Page 6 of 18
FM10.19 | Consent in Medical Practice — SDL Guide (Part 2)
Rules of Consent — Special Situations
Several clinical situations require the application of specific legal rules that modify or substitute for ordinary patient consent. These are the areas most tested in FM examinations and most likely to arise in medico-legal practice.
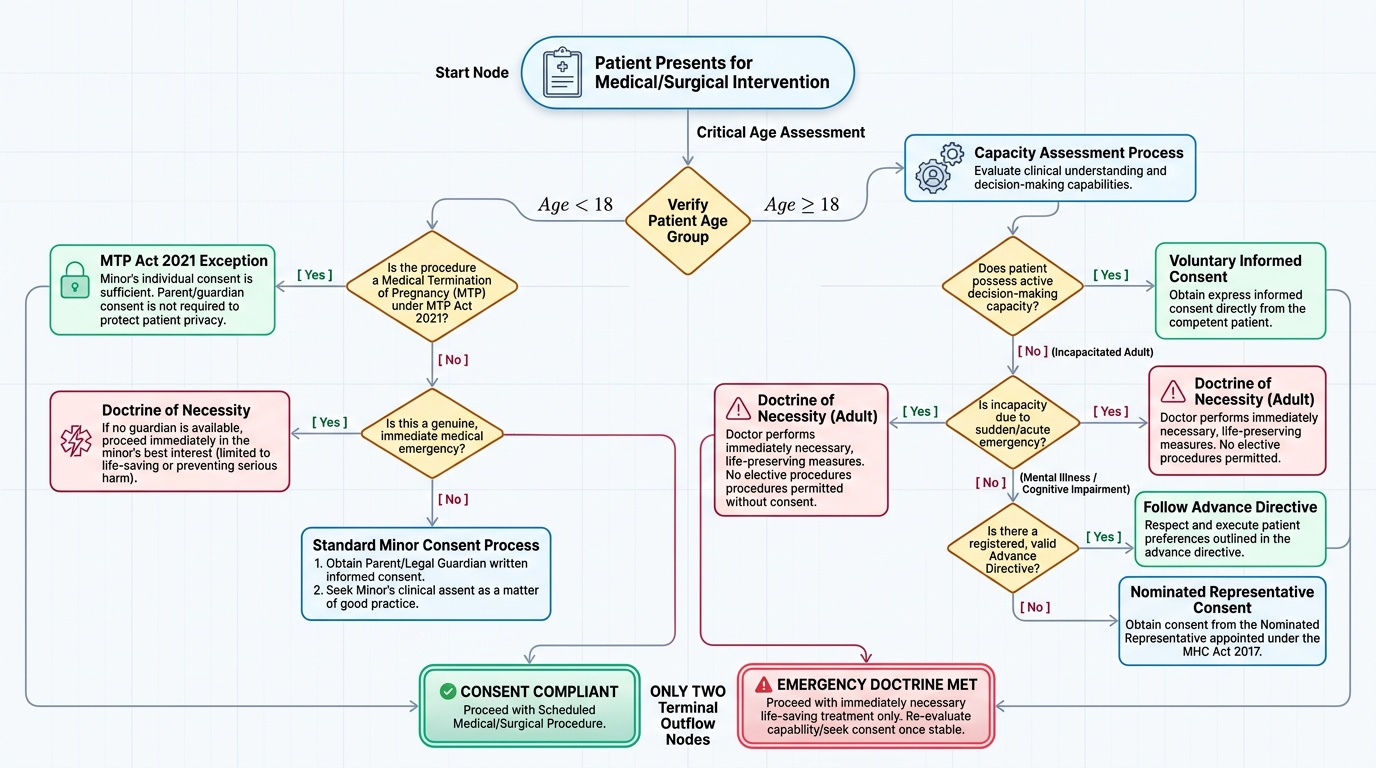
Age and consent:
- The age of majority in India is 18 years under the Indian Majority Act 1875. A person aged 18 and above has full legal capacity to consent to any medical procedure.
- For persons under 18 (minors), consent must ordinarily be obtained from the parent or legal guardian. The minor's own assent (agreement) should also be sought as a matter of good practice.
- MTP Act 2021 amendment exception: Under the amended MTP Act, a minor seeking termination of pregnancy does NOT require parental consent — the Act permits a registered medical practitioner to perform a termination on a minor without guardian consent, to protect the minor's privacy. This is a specific statutory carve-out from the general rule requiring guardian consent for minors.
- In emergencies affecting minors, if no guardian is available and immediate action is needed, the treating doctor may act in the minor's best interests under the doctrine of necessity.
Emergency exception:
In a genuine medical emergency, when the patient lacks capacity (unconscious, severely incapacitated) and no legally authorised substitute decision-maker is available and there is insufficient time to obtain consent, a doctor may proceed with treatment necessary to preserve life or prevent serious harm without prior consent. This is the doctrine of necessity. The exception is narrow: it applies only to measures immediately necessary; it does not permit elective or non-urgent procedures. Once the emergency is resolved, consent must be obtained for further treatment.
Mental illness:
Under the Mental Healthcare Act 2017 (MHC Act 2017, which replaced the Mental Health Act 1987), a person with mental illness retains decision-making capacity unless specifically assessed as lacking it. A psychiatric diagnosis alone does not negate consent capacity. The MHC Act 2017 introduced Advance Directives — a competent person with mental illness may specify in advance how they wish to be treated during a future episode of illness. If a person lacks capacity due to mental illness, the nominated representative (as appointed under the MHC Act) or a family member may provide consent. Involuntary admission and treatment are permitted only under strict procedural safeguards set out in the Act.
Alcohol intoxication:
A patient who is severely intoxicated with alcohol may lack the capacity to give or withhold consent due to impaired comprehension and judgment. The same rules as for incapacity apply: if the situation is an emergency, proceed under the doctrine of necessity; if non-urgent, defer the procedure until the patient regains capacity. Consent obtained from an acutely intoxicated individual may be challenged as invalid on the grounds of impaired capacity at the time of signing.
Provided image
CLINICAL PEARL
The MTP Act 2021 amendment and minor consent: This is a frequently examined, high-stakes fact. The 2021 amendment to the MTP Act extended the gestational limit to 24 weeks for specific categories of women (rape/incest survivors, foetal abnormalities, etc.) and, critically, removed the requirement for guardian consent for minors seeking a termination. A registered medical practitioner may terminate a minor's pregnancy without parental consent or notification. This protects the minor's reproductive autonomy and privacy. However, the minor should still be documented as having given her own expressed consent. Do NOT conflate this with the general rule — for all other medical procedures, a minor requires guardian consent.
Documentation of Consent and Applied Practice
The practical management of consent in a busy clinical setting requires systematic habits that simultaneously protect patient rights and create a defensible medico-legal record. The most significant errors in consent practice — which account for a large proportion of consumer complaints — arise not from ignorance of the law but from shortcuts taken under time pressure.
Consent form documentation standards:
- The form must be specific to the procedure (a generic 'I consent to any procedure the doctor recommends' is legally inadequate and may be unenforceable).
- It must be signed before premedication or sedation — a sedated patient lacks capacity.
- It should be witnessed by a third party, preferably a nurse or ward staff member.
- The form should record that risks, benefits, and alternatives were discussed — not merely that 'procedure was explained'.
- The physician obtaining consent should be the one performing (or leading the team performing) the procedure; delegating consent-taking to a junior without proper briefing of that junior is a common deficiency.
Capacity assessment: When doubt exists about a patient's capacity (cognitively impaired, confused, intoxicated), a formal capacity assessment should be conducted and documented. The four-component capacity test requires that the patient can: (a) understand the information given, (b) retain it long enough to make a decision, (c) weigh the pros and cons, and (d) communicate the decision.
Withdrawal of consent: A competent patient may withdraw consent at any time, including during a procedure (where stopping is clinically possible). The clinician must respect the withdrawal; completing a procedure against a withdrawn consent is battery, even if discontinuing mid-procedure carries some risk.
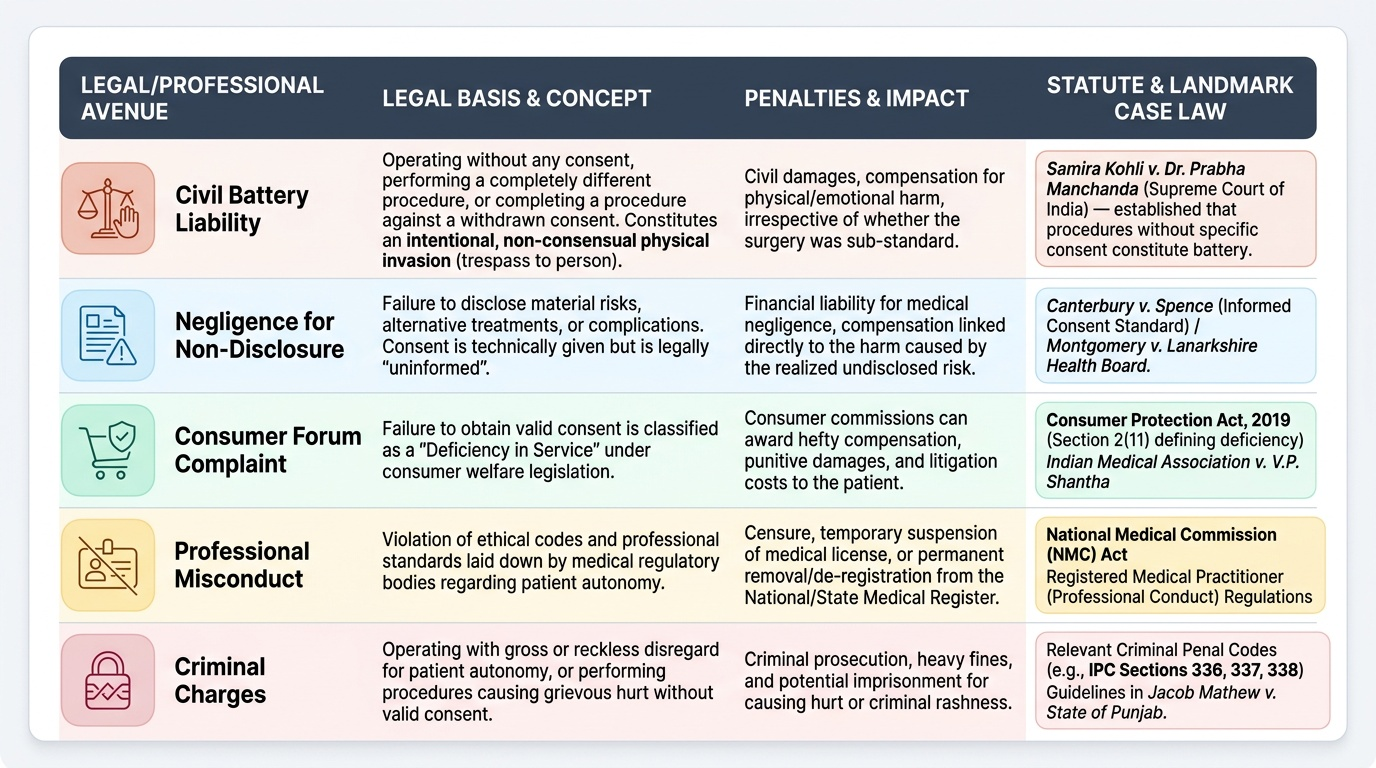
Consequences of operating without valid consent:
- Civil liability for battery (intentional unconsented touching)
- Negligence claim (failure to disclose material risks)
- Consumer forum complaint under CPA 2019
- Professional misconduct finding before the NMC or State Medical Council
- In extreme cases, criminal charges under IPC (assault, wrongful restraint)
Provided image
SELF-CHECK
A 19-year-old man with schizophrenia, currently stable on medication, is admitted for an elective hernia repair. His family insists he cannot consent and demands to sign on his behalf. Under the Mental Healthcare Act 2017, what is the CORRECT approach?
A. Accept the family's consent automatically because the patient has a psychiatric diagnosis
B. Proceed without consent under the emergency exception
C. Assess the patient's capacity — if he can understand, retain, weigh, and communicate his decision, his own consent is valid
D. Defer the surgery indefinitely until the patient has no psychiatric diagnosis
Reveal Answer
Answer: C. Assess the patient's capacity — if he can understand, retain, weigh, and communicate his decision, his own consent is valid
The Mental Healthcare Act 2017 affirms that having a mental illness does not automatically negate consent capacity. The correct approach is a formal capacity assessment. If the patient — despite having schizophrenia — can understand the proposed procedure, retain that information, weigh the pros and cons, and communicate his decision, his own consent is legally valid and should be obtained. A psychiatric diagnosis alone is an insufficient reason to override the patient's autonomy. Only if the capacity assessment finds him lacking capacity should a substitute decision-maker (nominated representative or family) be involved.