Page 24 of 33
FM13.20 | Drug Abuse, Mushroom & Food Poisoning — SDL Guide
Learning Objectives
- Identify the major drug classes of abuse — tobacco, cannabis, amphetamines, cocaine, hallucinogens, designer drugs, and solvents — and describe their mechanisms, clinical features, and forensic significance
- Describe the clinical presentations and management of mushroom poisoning syndromes
- Explain the mechanisms and management of common food poisoning organisms
- Describe the medicolegal and statutory framework relevant to drug abuse in India (NDPS Act 1985)
INSTRUCTIONS
Drug abuse, mushroom poisoning, and food poisoning are grouped together in FM13.20 because they represent the overlap of toxicology with public health, criminal law, and mass-casualty events. Drug abuse — particularly of tobacco, cannabis, opioids, and emerging new psychoactive substances — is a growing problem across Indian demographics. Mushroom and food poisoning occasionally cause mass-casualty events at community feasts. This SDL provides forensic medicine graduates with the recognition and response skills for each.
References
- KSN Reddy — Essentials of Forensic Medicine & Toxicology (textbook)
- BV Subrahmanyam — Modi's Medical Jurisprudence and Toxicology (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Three scenarios from a single Saturday evening: At a rave party, a 20-year-old collapses with hyperthermia (41°C), agitation, tachycardia, and dilated pupils — his friends say he took 'molly'. At the same time, a tribal community feast in a forest area leaves twelve people acutely ill, six hours after eating wild mushrooms — some are confused, others have severe abdominal cramps. And at a wedding buffet in a community hall, 80 guests develop vomiting and diarrhoea within 2 hours of the meal. Three toxicological emergencies, three different forensic dimensions — individual criminal law (NDPS Act), mass-casualty poisoning investigation, and food safety negligence.
WHY THIS MATTERS
Drug abuse is increasingly relevant to forensic medicine practice in India as urbanisation, smartphone-enabled drug supply networks, and the rise of new psychoactive substances ('designer drugs') create new patterns of toxicological harm. Cannabis (ganja), tobacco, opioids, and amphetamine-type stimulants are the most prevalent in India. Mushroom poisoning occurs in foraging communities and occasionally as deliberate poisoning (amanita used in homicide). Food poisoning is a recurring mass-casualty event in schools, hospital canteens, and community functions with significant legal and regulatory implications. Each domain has specific forensic medicine responsibilities.
RECALL
Recall from Year-1 and Year-2:
- Nicotinic and muscarinic pharmacology: tobacco's nicotine acts on nicotinic acetylcholine receptors (both CNS and ganglionic). Cannabis's THC acts on CB1 receptors in the CNS (particularly the basal ganglia and limbic system — hence the mood and motor effects).
- Monoamine neurotransmitters: dopamine (reward, movement), serotonin (mood, anxiety, appetite), noradrenaline (arousal, sympathetic). Cocaine and amphetamines increase dopamine/noradrenaline at the synapse — the basis of sympathomimetic toxidrome.
- Serotonin syndrome: triad of cognitive changes + autonomic dysfunction + neuromuscular abnormalities from excess serotonergic activity; distinguish from neuroleptic malignant syndrome (dopamine-related, no clonus) and anticholinergic toxidrome.
- Botulism: Clostridium botulinum toxin is a pre-synaptic cholinergic blocker at both nicotinic NMJ and muscarinic synapses — produces descending flaccid paralysis AND decreased secretions (dry mouth, constipation); the exact pre-synaptic mechanism parallels beta-bungarotoxin of krait venom.
Medicolegal Context: Drug Abuse in India and NDPS Act
Drug abuse has a dual medicolegal dimension in India: it is both a public health problem (requiring care and treatment) and a criminal law matter under the NDPS Act 1985 (Narcotic Drugs and Psychotropic Substances Act).
Provided image
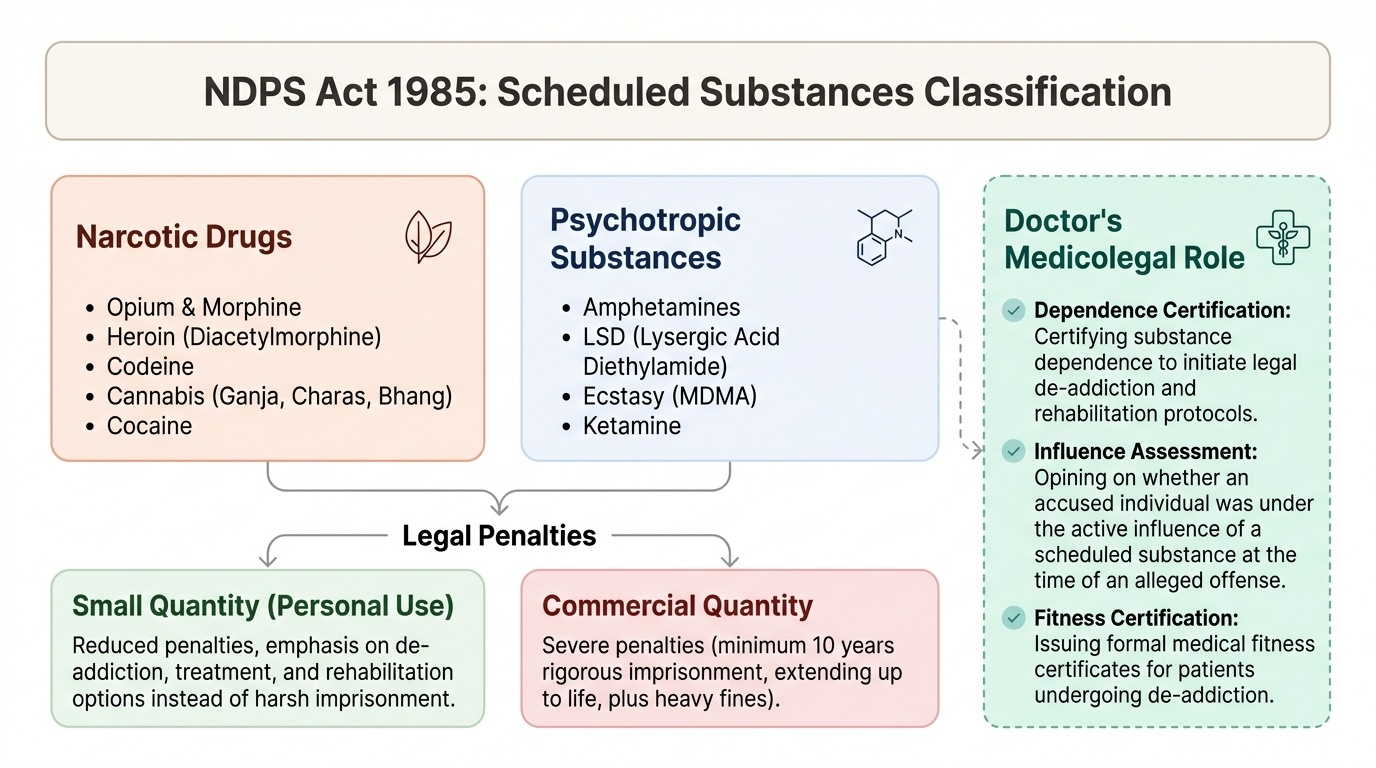
NDPS Act 1985 — key provisions for forensic medicine:
- Schedules narcotic drugs (opium, morphine, heroin, codeine, cannabis/ganja/charas/bhang, cocaine) and psychotropic substances (amphetamines, LSD, ecstasy/MDMA, ketamine)
- Possession of scheduled substances for personal use (small quantity): reduced penalties; possession of commercial quantity: severe penalties (minimum 10 years, possible life)
- The doctor's role: certifying substance dependence for treatment (de-addiction); opining on whether a person was under the influence of a scheduled substance at the time of an alleged offence; issuing fitness certificates for de-addiction.
Forensic categories:
- Drug-facilitated sexual assault: surreptitious administration of sedatives (GHB, benzodiazepines, ketamine) to incapacitate a victim — a criminal offence under IPC §375 (if sexual assault follows) and NDPS Act
- Driving under influence: NDPS Act substances covered alongside alcohol under MVA §185
- Drug-related deaths: post-mortem drug screen (urine/blood for LC-MS/MS) should be routine in any unexplained death of a person aged 15–45
- Cannabis and hemp: distinction between cannabis (THC-bearing plant material, scheduled) and hemp (low-THC; legal in some forms); tested by THC quantification
Major Drugs of Abuse: Mechanisms and Clinical Features
The FM13.20 competency requires knowledge of the following classes: tobacco, cannabis, amphetamines, cocaine, hallucinogens, designer drugs, and solvents. Each has a distinct mechanism, clinical syndrome, and forensic profile.
TOBACCO (nicotine):
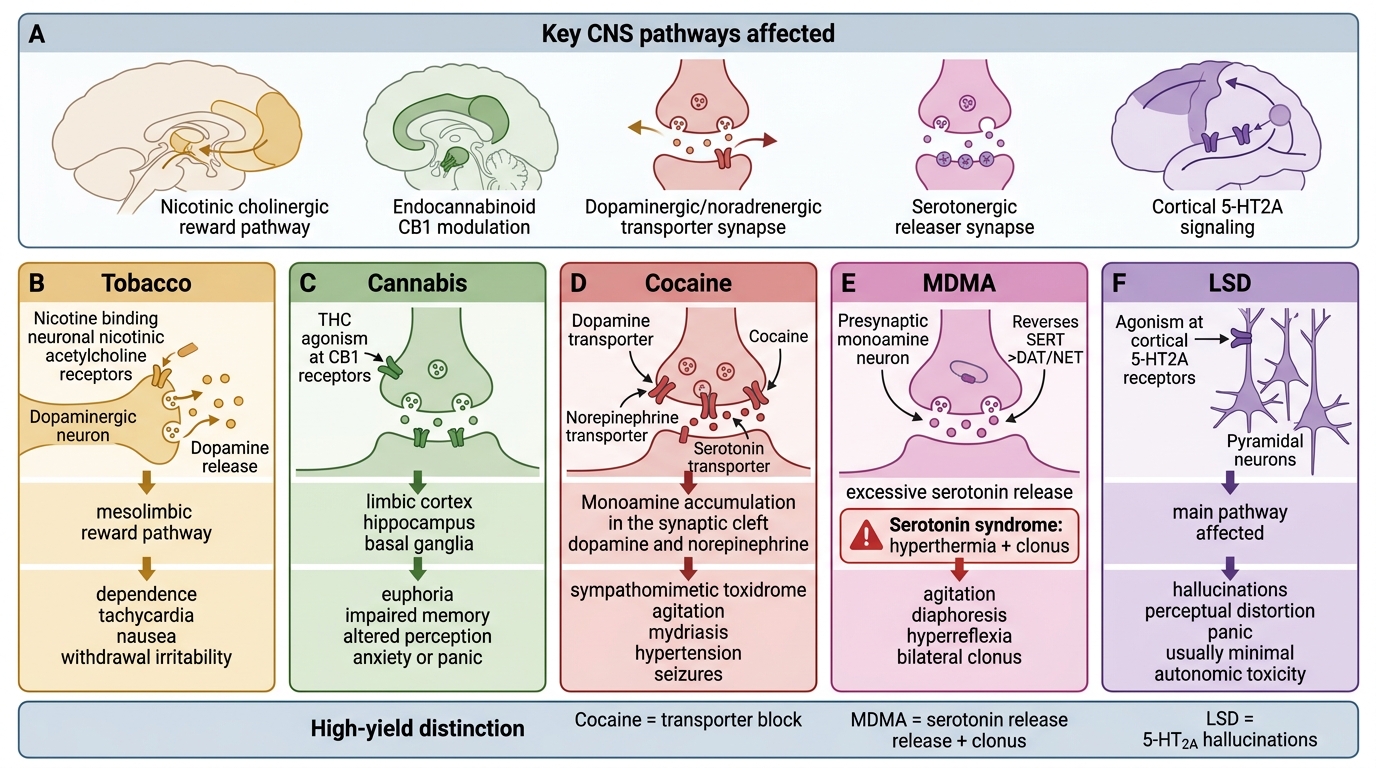
Mechanism: agonism at nicotinic acetylcholine receptors (nAChRs) in the CNS reward pathway (mesolimbic dopamine system) — the basis of addiction. Also cardiovascular effects (sympathomimetic — tachycardia, hypertension) and peripheral nicotinic effects at lower doses.
Forensic significance: nicotine toxicity from liquid nicotine (e-cigarette refill), insecticide nicotine poisoning (rare but documented); tobacco withdrawal in a hospitalised patient may masquerade as agitation. Second-hand smoke exposure in enclosed workplaces and homes is a passive exposure relevant to occupational/civil negligence cases.
CANNABIS (ganja, marijuana, charas, bhang):
Active compound: delta-9-tetrahydrocannabinol (THC) acts on CB1 cannabinoid receptors (CNS, particularly basal ganglia, hippocampus, cerebellum, prefrontal cortex) and CB2 receptors (peripheral, immune). Effects: euphoria, altered time perception, increased appetite ('munchies'), impaired short-term memory, mild perceptual distortions.
Acute toxicity in naïve users: anxiety, panic, tachycardia, paranoia, occasionally psychosis (cannabis-induced acute psychotic episode). Chronic heavy use: cannabis use disorder; amotivational syndrome; increased risk of schizophrenia in genetically susceptible individuals. THC is detectable in urine for up to 30 days after last use in chronic users — forensically relevant (does NOT imply current intoxication).
AMPHETAMINES and MDMA ('ecstasy', 'molly'):
Mechanism: reverse the direction of monoamine transporters → massive release of dopamine + noradrenaline (amphetamines, methamphetamine) or serotonin + dopamine (MDMA) into synaptic clefts. Also inhibit monoamine oxidase (MAO) at high doses.
Sympathomimetic toxidrome: tachycardia, hypertension, hyperthermia, diaphoresis, dilated pupils, agitation, seizures. MDMA specifically: serotonin syndrome (hyperthermia, clonus, hyperreflexia) + hyponatraemia (MDMA promotes SIADH + users often drink excessive water at rave parties → dilutional hyponatraemia → cerebral oedema → death in young women). The rave patient in the hook scenario = classic MDMA presentation.
COCAINE:
Mechanism: blocks monoamine reuptake transporters (dopamine > noradrenaline > serotonin) without releasing stores (unlike amphetamines). Also: local anaesthetic effect (Na⁺ channel block) → topical vasoconstriction (hence the 'Coca-Cola' nose in chronic use — septal perforation from cocaine-induced ischaemia).
Toxidrome: similar to amphetamines (sympathomimetic). Specific complications: cocaine-induced chest pain/MI (coronary artery spasm + accelerated atherosclerosis in young users); stroke; 'crack lung' (alveolar haemorrhage from crack cocaine vapour inhalation).
HALLUCINOGENS:
- LSD (lysergic acid diethylamide): serotonin 5-HT2A partial agonist → perceptual distortion, visual hallucinations, altered sense of self; no direct physical toxicity at standard doses; 'bad trips' (anxiety, paranoia); flashbacks (HPPD — hallucinogen persisting perception disorder)
- Psilocybin (magic mushrooms): same mechanism as LSD (5-HT2A); naturally occurring
- Ketamine: NMDA receptor antagonist (at sub-anaesthetic doses: dissociative); at anaesthetic doses: general anaesthesia. 'K-hole' = profound dissociation. Used in drug-facilitated assault (rapidly incapacitating, amnesia-producing)
- Phencyclidine (PCP): NMDA antagonist; more dangerous than ketamine; severe agitation, psychosis, violence
DESIGNER DRUGS (New Psychoactive Substances, NPS):
Synthetic cannabinoids ('Spice', 'K2') — potent CB1 agonists (often more potent than THC); can cause psychosis, seizures, cardiovascular events. Synthetic cathinones ('bath salts') — amphetamine-like; agitation, hyperthermia. Forensic challenge: standard drug screens may not detect NPS; specific LC-MS/MS panels required.
SOLVENTS (inhalants — 'glue sniffing'):
Mechanism: CNS depression/anaesthesia (various mechanisms including GABA enhancement, NMDA block). Examples: toluene (glue), butane/propane (aerosols), chloroform.
Forensic significance: prevalent among street children; sudden sniffing death — cardiac arrhythmia (sensitised myocardium → adrenaline-triggered VF) during or immediately after solvent inhalation. PM: chemical analysis of blood/lung tissue essential; no specific gross PM findings.
Mechanisms and Clinical Syndromes of Common Psychoactive Poisons
SELF-CHECK
A 22-year-old is brought from a rave party with temperature 41.5°C, severe agitation, hyperreflexia, bilateral clonus, and diaphoresis. She reportedly took 'molly' (MDMA). This clinical picture is most consistent with:
A. Anticholinergic toxidrome from TCA overdose
B. Serotonin syndrome from MDMA's excessive serotonin release
C. Neuroleptic malignant syndrome from antipsychotic drug reaction
D. Organophosphate poisoning — the diaphoresis is cholinergic
Reveal Answer
Answer: B. Serotonin syndrome from MDMA's excessive serotonin release
MDMA causes massive serotonin (and dopamine) release, producing the serotonin syndrome triad: cognitive changes (agitation), autonomic dysfunction (hyperthermia, diaphoresis, tachycardia), and neuromuscular abnormalities (hyperreflexia, clonus). Clonus is the key distinguishing sign of serotonin syndrome — it is NOT seen in anticholinergic toxidrome or NMS. NMS has muscular RIGIDITY (not clonus) and occurs over days, not minutes. OP poisoning is cholinergic (SLUDGE, miosis), not a sympathomimetic/serotonergic picture.
Mushroom Poisoning: Syndromes and Management
Mushroom poisoning follows a pattern-recognition approach: the clinical syndrome depends entirely on the toxin type, and the onset timing provides the critical clue to which toxin is responsible.
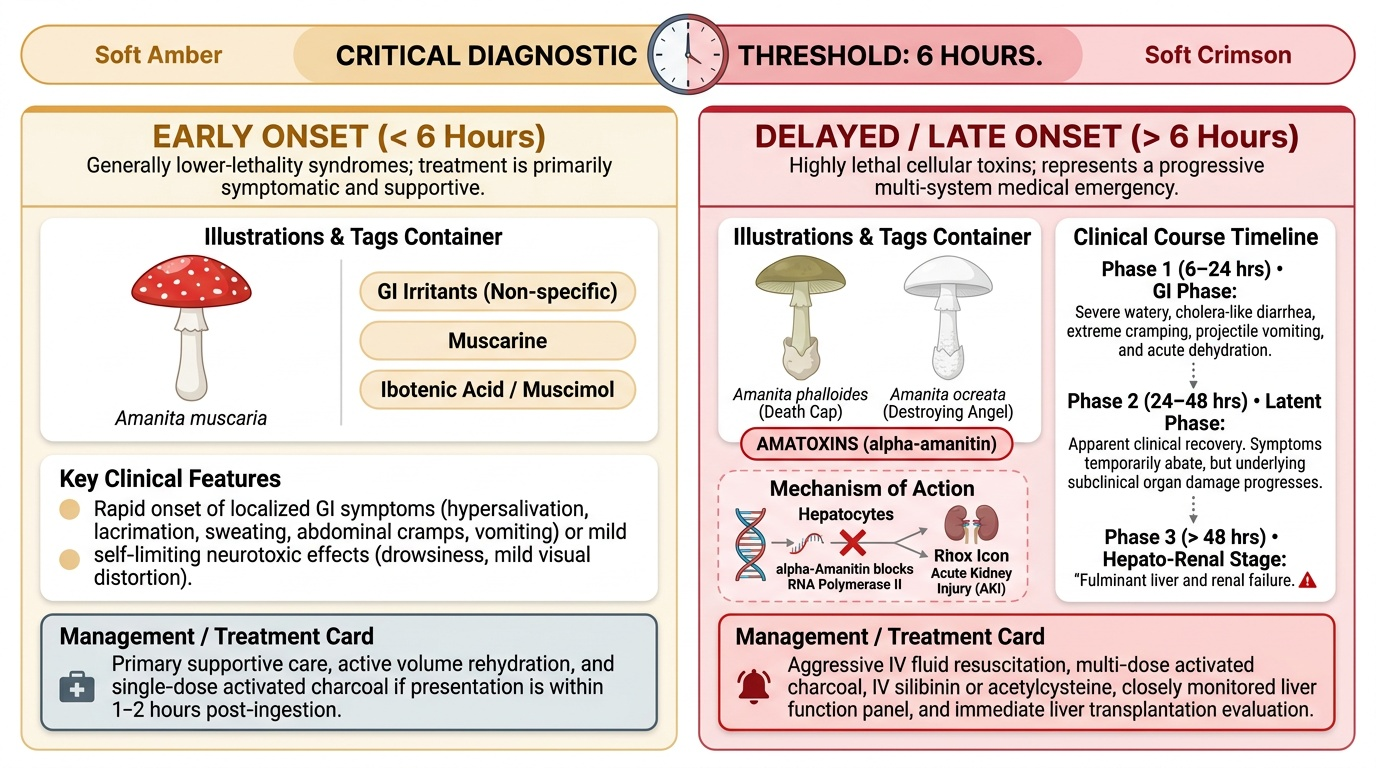
The 6-hour rule:
- Symptoms within 6 hours of ingestion: generally caused by LESS LETHAL toxins (GI irritants, muscarine in small amounts, ibotenic acid/muscimol in Amanita muscaria)
- Symptoms AFTER 6 hours (delayed onset): characteristic of the MOST LETHAL toxins — specifically amatoxins (Amanita phalloides and related species), the most dangerous mushroom toxin type
AMATOXINS — the most lethal mushroom toxins:
Amanita phalloides (death cap), Amanita ocreata (destroying angel), and other Amanita species containing alpha-amanitin are responsible for 90% of fatal mushroom poisoning worldwide.
Mechanism: alpha-amanitin is a highly specific inhibitor of RNA polymerase II — it blocks transcription of mRNA in eukaryotic cells. This preferentially kills the most transcriptionally active cells: hepatocytes (liver failure) and proximal renal tubular cells (renal failure).
Clinical course — three phases:
1. Phase 1 (6–24 h): GI syndrome — severe nausea, vomiting, cholera-like watery diarrhoea; patient appears critically unwell
2. Phase 2 (1–4 days): 'False recovery' — GI symptoms abate; LFTs begin to rise; coagulopathy starts
3. Phase 3 (4–7 days): Fulminant hepatic failure + renal failure; death if liver transplant not performed
No specific antidote (some evidence for IV silibinin/silymarin from milk thistle; N-acetylcysteine as hepatoprotectant). Treatment: supportive; activated charcoal if early; liver transplantation for fulminant hepatic failure.
Other mushroom toxin syndromes:
- Muscarine (Inocybe, Clitocybe): cholinergic toxidrome (SLUDGE syndrome) — onset 30 min to 2 h; treatment: atropine
- Ibotenic acid/muscimol (Amanita muscaria — fly agaric): CNS effects (delirium, seizures, coma); onset 30 min to 2 h; treatment: supportive; benzodiazepines for seizures
- Gyromitrin (false morel — Gyromitra): converted to monomethylhydrazine in the gut → pyridoxine-responsive seizures + haemolysis; treatment: IV pyridoxine (same as INH overdose)
Provided image
SELF-CHECK
Twelve people fall ill after eating wild mushrooms at a forest feast. Three are asymptomatic at 10 hours; nine have recovered from initial GI symptoms. On day 3, two of the 'recovered' patients develop jaundice and coagulopathy. Which toxin and mushroom species is most likely, and what was the forensic significance of the initial 'recovery'?
A. Muscarine (Inocybe) — the SLUDGE syndrome resolved with atropine; jaundice is an unrelated finding
B. Alpha-amanitin (Amanita phalloides) — the 'false recovery' (Phase 2) follows the initial GI phase; hepatorenal failure (Phase 3) follows and is the lethal stage
C. Ibotenic acid (Amanita muscaria) — delirium resolved; delayed hepatotoxicity is common with muscimol
D. Gyromitrin (Gyromitra) — haemolysis causes jaundice; recovery between haemolytic episodes is normal
Reveal Answer
Answer: B. Alpha-amanitin (Amanita phalloides) — the 'false recovery' (Phase 2) follows the initial GI phase; hepatorenal failure (Phase 3) follows and is the lethal stage
Alpha-amanitin (Amanita phalloides and related species) produces the classic three-phase syndrome: Phase 1 = GI crisis (6–24 h), Phase 2 = false recovery (1–4 days — clinically misleading), Phase 3 = fulminant hepatorenal failure (4–7 days). The 'recovery' of the nine patients is the Phase 2 false improvement — it gives a false sense of safety and may lead to discharge before the most lethal phase. Forensically: this pattern (apparent initial recovery → delayed death) is characteristic of amatoxin poisoning. Muscarine causes immediate SLUDGE syndrome (within 30 min–2 h); ibotenic acid causes CNS effects without significant hepatotoxicity; gyromitrin causes haemolysis + seizures.