Page 10 of 17
FM8.12-14 | Sterilization, Contraception, ART & Surrogacy — SDL Guide
Learning Objectives
- Describe sterilisation procedures in males (vasectomy) and females (tubectomy/tubal ligation) within the National Family Planning Programme
- Explain artificial insemination, IVF/test tube baby, surrogate motherhood, and hormone replacement therapy with their national and state legal contexts
- State the key provisions of the ART (Regulation) Act 2021 and the Surrogacy (Regulation) Act 2021
- Clearly distinguish the ART Act (covers clinics and procedures) from the Surrogacy Act (regulates surrogacy arrangements, bans commercial surrogacy)
- Identify the medicolegal issues arising from surgical contraception and ART procedures
INSTRUCTIONS
Assisted reproduction and surgical contraception sit at the intersection of medical science, ethics, and Indian law. Two landmark statutes enacted in 2021 — the ART (Regulation) Act and the Surrogacy (Regulation) Act — dramatically altered the regulatory landscape. This module covers the surgical and clinical methods alongside the legal framework, equipping you to identify medico-legal issues when they arise in clinical practice.
References
- KSN Reddy — Essentials of Forensic Medicine & Toxicology (textbook)
- BV Subrahmanyam — Modi's Medical Jurisprudence and Toxicology (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 35-year-old woman approaches a fertility clinic after years of infertility. She and her husband want to use in-vitro fertilisation with donor eggs and have approached a woman willing to carry the pregnancy as a surrogate for payment. The clinic director is unsure whether this arrangement is legal under the new 2021 Acts. Separately, a man presents claiming he underwent vasectomy five years ago and his wife is now pregnant — he wants a medico-legal opinion. Both cases require the clinician to know the 2021 legislative framework and the scientific basis of these procedures.
WHY THIS MATTERS
Sterilisation is the most widely used method of contraception in India, with millions of tubectomies performed annually through the National Family Planning Programme. When a sterilisation procedure fails — and failure rates, while low, are not zero — the medicolegal implications for the surgeon and the couple are significant. ART clinics are sites of complex legal and ethical issues involving gamete donation, embryo storage, and surrogacy. The 2021 Acts created formal registration, oversight, and prohibited practice frameworks that all doctors must understand.
RECALL
From Year-1 anatomy and physiology: recall the anatomy of the vas deferens (in the scrotum, the most accessible segment for vasectomy), the fallopian tubes (the site of tubectomy — ligated, cut, or coagulated), and the fertilisation process (sperm meets ovum in the ampulla of the fallopian tube). From obstetrics basics: recall that IVF involves ovarian stimulation, oocyte retrieval, in-vitro fertilisation, and embryo transfer. From FM8.9 SDL: recall disputed paternity/maternity — ART opens new categories of genetic vs gestational vs legal parentage that courts must resolve.
Surgical Sterilisation: Vasectomy and Tubectomy in the National Family Planning Programme
Surgical sterilisation is a permanent method of contraception that has been a cornerstone of India's National Family Planning Programme since the 1950s. Both male (vasectomy) and female (tubectomy) procedures are performed under the programme at government hospitals at no cost. The medicolegal issues that arise from these procedures are significant: failed sterilisation, allegations of negligence, unconsented sterilisation, and complications.
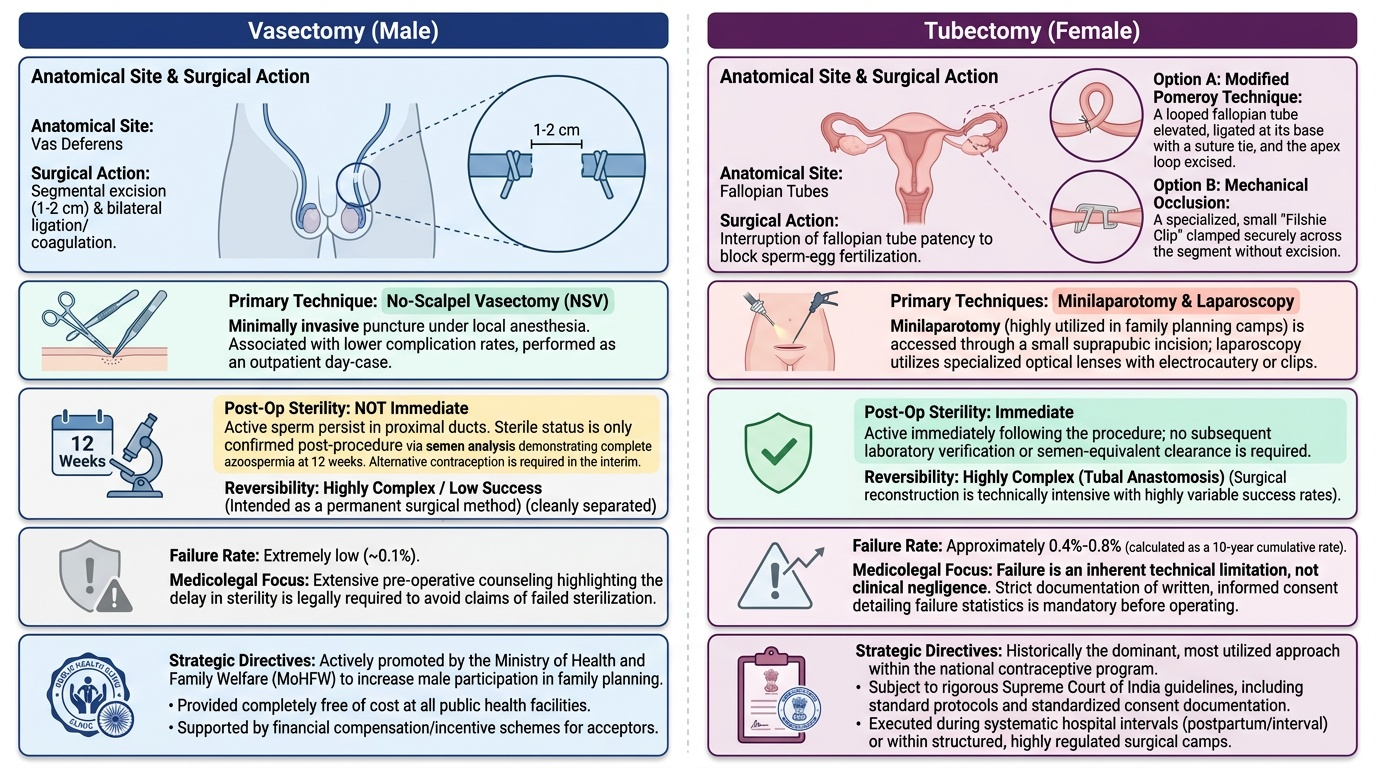
Vasectomy is the surgical division of the vas deferens to prevent sperm from mixing with seminal fluid. The standard procedure involves bilateral scrotal incision (or the No-Scalpel Vasectomy/NSV technique, the preferred method in the National Programme), isolation of the vas deferens, excision of a segment (typically 1-2 cm), and ligation or coagulation of the cut ends. The procedure is performed under local anaesthesia as a day-case procedure. NSV has a lower complication rate than conventional vasectomy and is the technique promoted by MoHFW. Post-vasectomy, azoospermia must be confirmed by semen analysis at 12 weeks; the man is not sterile immediately after the procedure (residual sperm persist in the proximal ducts).
Tubectomy (female sterilisation) involves interruption of the fallopian tubes to prevent fertilisation. Methods include: (a) Modified Pomeroy technique (the most common) — the tube is elevated into a loop, a suture ligates the base, and the loop is excised; (b) Filshie clips / Hulka clips — mechanical occlusion without excision; (c) Laparoscopic electrocautery — thermal occlusion; (d) Minilaparotomy (the most common approach in the National Programme — small suprapubic incision, performed postpartum or interval).
Medicolegal issues in sterilisation:
- Failure rate: tubal ligation has a lifetime failure rate of approximately 0.4-0.8% (10-year cumulative). This is not negligence — it is an inherent technical limitation that must be explained to the patient at counselling.
- Informed consent: the patient must be counselled on failure rates, permanence, and alternatives. Consent forms under the National Programme are prescribed; their proper completion is essential.
- Unconsented sterilisation: historically, mass sterilisation camps in India led to non-consensual or coerced sterilisation — a serious human rights violation and a legal offence. Court-ordered sterilisation of persons with disabilities is not permissible without proper legal process.
- Sterilisation as abortion-prevention: sterilisation before or after an abortion must be separately consented to and documented.
Provided image
SELF-CHECK
A woman underwent minilaparotomy tubectomy 6 years ago. She is now 8 weeks pregnant. Her husband has filed a complaint claiming the doctor was negligent. Which principle governs the medicolegal assessment?
A. Pregnancy after tubal ligation is conclusive evidence of surgical negligence
B. Tubal ligation has an inherent failure rate (~0.4-0.8% lifetime) that is not negligence; the patient must have been informed of this at consent
C. The surgeon is liable only if the standard Pomeroy technique was not used
D. Pregnancy after tubal ligation can only occur if the doctor operated on the wrong structure
Reveal Answer
Answer: B. Tubal ligation has an inherent failure rate (~0.4-0.8% lifetime) that is not negligence; the patient must have been informed of this at consent
Tubal ligation has a documented lifetime failure rate, which must be disclosed at consent. This represents an inherent limitation of the procedure, not negligence. Negligence would require showing a departure from standard of care — e.g., failure to ligate both tubes, wrong-structure identification, or inadequate technique — not simply the occurrence of failure within the known statistical rate.
ART Methods: Artificial Insemination, IVF, and Surrogacy
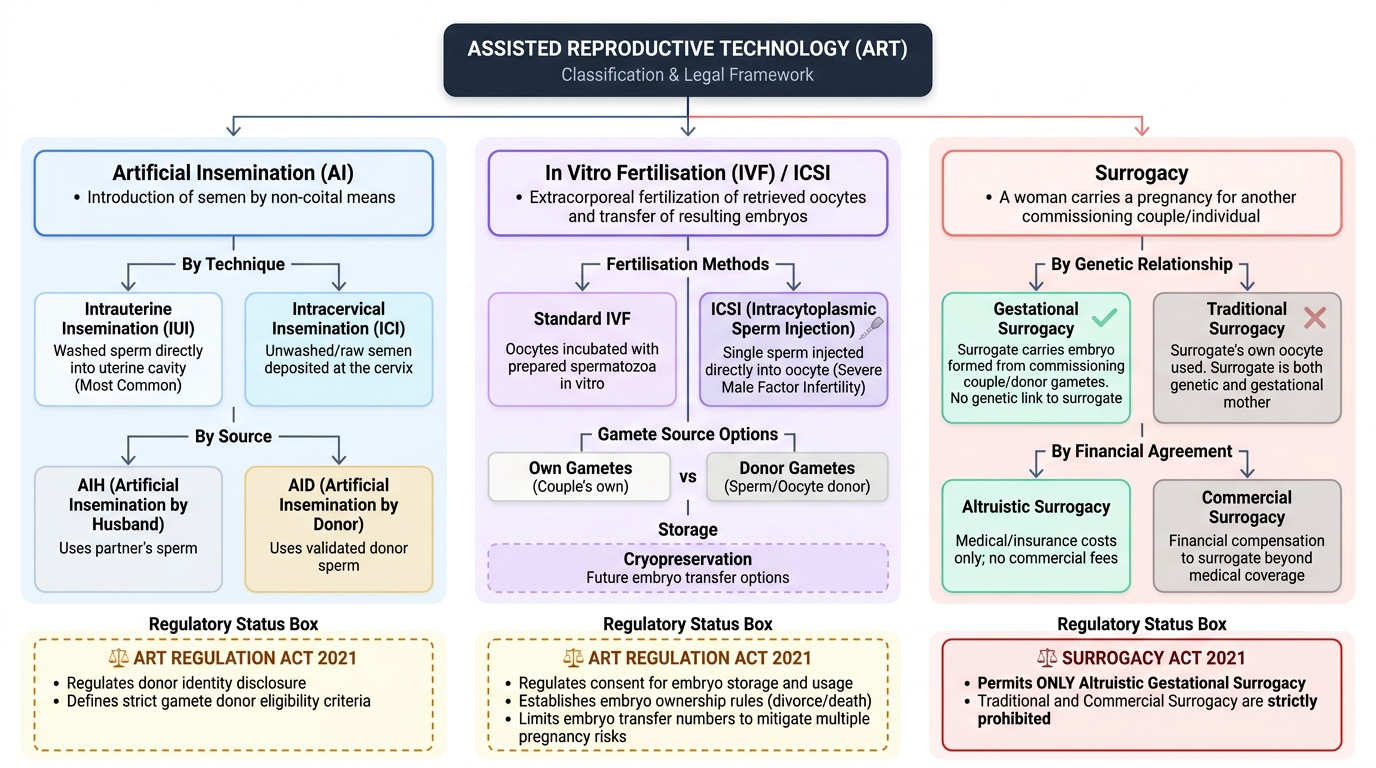
Artificial insemination (AI) involves the introduction of spermatozoa into the female reproductive tract by non-coital means. Two variants: (1) Intrauterine insemination (IUI) — washed spermatozoa are deposited directly into the uterine cavity, the most common form; and (2) Intracervical insemination (ICI) — semen deposited at the cervix. AI may use the husband's sperm (AIH — artificial insemination by husband) or donor sperm (AID — artificial insemination by donor). AID raises complex legal issues of paternity: the ART Regulation Act 2021 now regulates donor identity disclosure and gamete donor eligibility.
In vitro fertilisation (IVF) / Test tube baby: Oocytes retrieved by transvaginal ultrasound-guided follicle aspiration after ovarian stimulation are fertilised in the laboratory with prepared spermatozoa, cultured as embryos, and transferred to the uterus. IVF may use the couple's own gametes or donor oocytes/sperm. Embryos may be cryopreserved for future transfer. Intracytoplasmic sperm injection (ICSI) — injection of a single sperm directly into an oocyte — is used where male factor infertility is severe. Medicolegal issues: multiple pregnancy risk (historically from transferring multiple embryos — now regulated), embryo ownership and storage consent, use of cryopreserved embryos after divorce or death of a partner.
Surrogate motherhood: A surrogate is a woman who carries a pregnancy for another couple/individual. Two types: (1) Gestational surrogacy — the surrogate carries an embryo formed from the commissioning couple's (or donor's) gametes; the surrogate has no genetic link to the child; (2) Traditional surrogacy — the surrogate's own oocyte is used (she is both genetic and gestational mother). The Surrogacy Act 2021 (see below) now permits only altruistic gestational surrogacy.
Hormone replacement therapy (HRT): Administration of oestrogen (± progesterone) to address menopausal symptoms or surgical hypogonadism. Medicolegal issues arise where HRT is prescribed for gender-affirming purposes in transgender persons — the Transgender Persons Act 2019 addresses access to medical care.
Provided image
ART (Regulation) Act 2021 and Surrogacy (Regulation) Act 2021
Both statutes were enacted in December 2021 — enacted in the same session of Parliament but are distinct Acts governing distinct matters. Confusing them in a medico-legal report or examination is a common error.
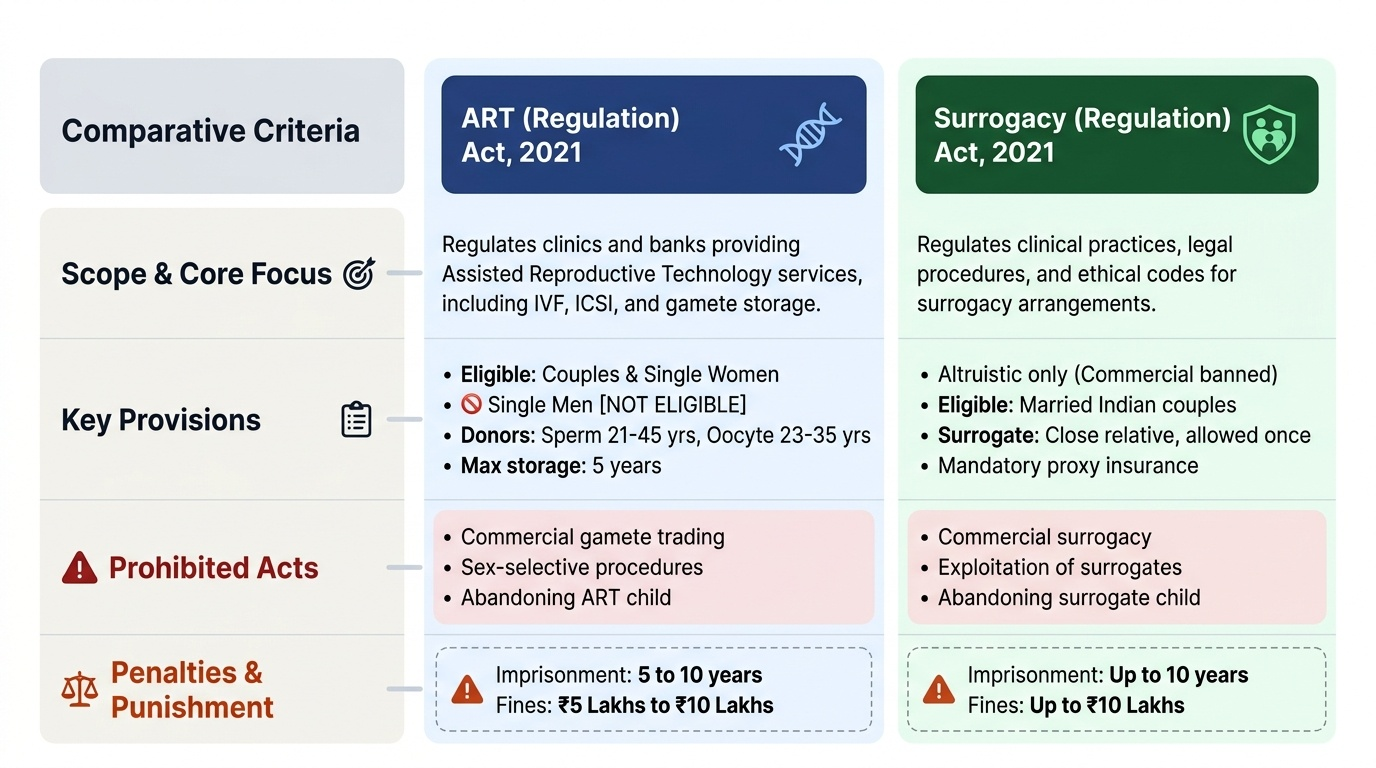
ART (Regulation) Act 2021 — this Act regulates clinics and banks providing assisted reproductive technology services. Key provisions:
- Registration: all ART clinics and ART banks must register with the National Registry of ART Clinics and Banks under the National Board; unregistered practice is an offence.
- Eligibility for commissioning couples: heterosexual married couples and single women (not single men — this specific exclusion is specified in the Act).
- Gamete donation regulation: sperm donors must be between 21-45 years, oocyte donors must be between 23-35 years; a woman can donate oocytes only once; gamete donation is compensated (expenses only, not for profit). Donor identity is maintained confidential from the recipient but accessible to the child at 18 years.
- Embryo storage: embryos may not be stored beyond 5 years without specific consent; abandoned embryo protocols are specified.
- Offences: commercial gamete trading, sex-selective ART, abandoning a child born via ART, and offering ART services to ineligible persons are criminal offences.
Surrogacy (Regulation) Act 2021 — this Act regulates surrogacy arrangements specifically. Key provisions:
- Prohibition of commercial surrogacy: surrogacy for money or any non-medical material benefit (beyond reasonable medical expenses and insurance) is prohibited. This is the most important provision — it bans commercial surrogacy.
- Permitted surrogacy: only altruistic surrogacy is allowed — where a close relative (intending couple's relative) agrees to carry the pregnancy without payment.
- Eligibility of intending couple: a heterosexual married couple; woman aged 23-50 years, man aged 26-55 years; couple must have a medical indication for surrogacy.
- Eligibility of surrogate: she must be a close relative of the intending couple, a married woman with at least one child of her own, aged 25-35 years; she may serve as a surrogate only once in her lifetime.
- Registration boards: National Surrogacy Board and State Surrogacy Boards oversee implementation.
- Offences: commercial surrogacy arrangement, abandoning a surrogate child, using a surrogate not meeting eligibility criteria, and sex selection through surrogacy are criminal offences.
Key distinction to remember: The ART Act covers ART clinics, banks, procedures, and gamete donation. The Surrogacy Act covers surrogacy arrangements specifically. A clinic may be compliant with the ART Act but still violate the Surrogacy Act if it facilitates a commercial surrogacy.
Provided image
SELF-CHECK
Under the Surrogacy (Regulation) Act 2021, which of the following surrogacy arrangements is permitted?
A. A woman agrees to carry a pregnancy for a couple she does not know, receiving payment of ₹5 lakhs
B. A cousin of the intending wife, who has two children of her own, agrees to carry the pregnancy out of family affection without payment
C. A single man wishes to commission surrogacy using a donor oocyte and his sperm
D. A lesbian couple commissions surrogacy from a professional agency
Reveal Answer
Answer: B. A cousin of the intending wife, who has two children of her own, agrees to carry the pregnancy out of family affection without payment
The Surrogacy Act 2021 permits only altruistic surrogacy by a close relative of the intending couple, without payment, where the surrogate meets eligibility criteria (married, own child, aged 25-35). Commercial surrogacy (option A), single male commissioning (option C — single women permitted under ART Act for ART but surrogacy Act has specific restrictions), and non-heterosexual couples (option D) are not permitted under the current Act.
SELF-CHECK
Which of the following correctly distinguishes the ART (Regulation) Act 2021 from the Surrogacy (Regulation) Act 2021?
A. The ART Act bans commercial surrogacy; the Surrogacy Act regulates IVF clinics
B. The ART Act regulates ART clinics, banks, and procedures; the Surrogacy Act specifically regulates surrogacy arrangements and prohibits commercial surrogacy
C. Both Acts are identical in scope and were enacted as companion legislation
D. The Surrogacy Act permits commercial surrogacy subject to licensing
Reveal Answer
Answer: B. The ART Act regulates ART clinics, banks, and procedures; the Surrogacy Act specifically regulates surrogacy arrangements and prohibits commercial surrogacy
The ART Act covers ART clinics and banks (registration, gamete donation, embryo storage). The Surrogacy Act is a separate statute covering surrogacy arrangements exclusively and specifically prohibits commercial surrogacy, permitting only altruistic surrogacy by a close relative.
CLINICAL PEARL
The most common exam error on the 2021 Acts is to describe the Surrogacy Act as permitting commercial surrogacy with conditions — it does not. Commercial surrogacy is absolutely prohibited. Only altruistic surrogacy by a close relative meeting specific criteria is permitted. This is a deliberate policy choice to prevent exploitation of economically vulnerable women as 'rent-a-womb' surrogates.
KEY TAKEAWAYS
Surgical sterilisation (vasectomy via NSV, tubectomy via modified Pomeroy or minilaparotomy) is conducted under the National Family Planning Programme; inherent failure rates (tubal ligation ~0.4-0.8% lifetime) are not negligence if properly consented. ART methods: AIH/AID, IVF/ICSI, surrogacy. ART (Regulation) Act 2021 regulates ART clinics and banks — registration, gamete donor eligibility, embryo storage, and offences. Surrogacy (Regulation) Act 2021 prohibits commercial surrogacy; only altruistic surrogacy by a close relative meeting specific eligibility criteria is permitted. The two Acts are distinct in scope: ART Act = clinics and procedures; Surrogacy Act = surrogacy arrangements.
REFLECT
A patient asks you: 'My sister is willing to carry my baby because I cannot due to a medical condition. She wants to be paid for her time and suffering. Is this legal?' How would you counsel this patient under the Surrogacy (Regulation) Act 2021? What arrangement would be legal, and what would not be? What documentation requirements apply?