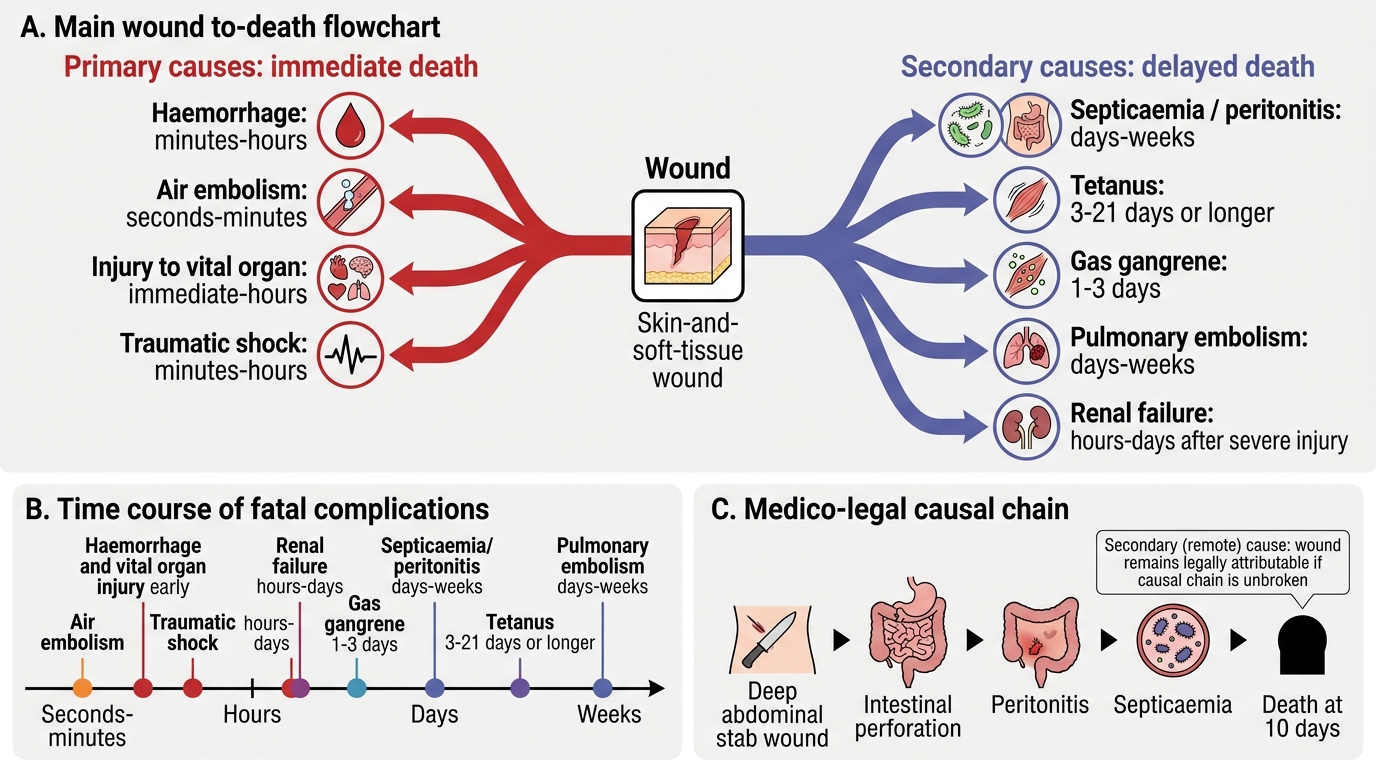
Primary (immediate) causes of death are those that cause death directly and rapidly, as a direct consequence of the wound itself, typically within minutes to hours. They include:
- Haemorrhage: either external (exsanguination from major vessel injury) or internal (haemothorax, haemoperitoneum, intracerebral haemorrhage). Fatal haemorrhage typically requires rapid loss of more than 40% of circulating blood volume (approximately 2 litres in an adult). The rate of blood loss, not just the volume, determines fatality — a slow bleed may be compensated while a rapid haemorrhage of the same volume is fatal.
- Injury to a vital organ: direct destruction of or haemorrhage into the brain, heart, or major vessels producing immediate incapacitation and death.
- Air embolism: entry of air into large veins (particularly the neck veins or during thoracic injuries) producing fatal embolic cardiac arrest.
- Traumatic shock: failure of circulation due to combined haemorrhage, neurogenic shock, and cardiorespiratory failure in severe polytrauma.
Secondary (remote) causes of death are complications that arise in the days to weeks after the initial wound due to the body's inadequate response to injury or to superadded infection. They include:
- Septicaemia and peritonitis: bacteria entering through the wound site or through bowel perforation spread systemically, causing septic shock; a major cause of death in untreated or inadequately treated wounds.
- Tetanus: Clostridium tetani infection in contaminated wounds (soil-contaminated, deep puncture wounds) — the toxin tetanospasmin blocks inhibitory neurotransmitter release, causing the classic trismus, opisthotonus, and autonomic instability seen in the case above; death results from respiratory muscle spasm or autonomic crisis.
- Gas gangrene (Clostridial myonecrosis): Clostridium perfringens and related species proliferate in devitalised, anaerobic tissue, producing gas and toxins causing systemic toxaemia and multiorgan failure.
- Pulmonary embolism: venous thromboembolism arising from DVT secondary to immobility during recovery — a particularly important cause of delayed death in lower limb trauma.
- Renal failure: acute tubular necrosis from shock, myoglobinuria from crush injury, or direct renal trauma.
Wound-to-Death Pathways
SELF-CHECK
A patient dies 10 days after sustaining a deep stab wound to the abdomen. Post-mortem findings show intestinal perforation with peritonitis and septicaemia. Which category of cause of death applies, and what is its medico-legal significance?
A. Primary cause of death — the wound directly caused death at the time of injury
B. Secondary (remote) cause of death — septicaemia following the wound is a complication, but the wound remains the legally attributable cause of death
C. Independent cause of death — peritonitis is unrelated to the stab wound
D. Accidental cause of death — septicaemia is not foreseeable from a stab wound
Reveal Answer
Answer: B. Secondary (remote) cause of death — septicaemia following the wound is a complication, but the wound remains the legally attributable cause of death
Septicaemia and peritonitis following an abdominal stab wound are secondary (remote) causes of death — complications arising from the original wound through an unbroken causal chain. In law, the original wound (stab) remains the legally attributable cause of death provided there is no novus actus interveniens (new intervening act) breaking the chain. The fact that death occurred 10 days later and through an infective complication rather than direct haemorrhage does not relieve the perpetrator of legal responsibility for causing death.
Wound Certification: Framing the Medico-legal Opinion on Healing
The medico-legal opinion on a wound's healing trajectory and its causative role in the patient's outcome requires integrating the clinical findings with the established timelines described above. In practice, this opinion addresses three questions: how long has the wound been present (injury dating), what was the expected healing course, and did the wound cause or contribute to the patient's current condition or death.
Injury dating from healing state: When examining a wound in a living patient or at post-mortem, the degree of healing — haematoma, granulation tissue, fibroblast activity, scar maturation — is correlated with the established histological and gross timelines (Reddy's) to produce an estimated range. The opinion should state a range (e.g. 'the wound is estimated to be 3–7 days old based on the presence of moderate granulation tissue and early fibroblast activity') rather than a precise date, acknowledging that individual variation and healing-modifying factors affect the timeline.
Certification of wound nature for BNS purposes: The healing trajectory is directly relevant to whether an injury qualifies as grievous hurt under BNS Section 118 Category 8 (causing the patient to be unable to follow ordinary pursuits for 20+ days). If healing prognosis indicates recovery within this period, the injury is simple hurt; if the injury type, wound depth, and any complications indicate a longer recovery, Category 8 grievous hurt applies. This prognosis must be documented at the time of examination with its clinical basis, not added retrospectively.
Causation opinion in death cases: When a patient dies following a wound, the MLC or post-mortem report must trace the causal chain explicitly. The standard medico-legal formulation is: 'The deceased sustained [wound type] of [site]. The cause of death is [primary/secondary complication]. In my opinion, the [complication] is a direct/indirect consequence of the original wound, and but for the wound, the [complication] would not have occurred.' Any intervening events — inadequate treatment, patient non-compliance, pre-existing disease — should be noted as modifying factors but should not be stated as breaking the causal chain unless there is strong evidence of an independent causative event.
SELF-CHECK
A patient with an uncomplicated incised wound on the palm is examined 6 weeks later. The wound shows a pale, flat scar with no active inflammation. Under BNS Section 118, which category is most appropriate, and what clinical information would be needed to certify Category 8?
A. Grievous hurt Category 7 (fracture of bone) — applicable to all hand injuries
B. Simple hurt (BNS S115) — wound has healed; however, to certify Category 8 one would need documented evidence that the patient was unable to follow ordinary pursuits for ≥20 days
C. Grievous hurt Category 8 automatically — palm wounds always qualify as endangering life
D. Grievous hurt Category 5 (permanent impairing of a member) — palm wounds always impair hand function
Reveal Answer
Answer: B. Simple hurt (BNS S115) — wound has healed; however, to certify Category 8 one would need documented evidence that the patient was unable to follow ordinary pursuits for ≥20 days
A healed incised palm wound at 6 weeks does not automatically qualify as grievous hurt. To certify Category 8 (BNS S118), the physician must demonstrate that the injury caused inability to follow ordinary pursuits for 20 or more days — requiring documented evidence of functional impairment during that period (occupation, nature of work, date of return to work). Without this documentation, the injury is simple hurt. Category 7 requires a fracture/dislocation; Category 5 requires permanent impairment — neither applies to a healed wound with presumably restored function.