Page 11 of 18
FM10.11-12 | Euthanasia, DNR & Stem-Cell Ethics — SDL Guide
Learning Objectives
- Define euthanasia and classify it by act, consent, and medical method
- Distinguish active from passive euthanasia and physician-assisted suicide
- Explain the legal framework for passive euthanasia and Advance Directives in India following key Supreme Court rulings
- Define Do Not Resuscitate (DNR) orders — process, ethical basis, and documentation
- Describe the ethical and legal issues in stem cell research, including regulatory oversight in India
INSTRUCTIONS
The spectrum from life-sustaining treatment withdrawal to physician-assisted dying is one of the most ethically charged domains in medicine. India's Supreme Court rulings on passive euthanasia and Advance Directives have created binding legal precedent that every clinician must understand. Simultaneously, the rapid expansion of stem cell science has outpaced regulatory frameworks, and knowing the ethical guardrails is an NMC-mandated competency.
References
- KSN Reddy — Essentials of Forensic Medicine & Toxicology (textbook)
- BV Subrahmanyam — Modi's Medical Jurisprudence and Toxicology (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Aruna Shanbaug was a nurse at KEM Hospital, Mumbai who, in 1973, was sexually assaulted and strangled, leaving her in a persistent vegetative state (PVS). For 42 years, she was cared for by the hospital nursing staff. In 2011, journalist Pinki Virani filed a petition in the Supreme Court of India seeking permission to discontinue her artificial nutrition and hydration, citing euthanasia on grounds of dignity. The KEM Hospital nursing staff opposed the petition and argued they would continue to care for her.
The Supreme Court's ruling in Aruna Ramachandra Shanbaug v Union of India (2011) is a landmark in Indian medical law. What did the Court decide? What is the legal status of passive euthanasia in India today? And separately — when a patient with a terminal cancer diagnosis asks their physician about a Do Not Resuscitate order, what is the legal and ethical framework governing that conversation?
WHY THIS MATTERS
End-of-life decisions are among the most ethically and legally complex situations a clinician will face. India's legal framework has evolved substantially: passive euthanasia is now legally permissible under specific conditions following Aruna Shanbaug (2011) and Common Cause v Union of India (2018). Advance Directives ('living wills') are now legally recognised documents. At the same time, active euthanasia and physician-assisted suicide remain criminal offences in India. Every intensivist, oncologist, geriatrician, general physician, and family medicine practitioner will encounter patients for whom these decisions arise — and most will encounter these before subspecialty training is complete.
RECALL
Recall from ethics and law sessions:
- Autonomy — the right of a competent individual to make decisions about their own body, including the right to refuse treatment.
- Beneficence vs non-maleficence — acting in the patient's best interest vs avoiding harm; sometimes these principles conflict at end-of-life.
- Consent and capacity — covered in SDL ml3; applies to decisions about treatment withdrawal.
- IPC 302 — murder (intentional killing of another person).
- IPC 304 — culpable homicide not amounting to murder.
- IPC 309 — attempt to commit suicide; partially decriminalised by the Mental Healthcare Act 2017.
Euthanasia: Legal and Professional Context
Euthanasia — from the Greek eu (good) + thanatos (death) — refers to the intentional ending of a life to relieve suffering. The term encompasses a spectrum of acts that vary enormously in their ethical and legal status, and precision in classification is essential because conflating categories leads to profound legal errors.
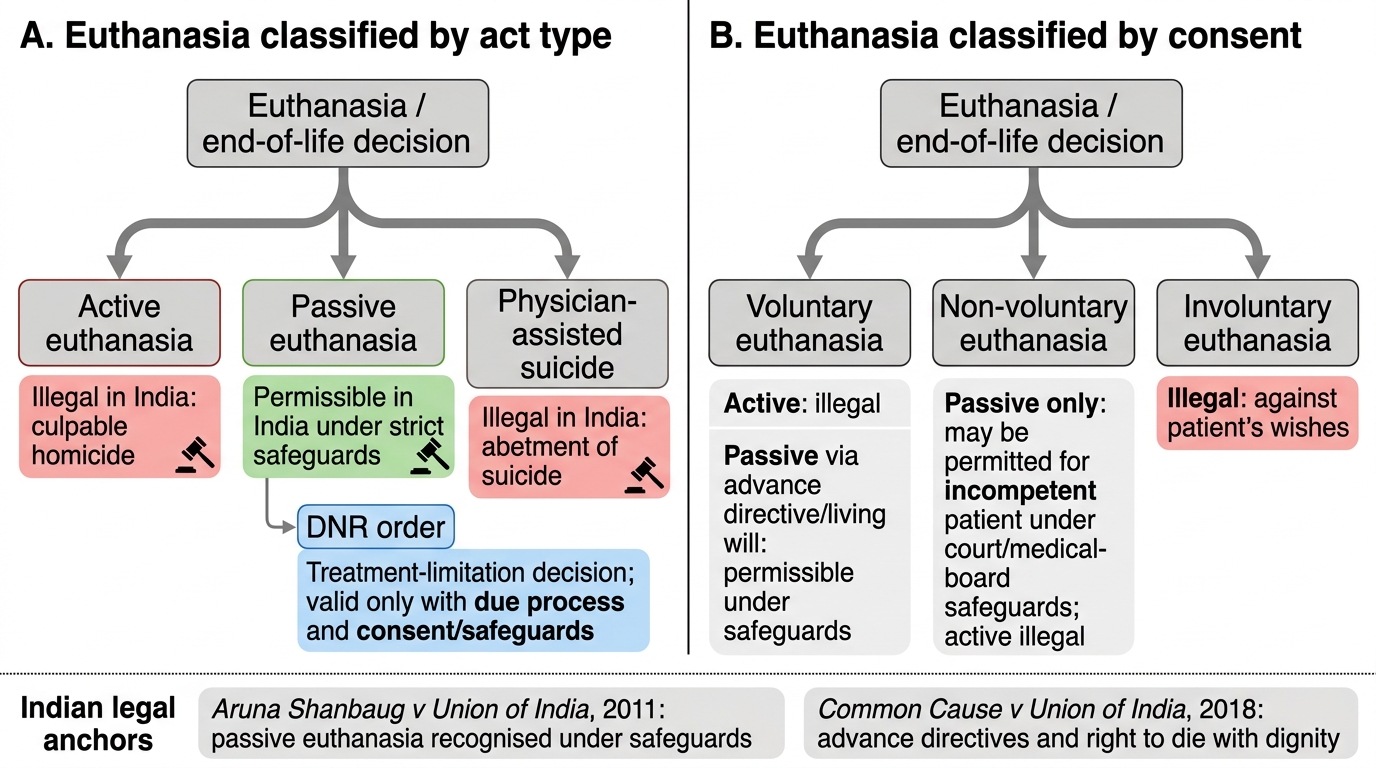
Classification of euthanasia:
By the actor's role (act vs omission):
- Active euthanasia: a positive act is taken to end the patient's life, such as administering a lethal injection. Active euthanasia is illegal in India and constitutes culpable homicide under the IPC, regardless of compassionate intent. It is illegal in most jurisdictions worldwide, with notable exceptions (Netherlands, Belgium, Canada).
- Passive euthanasia: withholding or withdrawing life-sustaining treatment, allowing the patient to die from the underlying disease. In India, passive euthanasia is legally permissible under specific conditions following the Supreme Court's rulings in Aruna Shanbaug v Union of India (2011) and Common Cause v Union of India (2018).
- Physician-assisted suicide (PAS): the physician provides the means (e.g., a lethal prescription) but the patient self-administers. PAS remains illegal in India.
By consent:
- Voluntary euthanasia: the patient explicitly requests or consents to the ending of their life.
- Non-voluntary euthanasia: the patient is unable to give consent (unconscious, PVS, infant) and the decision is made by others.
- Involuntary euthanasia: the patient is capable of consent but has not been asked or has expressed a wish to live; this is always illegal and constitutes murder.
Do Not Resuscitate (DNR) orders are a specific category of passive euthanasia — a decision, usually documented in advance, that cardiopulmonary resuscitation (CPR) will not be attempted if the patient suffers cardiac or respiratory arrest. DNR is NOT the same as euthanasia; it is a decision not to start a specific intervention (resuscitation) rather than a decision to actively end life. DNR orders are legally permissible in India when properly documented and consented.
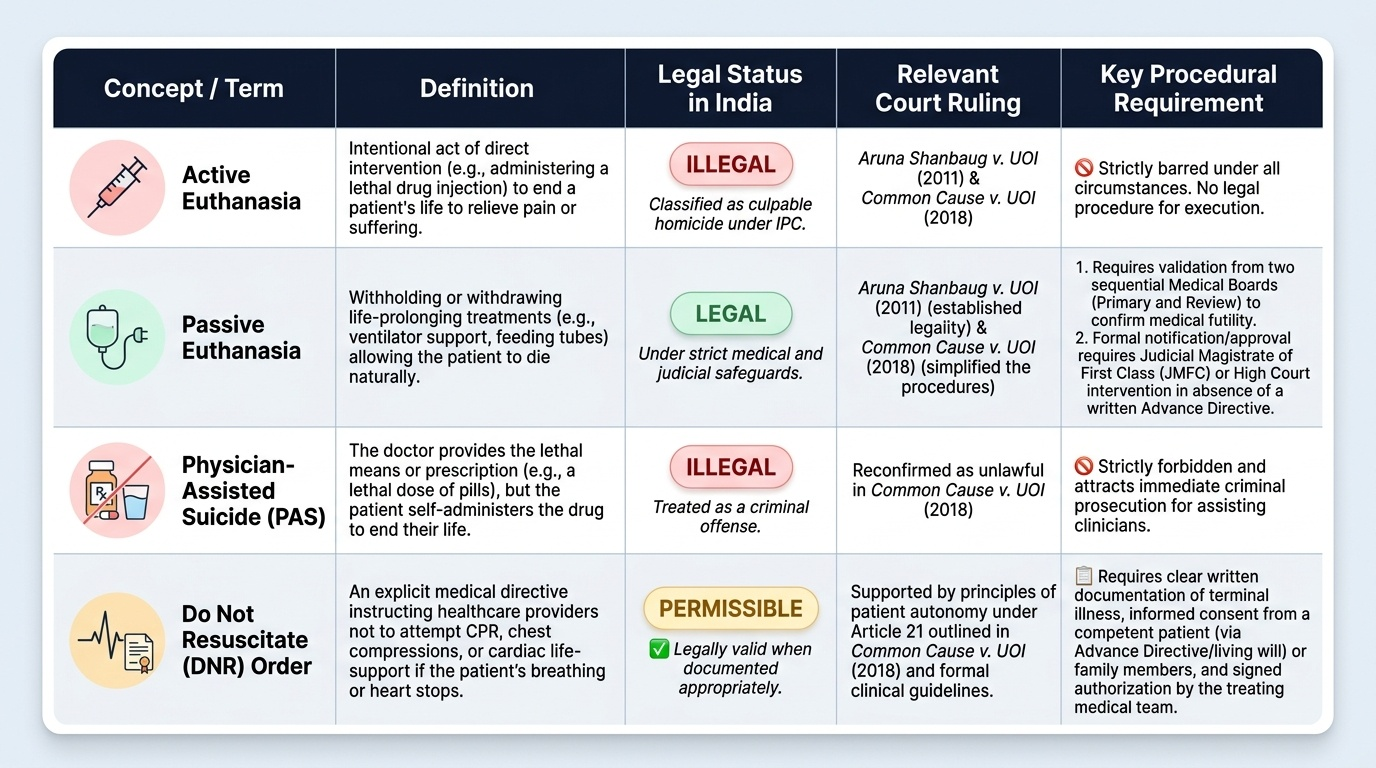
Classification of Euthanasia and Legal Status in India
Legal Framework: Governing Principles and Indian Precedents
The legal framework for end-of-life decisions in India has been established through two landmark Supreme Court rulings, both of which every clinician must know with precision.
Aruna Ramachandra Shanbaug v Union of India (2011):
In this case, the Supreme Court examined whether passive euthanasia could be permissible in a case of persistent vegetative state. The Court held:
1. Active euthanasia remains illegal in India and constitutes culpable homicide.
2. Passive euthanasia — withdrawal of life-sustaining treatment in patients in a permanent vegetative state or those with no hope of recovery — is permissible in India under strict procedural safeguards.
3. The decision for passive euthanasia in an incompetent patient must be made by the High Court (applying the parens patriae jurisdiction — the court's power to act as guardian for those unable to protect themselves) on the petition of close relatives or hospital staff, after consultation with a medical board.
4. In Aruna Shanbaug's own case, the Court declined to grant permission because the KEM nursing staff who cared for her expressed opposition to withdrawal.
Common Cause v Union of India (2018):
This landmark Constitution Bench (five judges) ruling went further and established:
1. Advance Directives ('living wills') are legally valid and binding in India. A competent adult may specify in advance that, in the event of a terminal illness or irreversible coma, they do not wish to be kept alive by artificial means.
2. The Court set out detailed procedural safeguards for executing, authenticating, and acting upon an Advance Directive.
3. Passive euthanasia through withdrawal of life support remains permissible for patients in a permanent vegetative state, now through a Medical Board and Judicial Magistrate process (simplified from the Aruna Shanbaug High Court route).
4. The right to die with dignity is a component of the fundamental right to life under Article 21 of the Constitution.
Current legal position in India:
- Active euthanasia: ILLEGAL — culpable homicide under IPC.
- Passive euthanasia: LEGAL under procedural safeguards (Medical Board + Judicial Magistrate or High Court).
- Physician-assisted suicide: ILLEGAL.
- Advance Directives: LEGALLY VALID under Common Cause (2018).
- DNR orders: LEGALLY PERMISSIBLE with proper documentation and consent.
Provided image
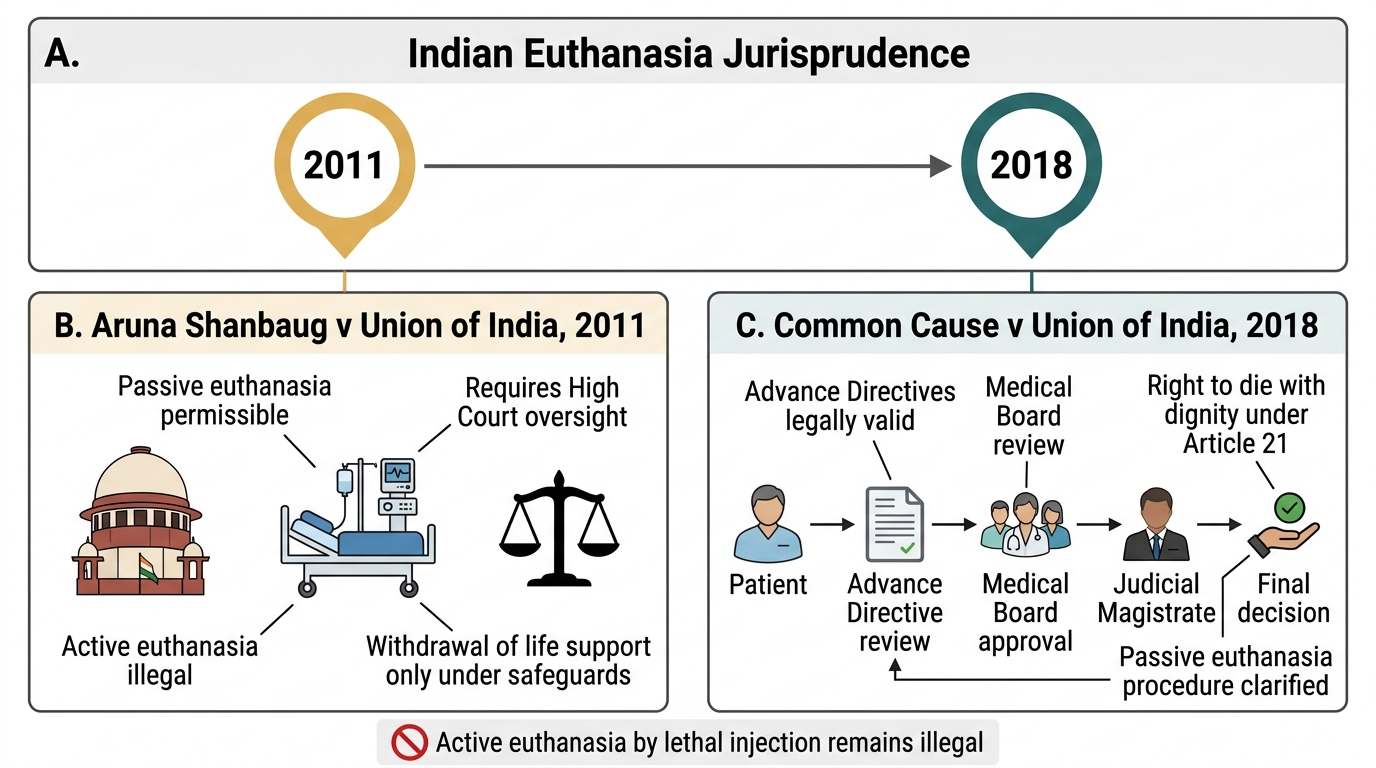
Indian Euthanasia Jurisprudence Timeline
SELF-CHECK
A 68-year-old man with end-stage metastatic lung cancer is in a permanent vegetative state on a ventilator. His family wishes to withdraw ventilator support. Under the Common Cause v Union of India (2018) ruling, what is the CORRECT procedural pathway?
A. The family's consent alone is sufficient to withdraw ventilation
B. A Medical Board review followed by approval from a Judicial Magistrate (or High Court if required)
C. The treating doctor may decide unilaterally based on clinical judgment
D. Active euthanasia by lethal injection, which is now legal under Common Cause 2018
Reveal Answer
Answer: B. A Medical Board review followed by approval from a Judicial Magistrate (or High Court if required)
Following Common Cause v Union of India (2018), passive euthanasia (withdrawal of life-sustaining treatment) for a patient in a permanent vegetative state is legally permissible in India through a specified procedure: review by an institutional Medical Board, followed by approval from a Judicial Magistrate. The family's consent is an important input but is NOT sufficient alone. Active euthanasia (lethal injection) remains illegal in India regardless of the family's wishes. The treating doctor cannot decide unilaterally without this safeguarded process.
DNR Orders: Method and Documentation
A Do Not Resuscitate (DNR) order — also termed a DNAR (Do Not Attempt Resuscitation) order or, in contemporary palliative care terminology, an AND (Allow Natural Death) order — is a prospective written medical instruction that specifies that cardiopulmonary resuscitation (CPR) should not be attempted in the event of cardiac or respiratory arrest. Understanding the distinction between DNR and euthanasia is critical: DNR is not about ending a patient's life; it is about not starting a specific intervention (resuscitation) when the clinical benefit of that intervention is judged to be nil or disproportionately harmful relative to its burdens.
Ethical basis of DNR:
CPR was originally designed for reversible sudden cardiac arrest in otherwise healthy or recoverable patients. In advanced terminal illness, irreversible organ failure, or permanent loss of consciousness, CPR may result in physical harm (fractured ribs, internal injuries), prolong the dying process, and deprive the patient of a peaceful death, without meaningfully altering the clinical trajectory. The ethical justification for a DNR order rests on: (a) patient autonomy — the right to refuse a specific treatment; (b) non-maleficence — avoiding futile and burdensome interventions; (c) clinical futility — the intervention cannot achieve its physiological goal.
Process of establishing a DNR order:
1. Clinical assessment: the attending physician makes a clinical judgment that CPR would either be futile (no chance of successful resuscitation) or disproportionately burdensome in the patient's specific context.
2. Competent patient conversation: if the patient is competent, the discussion of DNR must involve the patient; their autonomous decision to refuse CPR must be documented. Patient-initiated DNR requests are ethically unambiguous.
3. Family consultation for incompetent patients: when the patient lacks capacity, the family and the medical team discuss and reach a shared decision. A second senior clinician should be involved.
4. Documentation: the DNR order must be clearly documented in the medical notes — date, time, physician's name and signature, clinical basis for the order, who was consulted, and the patient's or family's understanding. It should be reviewed regularly.
5. Communication: all members of the care team — nurses, on-call doctors, paramedics — must be aware of and understand the DNR order.
Common misunderstandings about DNR:
- DNR does NOT mean withdrawal of all care — patients with DNR orders still receive full medical treatment for pain, infection, nutrition, and comfort.
- A DNR order for CPR does not automatically mean DNR for intubation, vasopressors, or other interventions — scope must be specified.
- A DNR order can be rescinded at any time by a competent patient who changes their mind.
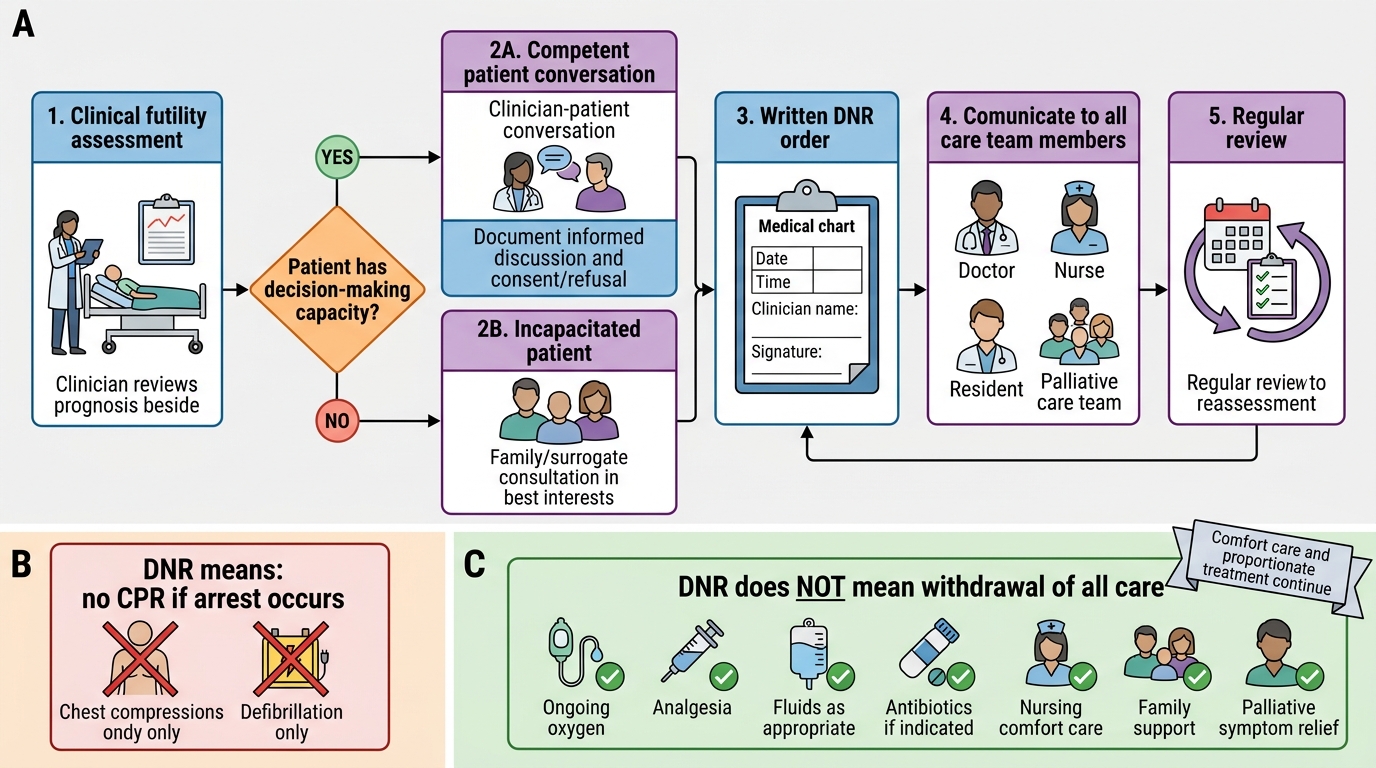
Establishing a DNR Order: Process and Scope
CLINICAL PEARL
Doctrine of double effect at end of life: The doctrine of double effect permits a clinician to administer a treatment — typically opioid analgesia or sedation for refractory symptom control in terminal illness — that has the foreseen but unintended side effect of hastening death, provided: (1) the act itself is not intrinsically wrong, (2) the bad effect (hastening death) is not the means by which the good effect (pain relief) is achieved, (3) the intention is the good effect only, and (4) there is proportionate reason. High-dose opioids for refractory cancer pain may meet these criteria and are legally and ethically permissible in palliative care. This is distinct from active euthanasia, where death is the intended endpoint.
Stem Cell Research: Applied Ethical Practice
Stem cell research involves the study and therapeutic application of pluripotent or multipotent cells capable of differentiating into multiple cell types. The ethical controversies in stem cell research arise primarily from the source of the cells, and India has developed specific regulatory guidance that students must know for FM10.12.
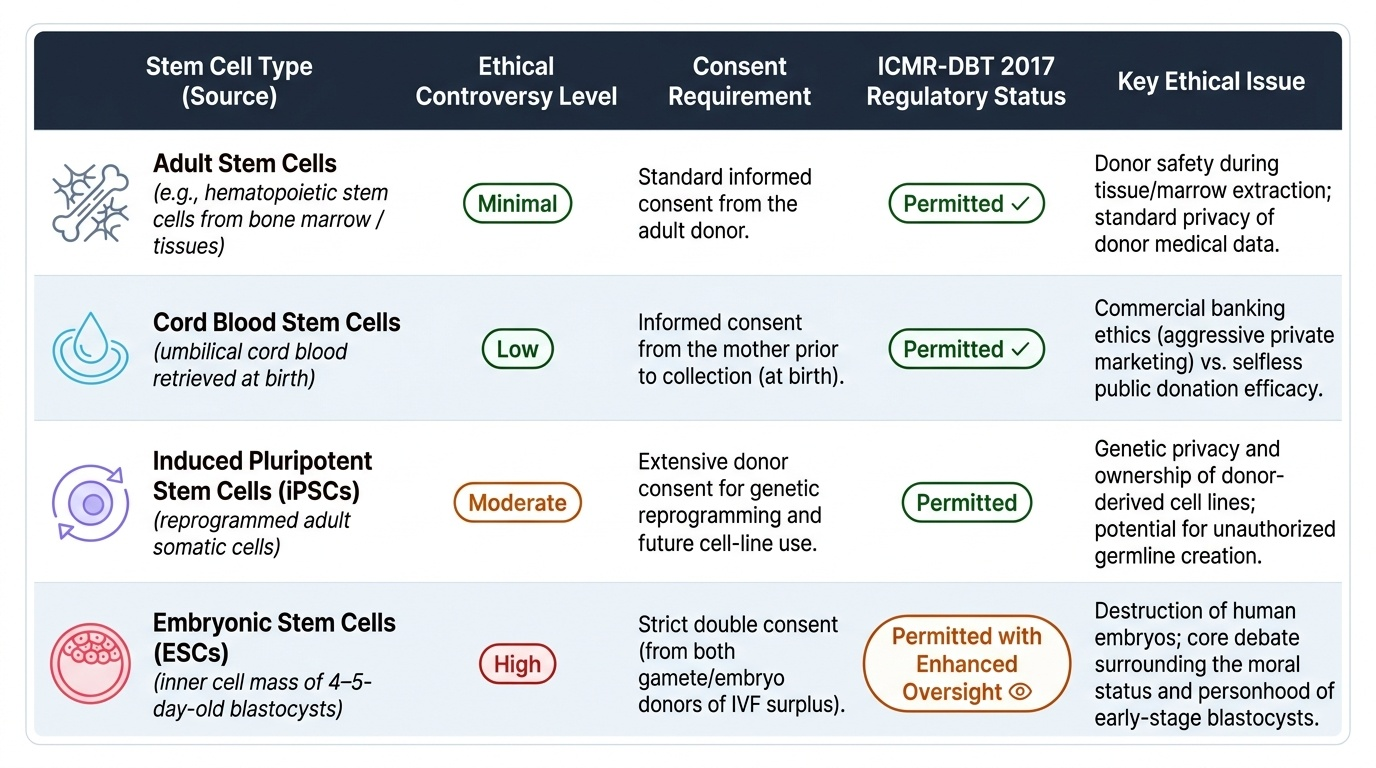
Classification of stem cells (by source — ethically relevant):
- Adult stem cells (e.g., haematopoietic stem cells from bone marrow): minimal ethical controversy; the donor provides informed consent in the usual way.
- Cord blood stem cells: collected from umbilical cord blood at birth; generally low ethical controversy; requires maternal consent.
- Induced pluripotent stem cells (iPSCs): adult cells reprogrammed to a pluripotent state; largely sidestep embryo destruction controversies; the primary concern is ensuring donor consent and privacy of the donor's genetic material.
- Embryonic stem cells (ESCs): derived from the inner cell mass of blastocysts (typically 4–5-day-old embryos). This source generates the most intense ethical debate because obtaining ESCs destroys the embryo. The central controversy is the moral status of the early embryo: those who consider the embryo a full moral person (from fertilisation) regard ESC research as equivalent to destruction of human life; others argue the blastocyst has a different moral status from a developed human being.
Ethical issues in stem cell research:
1. Embryo destruction — the derivation of ESCs destroys the embryo; morally contested.
2. Commercialisation and commodification — purchasing eggs or embryos creates markets in human biological material.
3. Informed consent for donors — egg donors face ovarian hyperstimulation; consent must cover potential risks, future uses of cells, and commercialisation.
4. Reproductive cloning — if somatic cell nuclear transfer (SCNT) is used to generate patient-specific stem cells (therapeutic cloning), the same technology could theoretically produce reproductive clones (human cloning); this is universally prohibited.
5. Germline modification — editing stem cells in ways that produce heritable genetic changes raises profound multigenerational ethical concerns.
Regulatory framework in India (ICMR and DBT guidelines):
- The ICMR and Department of Biotechnology (DBT) jointly developed the National Guidelines for Stem Cell Research (2017) governing permissible and prohibited activities.
- Permitted under strict oversight: adult and cord blood stem cell research; clinical trials of stem cells with Phase I–III registration; iPSC research.
- Permitted with enhanced IEC and national oversight: research on embryonic stem cells derived from supernumerary IVF embryos (with donor couple's consent, no purchase of embryos).
- Prohibited: reproductive cloning; creation of human–non-human chimeras for reproduction; creation of embryos solely for research purposes; research beyond 14 days of embryo culture (the '14-day rule' — the embryo must not be cultured in vitro beyond 14 days post-fertilisation, corresponding to the appearance of the primitive streak and the limit of individuation).
The 14-day rule: Embryos must not be maintained in laboratory culture beyond 14 days of development. This is the international standard (endorsed by ISSCR and ICMR), based on the appearance of the primitive streak (from which the neural axis develops) at day 14 — taken as the point at which individuation is established and meaningful neurological development begins. Some countries are now debating extending this limit to 28 days for specific scientific purposes, but this remains controversial and is NOT current Indian regulatory practice.
Provided image
SELF-CHECK
Under India's National Guidelines for Stem Cell Research (ICMR and DBT, 2017), which of the following activities is PROHIBITED?
A. Research on adult haematopoietic stem cells with donor consent
B. Clinical trials using autologous cord blood stem cells
C. Creation of embryos for the sole purpose of deriving embryonic stem cells
D. Research on induced pluripotent stem cells (iPSCs) with appropriate consent
Reveal Answer
Answer: C. Creation of embryos for the sole purpose of deriving embryonic stem cells
The ICMR/DBT National Guidelines for Stem Cell Research (2017) explicitly prohibit the creation of human embryos specifically and solely for research purposes. Research using stem cells from supernumerary IVF embryos (embryos created for reproductive purposes but no longer required) is permitted under enhanced oversight, but purposively creating embryos just to derive stem cells is prohibited. Adult stem cell research, cord blood research, and iPSC research with consent are permitted. Reproductive cloning is also prohibited.
KEY TAKEAWAYS
Active euthanasia (lethal act) is illegal in India — IPC culpable homicide. Passive euthanasia (withdrawal of life-sustaining treatment) is legally permissible under Aruna Shanbaug (2011) and Common Cause (2018) via Medical Board + Judicial Magistrate process. Advance Directives are legally valid under Common Cause (2018) as part of the Article 21 right to die with dignity. Physician-assisted suicide remains illegal. DNR is a permissible, specific decision not to attempt CPR — not euthanasia — documented through a clinical–family discussion process; DNR does NOT mean withdrawal of all other care. Stem cell ethics: ESC research controversies centre on embryo destruction and moral status; ICMR/DBT 2017 guidelines permit research on supernumerary embryos with consent but prohibit creating embryos for research and reproductive cloning; the 14-day rule prohibits in vitro embryo culture beyond 14 days (primitive streak formation). Adult, cord blood, and iPSC research permitted.
REFLECT
A patient you know well — a 72-year-old former teacher with advanced cardiac failure — tells you she has written an Advance Directive asking that she not be resuscitated or intubated if her condition deteriorates. Her daughter insists you should 'do everything possible.' How would you navigate this ethical and legal tension? What does the Common Cause ruling give you the right and obligation to do? Reflect on the principles of autonomy, beneficence, and non-maleficence in this scenario, and how the legal framework protects the patient's right to die with dignity.