Page 20 of 33
FM13.18 | Narcotics, Anaesthetics, Cardiotoxic Plants & Insulin — SDL Guide
Learning Objectives
- Describe the toxicokinetics and clinical features of narcotic analgesic overdose and identify naloxone as the specific antidote
- Explain the mechanisms of toxicity of cardiotoxic plants — oleander, Cerbera odollam, aconite, and digitalis — and their post-mortem and clinical features
- Describe insulin overdose and hypoglycaemic coma, including its forensic significance in medically-assisted homicide
- Apply the management framework for overdose with each agent class covered in FM13.18
- Discuss the medicolegal significance of muscle relaxant misuse and anaesthetic-related deaths
INSTRUCTIONS
This SDL covers a diverse but forensically cohesive group of agents — narcotics, general anaesthetics, cardiotoxic plants, and insulin — all of which are associated with deaths that may appear natural unless forensically investigated. Narcotic deaths are increasingly common with opioid misuse. Cardiac glycoside plant poisoning (oleander, Cerbera odollam) is a significant cause of suicidal and homicidal death in South India. Insulin homicide is among the most difficult poisonings to detect post-mortem. Each requires specific forensic alertness.
References
- KSN Reddy — Essentials of Forensic Medicine & Toxicology (textbook)
- BV Subrahmanyam — Modi's Medical Jurisprudence and Toxicology (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Case 1: A 35-year-old healthcare worker is found collapsed in the hospital break room with a syringe near his arm. He has pin-point pupils, respiratory rate of 4 breaths/minute, and is unrousable. Case 2: A family from coastal Tamil Nadu presents to the mortuary — the 60-year-old patriarch died suddenly at home with complaints of nausea and 'heart pounding'. His wife mentions he had a fruit salad from the garden the previous evening, and she describes a tree with red fruits. Case 3: A 40-year-old diabetic woman is found in a coma by her husband — he says he gave her 'her usual insulin' but has been having a marital dispute for weeks. Her blood glucose is 0.8 mmol/L. Case 1 calls for a specific and time-critical antidote. Case 2 calls for knowledge of an Indian plant toxin's forensic signature. Case 3 raises serious homicidal intent concerns. What does each case teach you?
WHY THIS MATTERS
The agents covered in FM13.18 — narcotics, anaesthetics, cardiotoxic plants, and insulin — are united by their forensic pattern of deaths that may appear natural. Opioid deaths simulate sleep; cardiac glycoside poisoning simulates a cardiac event; insulin homicide leaves no gross pathological evidence unless the clinician looks specifically. Anaesthetic-related deaths in healthcare settings raise institutional medico-legal questions. As a forensic medicine graduate, your job is to not accept the superficial appearance of 'natural death' in any of these cases without documented evidence.
RECALL
Recall from Year-2 pharmacology:
- Opioid receptors: μ (mu), κ (kappa), δ (delta) receptors; mu-receptor activation = analgesia + respiratory depression + miosis + constipation + euphoria; mu receptor is the primary target of morphine, heroin, fentanyl. Naloxone is a pure opioid receptor antagonist (competitive at all three receptor subtypes).
- Cardiac glycosides (digoxin): inhibit Na⁺/K⁺-ATPase pump on cardiac cell membrane → intracellular Na⁺ rises → Na⁺/Ca²⁺ exchanger reverses → intracellular Ca²⁺ rises → positive inotropy (therapeutic) + at toxic levels → triggered arrhythmias (DADs — delayed after depolarisations from Ca²⁺ overload).
- Insulin physiology: insulin promotes glucose uptake into cells (via GLUT4 in muscle/fat) → blood glucose falls; in overdose, severe hypoglycaemia → brain glucose deprivation → coma and irreversible neurological injury.
- Succinylcholine pharmacology: depolarising neuromuscular blocking agent — initially causes fasciculations then sustained NMJ block. Metabolised rapidly by plasma pseudocholinesterase. Forensically relevant because it hydrolyses quickly — may be undetectable on post-mortem analysis.
Medicolegal Context: Deaths That Mimic the Natural
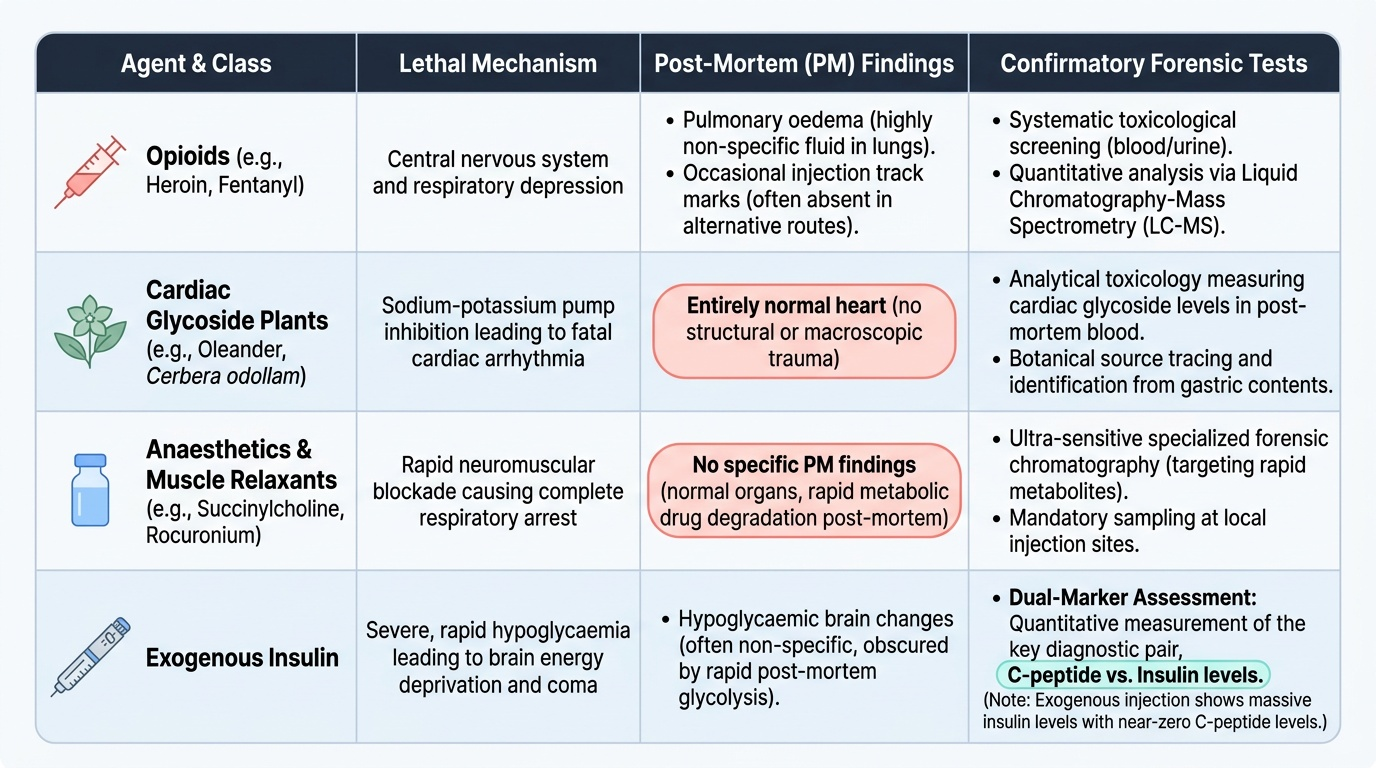
The FM13.18 group of agents shares a forensically critical property: they can cause death with minimal or no post-mortem anatomical findings. This makes them uniquely dangerous in the context of homicide, because without a specific analytical toxicological investigation, the cause of death may be attributed to natural causes.
Opioid overdose deaths may show only pulmonary oedema (non-specific) and possibly injection marks at autopsy. In the absence of drug history or scene evidence, the pathologist must initiate a toxicological screen.
Cardiac glycoside plant poisoning (oleander, Cerbera odollam) kills via arrhythmia — at autopsy, the heart may appear entirely normal. The diagnosis requires analytical toxicology (cardiac glycoside levels in post-mortem blood) or recognition of the plant source.
Insulin homicide is arguably the most forensically difficult category of all: insulin is endogenous, blood glucose level falls post-mortem anyway (from glycolysis by microorganisms), and standard insulin assays may cross-react with endogenous insulin. The forensic approach requires measurement of C-peptide (a byproduct of endogenous insulin synthesis) vs. injected exogenous insulin (which contains NO C-peptide).
Muscle relaxant misuse (succinylcholine, rocuronium) in a healthcare setting causes death by respiratory arrest without gross pathological findings — the drug metabolises rapidly. Forensic chemistry at specialised laboratories is required.
General principle: in any unexpected death of an otherwise-healthy person without obvious trauma, a comprehensive toxicological screen is obligatory before a natural cause of death is certified. The medicolegal doctor should not accept 'cardiac arrest' as a cause of death for a young person without investigating these possibilities.
Provided image
Narcotic Analgesics and Anaesthetics
NARCOTIC ANALGESICS (OPIOIDS):
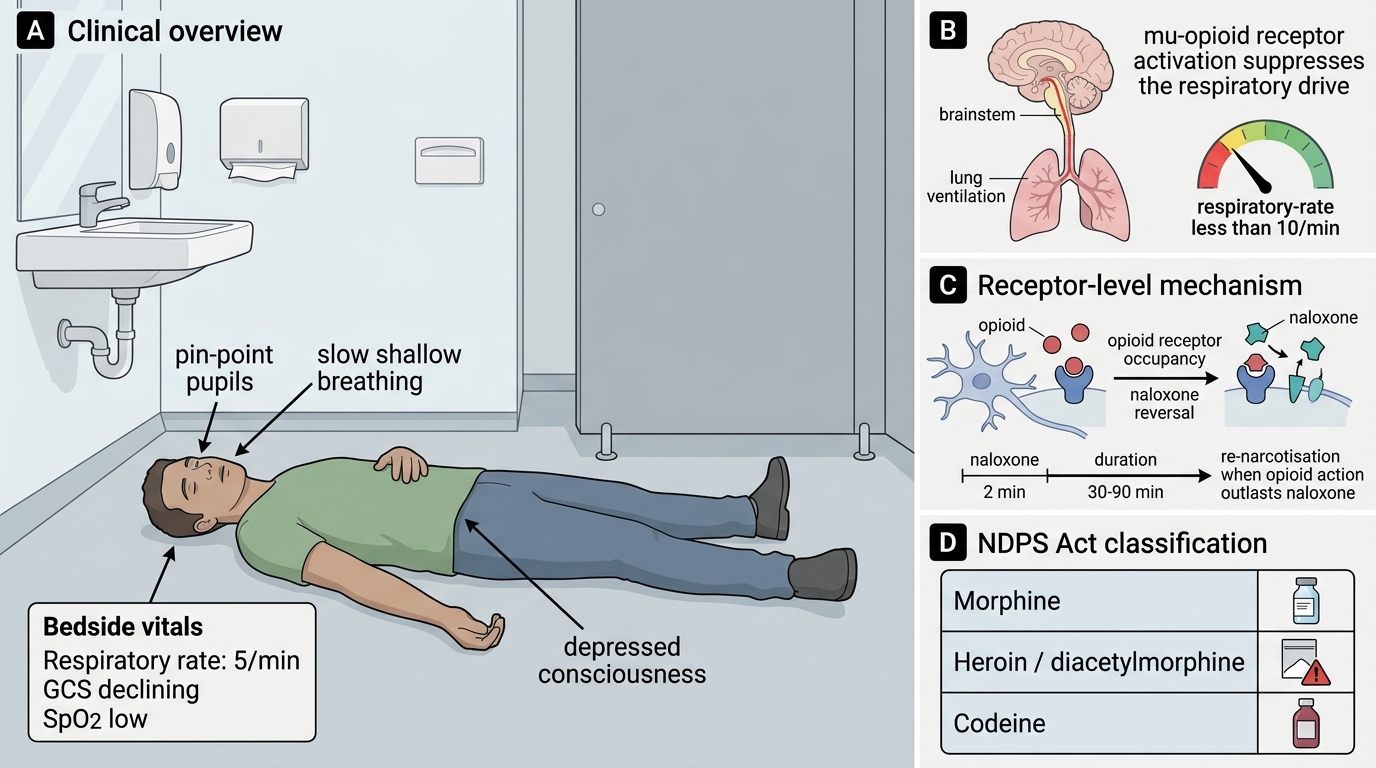
The term 'narcotic' in Indian forensic medicine and law generally refers to opioid analgesics and related NDPS Act-scheduled substances. Morphine, heroin (diacetylmorphine), codeine, tramadol, pethidine, and fentanyl are the key forensically relevant opioids.
Mechanism: Mu (μ)-opioid receptor agonism → inhibition of adenylyl cyclase → reduced neuronal excitability. Central effects: analgesia, euphoria, sedation, respiratory depression. The respiratory depression is the cause of death in opioid overdose.
Opioid toxidrome:
- Miosis (pin-point pupils) — the most reliable clinical sign
- Respiratory depression (rate <10 breaths/min; shallow; Cheyne-Stokes in severe cases)
- CNS depression (reduced consciousness → coma)
- This triad: miosis + respiratory depression + CNS depression = opioid toxidrome
Post-mortem findings:
- Pulmonary oedema (non-cardiogenic; neurogenic)
- Frothy fluid in airways
- Injection marks (particularly antecubital fossa, femoral, neck — in experienced users who have 'used up' veins)
- No specific gross pathological findings; diagnosis confirmed by toxicological analysis
Antidote: naloxone (Narcan)
- Pure competitive opioid receptor antagonist at μ, κ, and δ receptors
- IV/IM/intranasal: onset within 2 minutes
- Duration of action: 30–90 minutes — shorter than most opioids; re-narcotisation occurs as naloxone wears off while opioid levels remain elevated → monitor and repeat dosing, or initiate naloxone infusion
- With fentanyl analogues (ultra-potent — 100× morphine): higher doses of naloxone may be required
General and local anaesthetics (forensic aspects):
Lidocaine (lignocaine) and bupivacaine toxicity: systemic absorption from excess local injection causes CNS toxicity (tinnitus, convulsions) and cardiac toxicity (bupivacaine Na⁺ channel block — cardiac arrest). Antidote: IV lipid emulsion (intralipid 20%) — 'lipid rescue' for bupivacaine cardiac arrest.
Muscle relaxants — forensic significance:
Succinylcholine (suxamethonium) — depolarising NMB agent — used in anaesthesia and occasionally implicated in homicide/suicide in healthcare workers. Metabolised by plasma cholinesterase within minutes → rarely detectable at PM unless collected very early or specialized succinylmonocholine analysis performed. Rocuronium (non-depolarising NMB) — more stable; reversed by sugammadex. Any unexplained respiratory arrest in a person with access to anaesthetic agents should raise suspicion.
Opioid Toxidrome and Naloxone Reversal
SELF-CHECK
A 28-year-old is found unrousable in a public toilet with pin-point pupils and a respiratory rate of 5 breaths/minute. He is given naloxone 0.4 mg IV — he wakes up within 2 minutes, is alert, and appears normal. Thirty minutes later he becomes obtunded again. The BEST explanation for his re-narcotisation is:
A. Naloxone is ineffective after first dose and should not be repeated
B. His opioid (possibly heroin or a long-acting opioid) has a longer duration of action than naloxone (30–90 min); as naloxone wears off, opioid receptor occupancy returns
C. He has developed tolerance to naloxone from prior opioid use
D. His pin-point pupils were from head injury, not opioid toxicity; the naloxone response was coincidental
Reveal Answer
Answer: B. His opioid (possibly heroin or a long-acting opioid) has a longer duration of action than naloxone (30–90 min); as naloxone wears off, opioid receptor occupancy returns
Naloxone's duration of action (30–90 minutes) is shorter than most clinically significant opioids (morphine ~4–6 h, methadone ~24–48 h, fentanyl variable but often longer than naloxone). The dramatic initial reversal confirms the opioid toxidrome was real. As naloxone is eliminated, opioid receptor occupancy returns → re-narcotisation. This is expected and well-documented — management requires repeat naloxone doses and/or an infusion, not just a single bolus and discharge.
Cardiotoxic Plants: Oleander, Cerbera odollam, Aconite, Digitalis
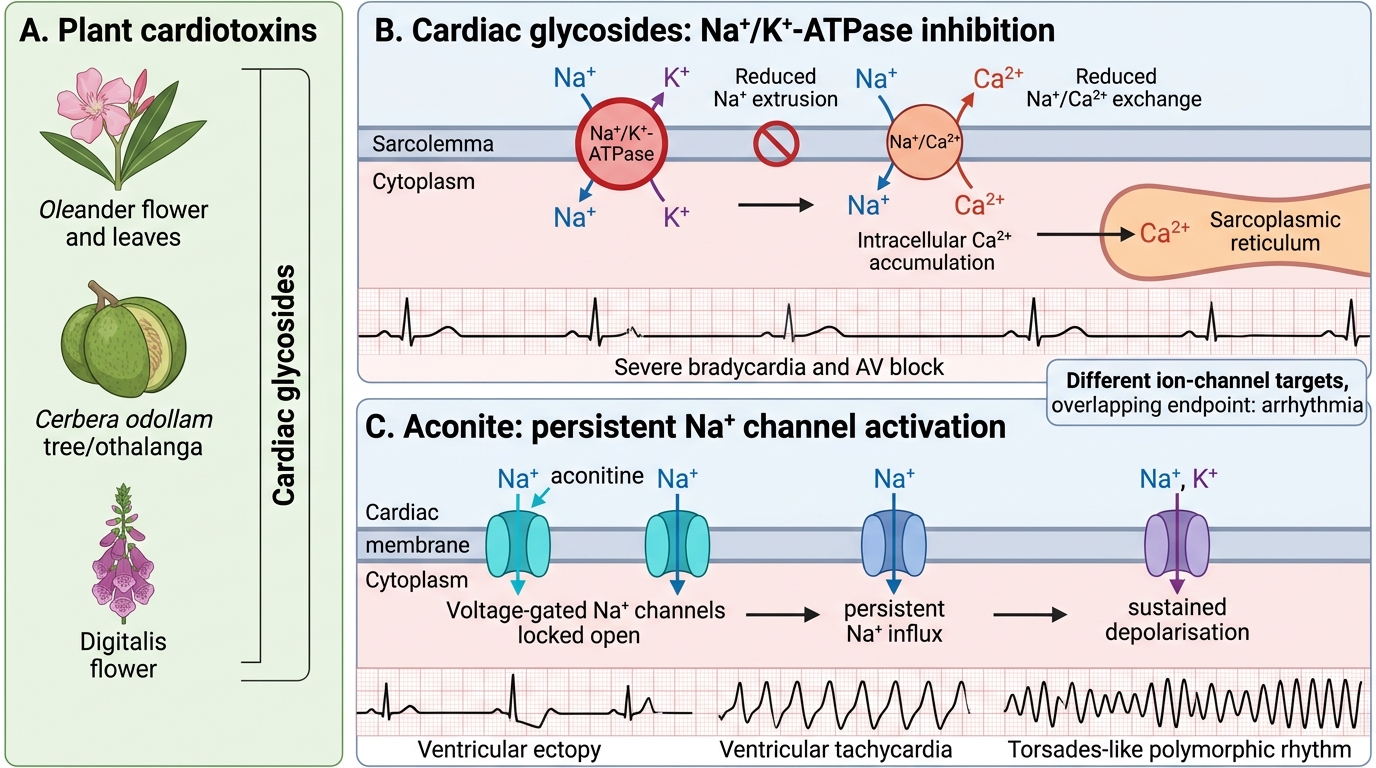
Cardiac glycoside-containing plants are among the most important causes of plant-related homicidal and suicidal poisoning in South India. Understanding their mechanism, which is identical to digoxin, is the key to understanding their clinical picture.
CARDIAC GLYCOSIDE MECHANISM (all agents below):
Cardiac glycosides inhibit the Na⁺/K⁺-ATPase pump on cardiomyocyte membranes. Loss of the transmembrane Na⁺ gradient reduces the driving force for Na⁺/Ca²⁺ exchange, leading to intracellular Ca²⁺ overload. At toxic levels: triggered arrhythmias (delayed after-depolarisations, DADs) → ventricular ectopics, bidirectional ventricular tachycardia (characteristic of digoxin/oleander toxicity) → ventricular fibrillation. Also: atrioventricular (AV) block (vagal enhancement + direct depression of AV node).
OLEANDER (Nerium oleander):
Common ornamental plant throughout India; all parts are toxic. Contains cardiac glycosides including neriine and oleandrin. A case of extreme forensic importance in South Asia — oleander is a documented suicidal and homicidal agent in rural communities. Clinical: GI symptoms first (nausea, vomiting, diarrhoea), then cardiac effects (bradycardia, AV block, ventricular arrhythmias). Similar to digoxin toxicity clinically but analytical detection requires specific oleander glycoside assays.
CERBERA ODOLLAM (the 'suicide tree'):
Cerbera odollam (pong-pong tree, 'othalanga' in Malayalam) is native to coastal Kerala and Tamil Nadu. Its kernel contains cerberin, a cardiac glycoside more potent than digoxin. Cerbera odollam poisoning is a major cause of suicidal death in Kerala. Forensically important: the fruit resembles a mango; the seed can be concealed in food. The bitter almond-like taste of the seed may be masked by spices. Cerberin is detectable by specialised LC-MS/MS analysis of gastric contents and blood.
ACONITE (Aconitum species — 'monkshood', 'wolfsbane', 'bachnak' in Hindi):
Aconite alkaloids (aconitine, mesaconitine) act differently from cardiac glycosides — they permanently activate voltage-gated Na⁺ channels (prevent channel inactivation → sustained depolarisation of nerve and cardiac cells). This causes:
- Immediate neurological effects: intense burning/tingling → numbness → paraesthesia → weakness
- Cardiac effects: ventricular arrhythmias (wide complex), AV block, cardiac arrest
- Initial oral burning sensation after ingestion → systemic onset within 20–30 min
Aconite is used as a flavouring in Ayurvedic preparations (should be processed — 'shodhita'); unprocessed aconite has been implicated in homicidal poisoning via food. No specific antidote. Treatment: supportive, cardiac monitoring, amiodarone for refractory arrhythmias.
DIGITALIS (foxglove — Digitalis purpurea/lanata):
The original source of cardiac glycosides (digitalin, digitoxin, digoxin). Digitalis leaf poisoning is rare but forensically documented. Mechanism identical to digoxin. The 'digitalis toxidrome': yellow-green visual halos ('yellow vision' — xanthopsia), nausea/vomiting, bradycardia, AV block, atrial tachycardia with block. Digoxin-specific antibody fragments (Fab antibodies — DigiFab) are the specific antidote — they bind free digoxin (and cross-react with plant cardiac glycosides including oleander) and form a complex that is renally excreted.
Cardiotoxic Plant Poisons: Ion Targets and Arrhythmias
SELF-CHECK
A 55-year-old woman from Kerala is brought in with nausea, vomiting, and severe bradycardia (HR 38 bpm) with AV block on ECG. Her daughter mentions the mother has been distressed and that there is a 'pong-pong tree' in the garden. The most appropriate specific antidote is:
A. Naloxone 0.4 mg IV
B. Digoxin-specific antibody fragments (Fab, DigiFab)
C. IV calcium gluconate
D. IV sodium bicarbonate
Reveal Answer
Answer: B. Digoxin-specific antibody fragments (Fab, DigiFab)
This is Cerbera odollam (pong-pong tree/othalanga) cardiac glycoside poisoning — bradycardia + AV block + GI symptoms + coastal Kerala setting. The mechanism is identical to digoxin (Na⁺/K⁺-ATPase inhibition). Digoxin-specific Fab antibodies (DigiFab) cross-react with plant cardiac glycosides including cerberin from Cerbera and neriine/oleandrin from oleander — they are the specific antidote for both pharmaceutical digoxin and plant cardiac glycoside poisoning. Naloxone reverses opioids. Calcium gluconate is for hypocalcaemia (and is relatively contraindicated in digoxin/cardiac glycoside toxicity as it worsens Ca²⁺ overload). NaHCO₃ is for TCA or salicylate poisoning.