Page 17 of 33
FM13.17 | Therapeutic Drug Overdose: Antipyretics, Anti-infectives & Neuropsychotropics — SDL Guide
Learning Objectives
- Describe the mechanism of toxicity, clinical features, and management of paracetamol and salicylate (aspirin) overdose
- Identify the clinical features and management of overdose with barbiturates, benzodiazepines, phenytoin, lithium, haloperidol, neuroleptics, and tricyclic antidepressants
- Apply the N-acetylcysteine (NAC) protocol for paracetamol hepatotoxicity
- Describe the forensic significance of prescription drug overdose in suicidal and homicidal poisoning
- Outline the general toxicokinetic principles applicable to drug overdose (volume of distribution, protein binding, enhanced elimination)
INSTRUCTIONS
Therapeutic drug overdose — medicines used in excess or deliberately — represents an increasingly important cause of poisoning admissions in Indian hospitals as pharmaceutical access expands. Paracetamol (ubiquitous analgesic) is the most common cause of acute liver failure from overdose in India. Neuropsychotropic drugs — particularly antidepressants, antipsychotics, and sedatives — are the agents most commonly used in deliberate self-harm. This SDL covers the forensic toxicology and clinical management principles for each of these agent classes.
References
- KSN Reddy — Essentials of Forensic Medicine & Toxicology (textbook)
- BV Subrahmanyam — Modi's Medical Jurisprudence and Toxicology (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
It is 2 am in a busy city emergency department. Three patients arrive within an hour of each other. The first: a 22-year-old who 'took all the Crocin in the house' 8 hours ago after an argument — she looks remarkably well, is alert, and has mild nausea. The second: a 45-year-old man found in his office with an empty strip of diazepam tablets, deeply sedated but maintaining his airway. The third: a 17-year-old found unconscious after drinking a solution that smelled 'like nail polish remover' — his ECG shows a wide QRS and a prolonged QTc. The first patient seems fine but is heading for liver failure in 72 hours unless you intervene now. The second will likely wake up on his own. The third needs immediate cardiac stabilisation. Three different drug classes, three completely different management priorities.
WHY THIS MATTERS
Therapeutic drug overdose is the most common form of deliberate self-harm in urban India — tablets are accessible, their lethality is perceived as 'controllable', and the cultural stigma around admission to overdose is lower than with more violent methods. Paracetamol is uniquely dangerous because the initial clinical picture is deceivingly benign — no symptoms for 24–48 hours while hepatotoxic metabolites accumulate — and many patients present late, after the treatment window has closed. The neuropsychotropic drugs (benzodiazepines, tricyclics, antipsychotics) are the commonest drug class used in deliberate self-harm. Forensic medicine graduates encounter these patients both as treating doctors and as assessors in suicidal death investigations — the medicolegal report must document drug class, estimated ingested quantity, and timing.
RECALL
Retrieve relevant Year-2 pharmacology knowledge:
- Paracetamol metabolism (biochemistry): Paracetamol is primarily glucuronidated and sulphated (90%) → excreted; a small fraction (~5–10%) is metabolised by CYP2E1 to NAPQI (N-acetyl-p-benzoquinone imine), a reactive hepatotoxic metabolite that is rapidly conjugated with glutathione → non-toxic. In overdose, glutathione stores deplete → NAPQI accumulates → centrilobular hepatic necrosis.
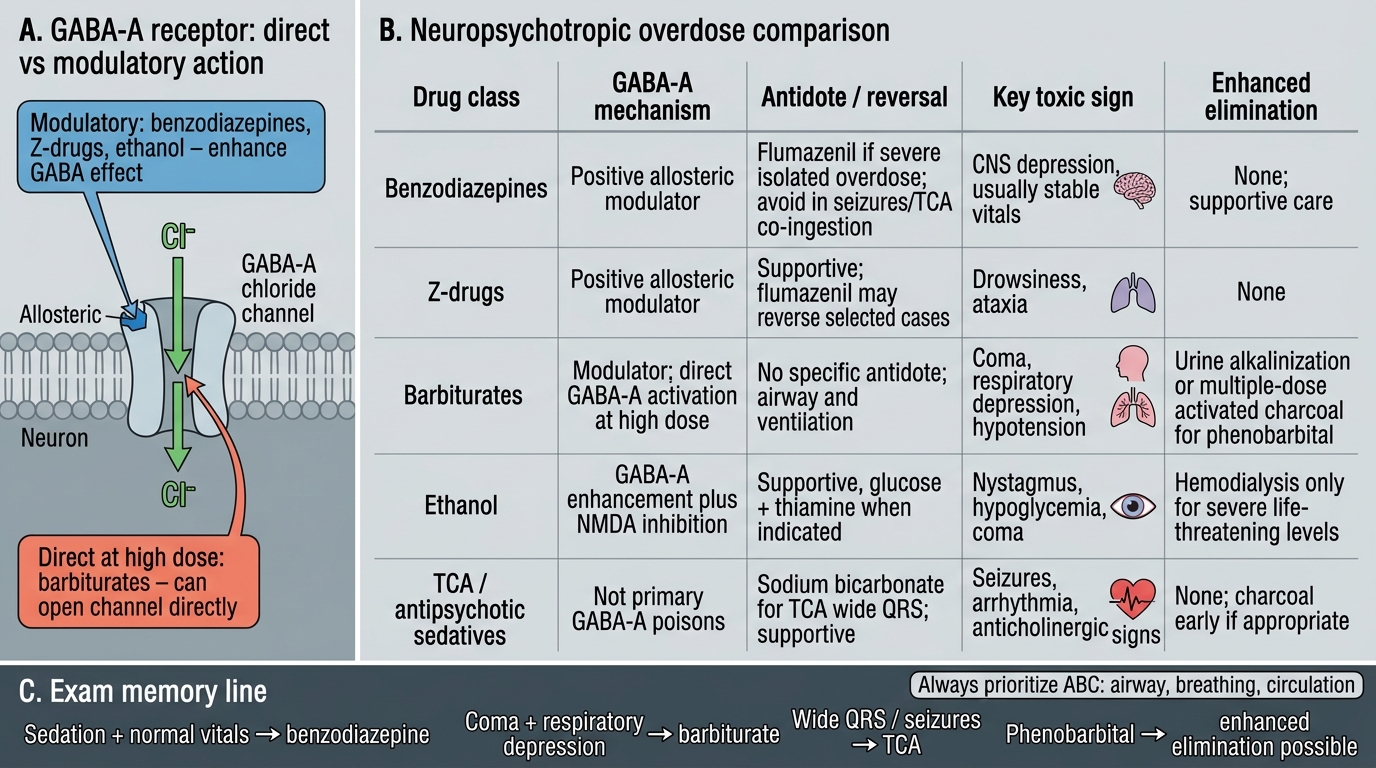
- GABA pharmacology: benzodiazepines (BZDs) act as positive allosteric modulators at the GABA-A receptor (not agonists — they enhance the effect of GABA, not replace it). Barbiturates have a similar mechanism but at higher concentrations can open Cl⁻ channels directly (no GABA required) — hence barbiturates are more lethally toxic than BZDs in overdose.
- Sodium channel pharmacology: tricyclic antidepressants (TCAs) block fast Na⁺ channels in the cardiac conduction system at toxic doses → QRS widening → ventricular arrhythmia. This is the mechanism of TCA cardiac toxicity.
- Lithium pharmacology: lithium is similar in size to Na⁺/K⁺ and distributes into cells via Na⁺ channels; it has a narrow therapeutic index (therapeutic: 0.6–1.2 mEq/L; toxic: >1.5 mEq/L).
Medicolegal Context: Prescription Drug Overdose in India
Prescription drug overdose has a distinctive medicolegal profile that differs from agricultural or industrial poisons. The key medicolegal questions in a therapeutic drug overdose case are:
- Intent — was this accidental (child ingestion of a grandparent's medications, elderly patient confused about dosing), a deliberate self-harm attempt (suicide attempt), or homicidal administration without the victim's knowledge (a documented pattern with sedatives and paracetamol in India)?
- Timing — particularly critical for paracetamol (the treatment window is narrow), for TCA cardiac effects (can develop rapidly), and for forensic estimation of when drug was taken
- Quantity and source — the empty packet/blister is forensic evidence; pharmacy records (for prescription drugs) may document dispensing pattern if overdose is suspected to be chronic
- Medical context — a patient on therapeutic lithium or warfarin may develop toxicity from a dose change, drug interaction, or renal failure; this is not 'poisoning' but is still a medicolegal event if it causes harm through negligence
The forensic categories:
- Suicidal overdose (most common): tablets are the most common mode of self-harm in urban Indian women; MLR should document the number of tablets found/missing, circumstances, prior psychiatric history
- Accidental paediatric overdose: paracetamol syrup, iron supplements — document the storage and labelling of the implicated medication
- Homicidal sedation (medication-facilitated crimes): sedative/hypnotic (benzodiazepine, antihistamine) administered to incapacitate a victim for assault, robbery, or other crimes
- Iatrogenic overdose from prescription error or dosing in renal/hepatic failure (particularly lithium, digoxin, aminoglycosides)
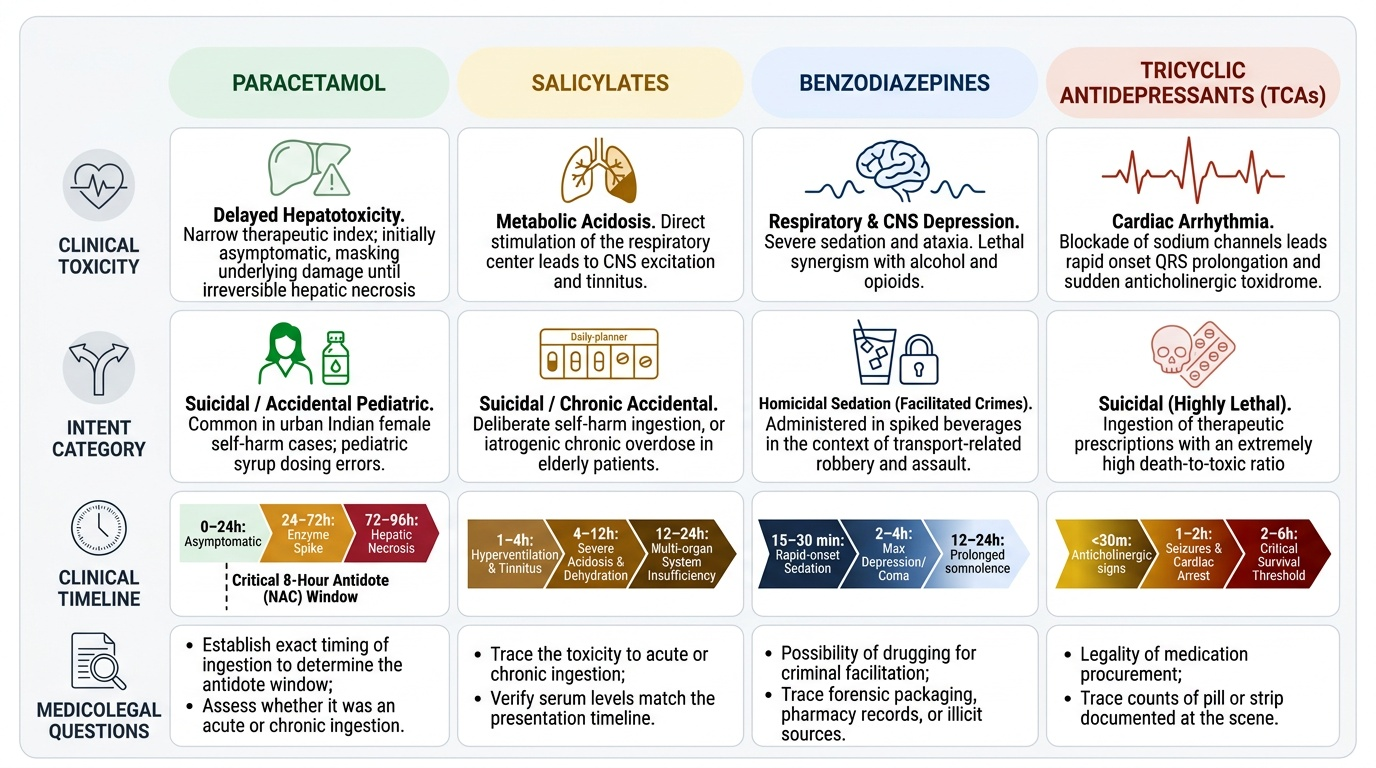
Provided image
Antipyretics: Paracetamol and Salicylates in Overdose
PARACETAMOL (acetaminophen) OVERDOSE:
Paracetamol is perhaps the most dangerous example of a 'safe-seeming' overdose. At therapeutic doses (0.5–1 g, 4-hourly, max 4 g/day), it is one of the safest analgesics. In overdose, the hepatotoxic metabolite NAPQI (formed via CYP2E1) exceeds glutathione buffering capacity.
Toxic dose: >150 mg/kg or 7.5 g single ingestion in an adult (lower in patients with induced CYP2E1: chronic alcohol, anticonvulsant therapy).
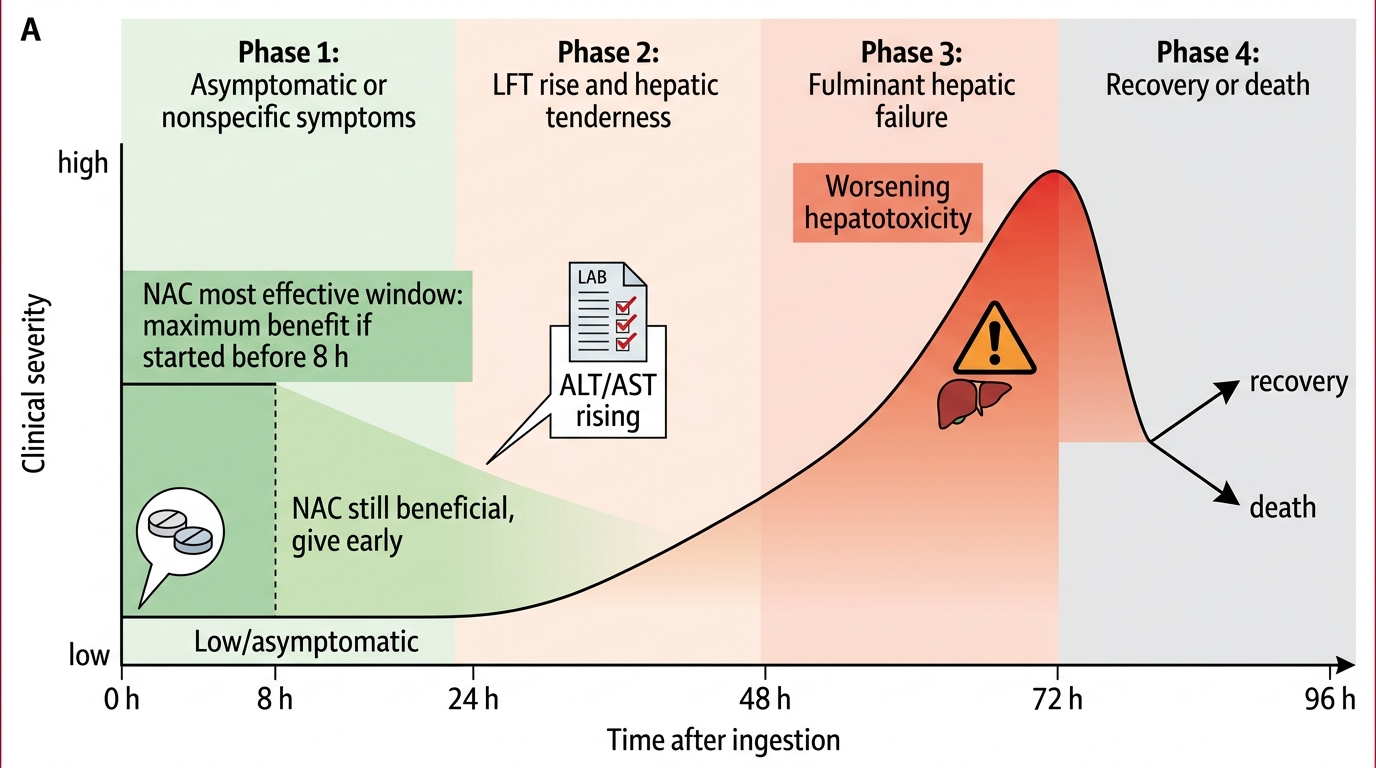
Four-phase clinical course:
Phase 1 (0–24 h): Nausea, vomiting, malaise — or may be ASYMPTOMATIC. The patient 'looks fine'. LFTs are still normal.
Phase 2 (24–72 h): Right upper quadrant pain; LFTs begin to rise (AST, ALT); INR starts to rise.
Phase 3 (72–96 h): Peak hepatotoxicity — fulminant hepatic failure; jaundice, coagulopathy, encephalopathy, hypoglycaemia, renal failure (direct tubular toxicity of NAPQI). Peak AST may exceed 10,000 IU/L. This is the potentially fatal phase.
Phase 4 (4+ days): Recovery if liver function returns, or death from fulminant hepatic failure.
Treatment — N-acetylcysteine (NAC):
NAC is the specific antidote for paracetamol toxicity. It works by:
1. Directly replenishing glutathione (the natural NAPQI scavenger)
2. Acting as a glutathione precursor
3. Providing a direct sulphhydryl group to detoxify NAPQI
Timing is critical: NAC is maximally effective within 8 hours of ingestion; still beneficial up to 24 hours; efficacy decreases beyond 24 hours but should still be given if LFTs are rising. The Rumack-Matthew nomogram plots serum paracetamol concentration against time since ingestion — readings above the treatment line mandate NAC.
NAC protocol (IV): loading dose 150 mg/kg in 200 mL 5% dextrose over 1 h → 50 mg/kg in 500 mL over 4 h → 100 mg/kg in 1 L over 16 h. Oral protocol also effective if IV unavailable.
SALICYLATE (ASPIRIN) OVERDOSE:
Covered in detail in SDL sp1-corrosives (as acetylsalicylic acid under corrosive poisons). Key recall here: biphasic acid-base disturbance (early respiratory alkalosis → metabolic acidosis); treatment: urinary alkalinisation (sodium bicarbonate — ion trapping) + haemodialysis for severe cases (serum salicylate >350 mg/L).
Four Phases of Paracetamol Poisoning
SELF-CHECK
A 20-year-old woman presents 10 hours after taking 'approximately 20 paracetamol 500 mg tablets' (total ~10 g). She is asymptomatic with no nausea. Serum paracetamol is 150 mg/L. The Rumack-Matthew nomogram for a 10-hour level of 150 mg/L places this ABOVE the treatment line. Which action is most appropriate?
A. Reassure and discharge — she is asymptomatic; toxic symptoms would have appeared by now
B. Administer IV N-acetylcysteine immediately — the nomogram reading above the treatment line mandates treatment regardless of symptoms
C. Wait 24 hours for LFTs to rise before treating — NAC has little effect before LFT elevation
D. Give activated charcoal only — NAC is not indicated at 10 hours
Reveal Answer
Answer: B. Administer IV N-acetylcysteine immediately — the nomogram reading above the treatment line mandates treatment regardless of symptoms
Paracetamol hepatotoxicity is clinically silent in Phase 1 (0–24 h) — the asymptomatic presentation does NOT mean the patient is safe. The Rumack-Matthew nomogram is the decision tool: if the serum paracetamol level at the given time post-ingestion plots above the treatment line, IV NAC must be started immediately regardless of symptoms. At 10 hours, NAC is still highly effective (maximum effect is within 8 hours, but benefit continues up to 24 hours). Waiting for LFT elevation wastes the critical treatment window. Activated charcoal may have marginal benefit at 10 hours but does NOT replace NAC.
Neuropsychotropic Drugs: Sedative-Hypnotics, Anticonvulsants and Lithium
The neuropsychotropic drug class is the most commonly implicated group in deliberate self-harm overdose in India. Each subclass has a distinctive toxidrome and specific management approach.
BARBITURATES (phenobarbitone, pentobarbitone):
Barbiturates act on GABA-A receptors but with a critical pharmacological distinction from benzodiazepines: at HIGH CONCENTRATIONS, barbiturates can open the GABA-A Cl⁻ channel DIRECTLY (without requiring GABA), unlike benzodiazepines which only modulate the receptor. This property makes barbiturate overdose more reliably lethal — they cannot be reversed by flumazenil.
Clinical: progressive CNS depression → coma; respiratory depression (the cause of death); cardiovascular depression; hypothermia. No antidote — supportive care (ventilatory support). Enhanced elimination: urine alkalinisation (for phenobarbitone — increases ionised fraction in urine, similar to salicylate) and haemodialysis for severe cases.
BENZODIAZEPINES (diazepam, alprazolam, clonazepam, lorazepam):
Benzodiazepines are GABA-A positive allosteric modulators — they CANNOT open Cl⁻ channels independently. As a result, there is a 'ceiling' to their respiratory-depressant effect in isolation (even massive BZD overdose in isolation rarely causes fatal respiratory depression in a healthy adult with a patent airway). However, combined with other CNS depressants (alcohol, opioids, barbiturates), the respiratory depression is synergistically potentiated and can be fatal.
Clinical: sedation, somnolence, ataxia, respiratory depression.
Antidote: flumazenil — a competitive BZD antagonist at the GABA-A receptor. Reverses BZD sedation rapidly (IV). Cautions: very short half-life (~1 h) vs BZD half-lives of hours to days — re-sedation may occur; requires monitoring and repeat dosing. Also contraindicated if patient is a chronic BZD user with dependence (may precipitate acute withdrawal seizures).
PHENYTOIN:
Phenytoin is an anticonvulsant used for generalised and partial seizures. Mechanism: blocks voltage-gated Na⁺ channels in the frequency-dependent (use-dependent) manner. In overdose, same Na⁺ channel blockade produces cerebellar signs (nystagmus, ataxia, dysarthria) and cardiac toxicity (cardiac conduction defects, arrhythmia) — a pattern seen at both toxic serum levels and with rapid IV injection. Therapeutic range: 10–20 mg/L. CNS toxicity begins at >20 mg/L. No specific antidote — supportive, activated charcoal, lipid emulsion for refractory cardiac toxicity.
LITHIUM:
Lithium has the narrowest therapeutic index of any commonly prescribed psychotropic (therapeutic range 0.6–1.2 mEq/L; toxic symptoms at >1.5 mEq/L; severe toxicity at >2.0 mEq/L). Lithium substitutes for Na⁺ at Na⁺ channels, causing diffuse neurotoxicity: tremor (earliest and most reliable sign), ataxia, confusion, hyperreflexia, seizures, and at extreme levels — irreversible neurological damage (cerebellar atrophy).
Lithium toxicity may be acute (overdose) or chronic (accumulation from dehydration, NSAID co-prescription, diuretics, or renal failure). Treatment: IV fluids (sodium loading promotes lithium excretion — they compete for Na⁺ channels/renal reabsorption), haemodialysis (lithium is small, water-soluble, and not protein-bound — dialysable; indicated for severe toxicity or renal failure).
Neuropsychotropic Overdose Comparison