Page 1 of 33
FM13.11 | Corrosive Poisons (Acids) — SDL Guide
Learning Objectives
- Identify the common corrosive acids (sulphuric, nitric, hydrochloric, carbolic/phenol, oxalic, acetylsalicylic) and their characteristic features
- Explain the pathological mechanisms of tissue destruction for each agent
- Describe the clinical examination findings and post-mortem appearances in corrosive acid poisoning
- Apply the management framework — decontamination, supportive care, specific antidotes, and enhanced elimination — to each agent
- Prepare a medicolegal report and identify relevant IPC sections in acid attack cases
INSTRUCTIONS
Corrosive acid poisoning occupies a unique position in forensic medicine — it arises both as a criminal act (acid attack, homicide) and as an accidental or suicidal ingestion. As a doctor, you may be called to examine a living victim for injury documentation or a deceased for post-mortem findings, and you may be asked to testify about the nature of injury and its potential medicolegal significance. This SDL builds the scientific and clinical foundation you need for both roles.
References
- KSN Reddy — Essentials of Forensic Medicine & Toxicology (textbook)
- BV Subrahmanyam — Modi's Medical Jurisprudence and Toxicology (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 24-year-old woman is brought to the emergency department with severe facial and neck burns. She is in acute distress, unable to swallow, and her clothing is damaged in a splash pattern. The accompanying police officer tells you she was attacked outside her home thirty minutes ago — a substance was thrown at her face. Bystanders report a pungent, suffocating smell. You are asked to examine her, document the injuries formally, and advise on immediate treatment. Later, you may be required to testify about whether the injuries are consistent with a specific acid, their severity under IPC classification, and the prognosis. What do you need to know — and do — right now?
WHY THIS MATTERS
Acid attacks are unfortunately a recognised pattern of violence in India and South Asia, and they generate some of the most demanding medicolegal work a doctor will encounter. Beyond criminal assaults, corrosive acid ingestion — whether suicidal, accidental, or homicidal — requires urgent clinical management and precise injury documentation. The same pharmacological principles (mechanism of injury, systemic toxicity, antidote logic) that guide treatment also underpin every medicolegal opinion you will form. Forensic medicine graduates are uniquely placed to bridge clinical care and legal testimony in these cases.
RECALL
Before you proceed, retrieve what you already know from Year 1:
- From Physiology: the normal acid-base balance — pH 7.35–7.45, buffer systems (bicarbonate, haemoglobin, phosphate), the kidney's role in bicarbonate reabsorption, and the concept of anion-gap metabolic acidosis (AG = Na⁺ − [Cl⁻ + HCO₃⁻], normal 8–12 mEq/L — elevated when non-chloride acids accumulate).
- From Anatomy: the oesophagus traverses three anatomical narrowings (cricopharyngeus, aortic arch, diaphragmatic hiatus) — these are the sites most vulnerable to stricture after caustic ingestion.
- From Biochemistry: protein denaturation — the loss of secondary/tertiary structure of proteins by pH extremes — which is the cellular mechanism behind coagulation necrosis.
- From Pharmacology (Year 2): the basic principles of toxicokinetics — absorption, distribution, first-pass, and the concept of enhanced elimination (haemodialysis, urinary alkalinisation).
Medicolegal Scenario: The Acid Attack
Corrosive poisoning, particularly by strong acids, represents one of the most severe forms of chemical assault in forensic medicine. Acid attacks — the deliberate throwing or applying of acid onto a person — constitute a criminal offence under the Indian Penal Code, and the doctor who first examines the victim occupies a critical role: part clinician, part evidence collector, and part expert witness. The medicolegal significance begins the moment the patient arrives.
Provided image
The forensic relevance of corrosive poisoning extends beyond assault. Suicidal ingestion of concentrated acids (notably sulphuric acid in India, carbolic acid/phenol historically, hydrochloric acid in industrial settings) presents as a combined toxicological emergency and potential coroner's or magistrate's case. Accidental poisoning — oxalic acid in food (rhubarb leaves), acetylsalicylic acid (aspirin) in children or elderly — requires documentation of exposure circumstances. Homicidal administration via food or drink, though less common with strong acids, has been reported and demands careful investigation of the mode of access.
Key medicolegal questions that arise in every corrosive case:
- Is this injury self-inflicted, accidental, or criminal? (distribution, splash pattern, site of primary contact, accessibility)
- What is the nature of grievous hurt? (IPC §320 — acid attack causing permanent disfigurement or disability)
- Which acid caused the injury? (colour of burns, odour, characteristic staining — a question for both clinician and analytical toxicologist)
- What is the prognosis for permanent impairment? (ocular, oesophageal, laryngeal)
Pathological Basis of Corrosive Injury
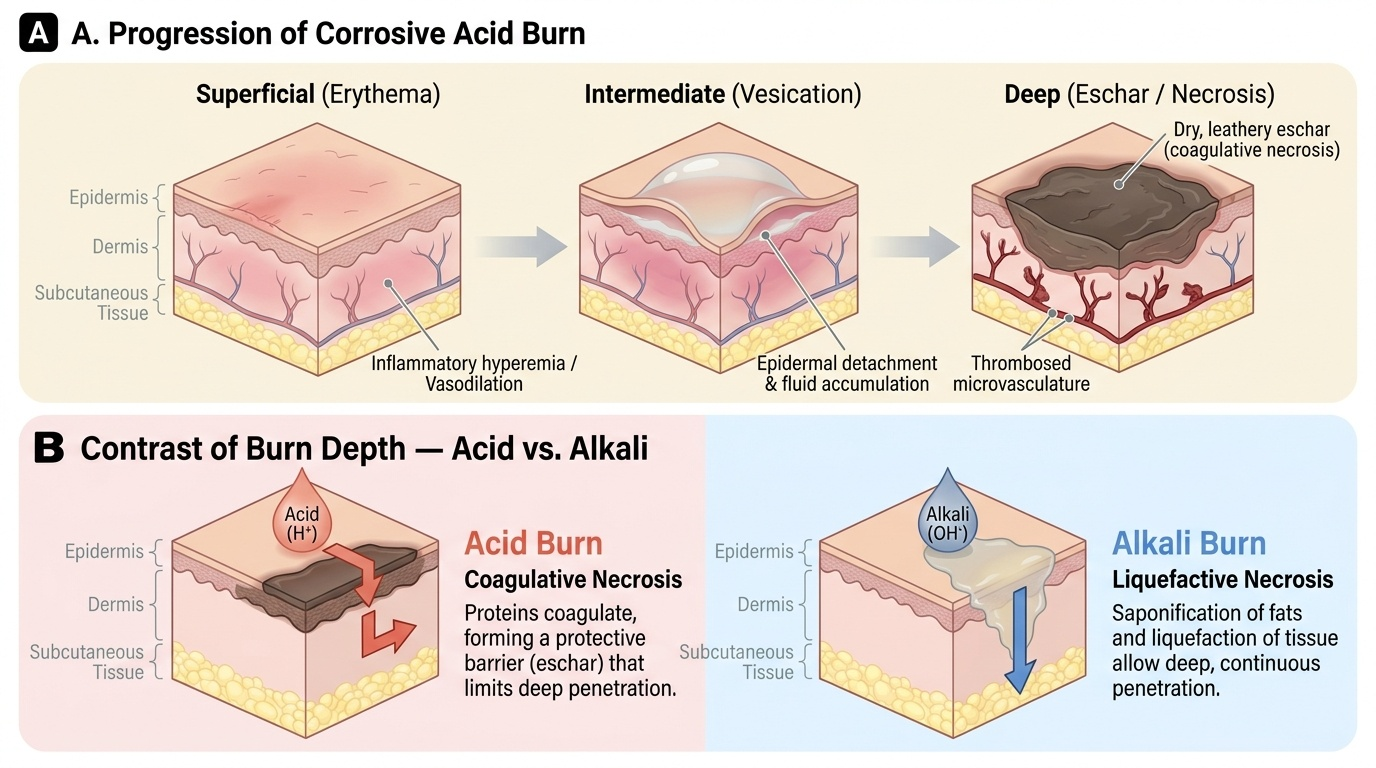
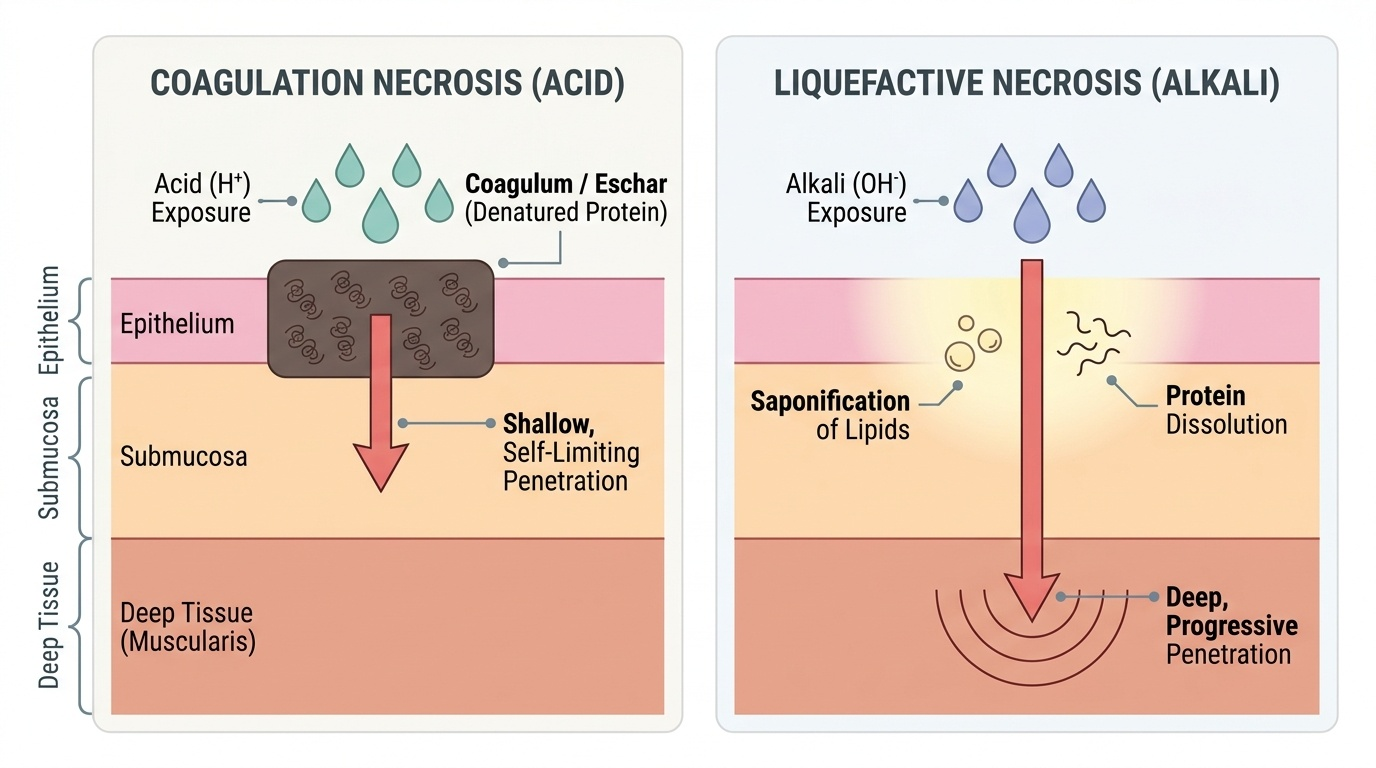
Understanding WHY acids cause the injuries they do is prerequisite to recognising what you see clinically and at post-mortem. Strong acids are tissue destructors — they cause coagulation necrosis by denaturing proteins at the point of contact, forming a firm, leathery eschar (coagulum) that, paradoxically, limits deeper penetration. This is in direct contrast to alkali injuries (liquefactive necrosis — saponification of lipids and dissolution of proteins allows deeper penetration). The eschar formed by strong acids acts as a partial physical barrier, which is why the depth of acid injury, while severe, is often somewhat self-limiting compared with equivalent alkali exposure.
Beyond the local coagulative effect, acids differ markedly in their systemic potential:
- Mineral acids (H₂SO₄, HNO₃, HCl) — primarily local corrosive. Systemic acidosis can occur in large ingestions as the absorbed hydrogen ions overwhelm buffering capacity. Sulphuric acid also liberates heat on contact with water (exothermic dissolution), adding a thermal injury component.
- Carbolic acid (phenol/lysol) — this compound is unique because it is absorbed rapidly across all mucous membranes and even intact skin, causing significant systemic toxicity — CNS depression (initially excitement → convulsions → coma), renal tubular necrosis, and haemolysis. The urine turns dark green/black (phenoluria/carboluria). The corrosive local effect (white eschar turning brown) is secondary to the systemic danger.
- Oxalic acid — the toxic mechanism is primarily systemic. Absorbed oxalate ions chelate serum calcium to form insoluble calcium oxalate, producing acute hypocalcaemia (serum Ca²⁺ <1.8 mmol/L → carpopedal spasm, tetany, prolonged QT, ventricular arrhythmia). Renal tubular deposition of calcium oxalate crystals causes acute renal injury. The local corrosive effect on mucous membranes is relatively mild.
- Acetylsalicylic acid (aspirin) — at therapeutic doses anti-inflammatory; in overdose, salicylate produces a characteristic biphasic acid-base disturbance: early respiratory alkalosis (direct stimulation of the respiratory centre → hyperventilation → CO₂ loss), followed by metabolic acidosis (salicylate itself as an organic acid; uncoupling of oxidative phosphorylation → lactic acid and ketoacid accumulation). High-dose aspirin toxicity is therefore NOT primarily a local corrosive injury but a systemic metabolic emergency.
Provided image
Classification and Identification of Common Corrosive Acids
The FM13.11 competency lists six agents that a forensic medicine graduate must know in detail. Each has distinctive identifiable features that assist both clinical management and forensic identification. The following systematic overview covers all required agents, organised by chemical class.
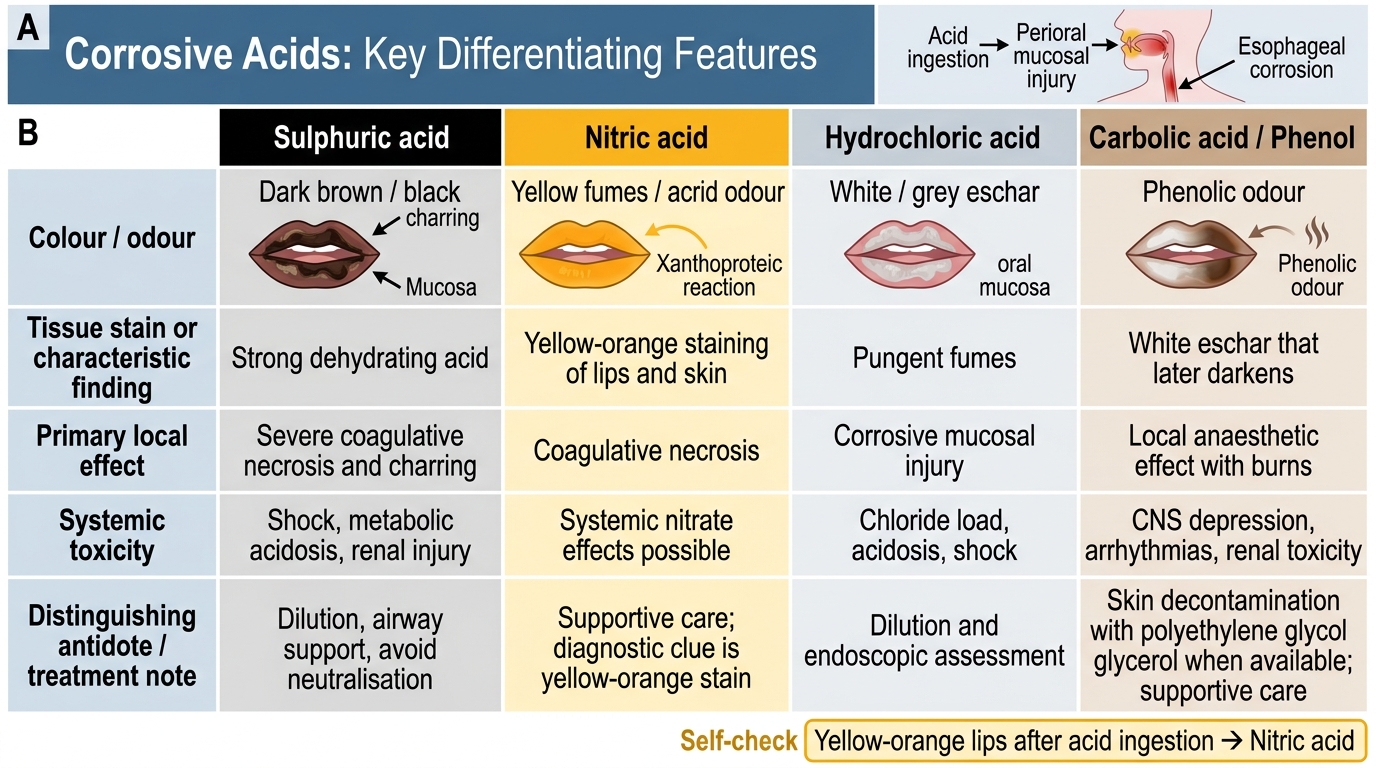
1. Sulphuric acid (H₂SO₄) — the most common acid in Indian forensic practice, widely available as battery acid and industrial chemical. Concentrated H₂SO₄ is colourless, oily, and highly hygroscopic (produces intense heat on contact with water or tissue). Injuries are characterised by black/dark-brown charring of tissues (due to carbonisation — dehydration of organic matter). The smell is acrid-pungent; vapours cause severe respiratory tract irritation. Clothing is bleached/charred.
2. Nitric acid (HNO₃) — produces a distinctive xanthoproteic reaction (yellow/orange staining of skin and tissue due to nitration of tyrosine residues in proteins). This yellow/orange colouration is pathognomonic of nitric acid exposure. Fuming nitric acid releases toxic NO₂ gas fumes that cause pulmonary oedema if inhaled.
3. Hydrochloric acid (HCl, muriatic acid) — produces white/grey-whitish eschars. The acid releases hydrogen chloride gas fumes with a characteristic pungent, suffocating odour (distinguishable from H₂SO₄). Industrial availability (toilet bowl cleaners, swimming pool pH adjustment) makes it a common poisoning acid.
4. Carbolic acid (phenol/lysol) — white/colourless crystalline solid that liquefies above 18°C; the commercial preparation lysol is a soap-based solution. The distinctive carboluria (dark green/black urine) is a clinical marker of systemic absorption. The characteristic smell of phenol (antiseptic, phenolic) is recognisable. On skin: initial white eschar turns brown/black. Rapid systemic absorption makes this the most dangerous corrosive acid systemically.
5. Oxalic acid — found naturally in rhubarb leaves, sorrel, and certain plants; also used as a cleaning/bleaching agent. Ingestion causes a gritty, sour taste and mild local irritation. The systemic danger — hypocalcaemia with tetany and renal damage — is disproportionate to the mild local corrosive effect. Urine may contain calcium oxalate crystals (confirmatory). PM examination reveals calcium oxalate crystals in renal tubules.
6. Acetylsalicylic acid (aspirin) — the least locally corrosive of this group. Overdose (>150 mg/kg) is a systemic salicylate poisoning. The clinical picture: hyperventilation (early respiratory alkalosis), tinnitus, deafness, sweating, hyperpyrexia, and eventually metabolic acidosis. Acid-base analysis is more informative than local examination in aspirin poisoning.
Corrosive Acids: Differentiating Clinical Features
SELF-CHECK
A patient who ingested an unknown acid is noticed to have yellow-orange staining of the lips and perioral skin. Which acid is this characteristic of?
A. Sulphuric acid
B. Nitric acid
C. Hydrochloric acid
D. Carbolic acid (phenol)
Reveal Answer
Answer: B. Nitric acid
Nitric acid produces the xanthoproteic reaction — nitration of tyrosine residues in skin proteins creates yellow/orange chromogens. Sulphuric acid causes dark brown/black charring; HCl causes white/grey eschar; phenol initially causes white eschar that darkens.