Page 5 of 16
FM13.{6,8} | Diagnosis & General Management of Poisoning — SDL Guide
Learning Objectives
- Describe the general symptoms and principles of diagnosis of common poisonings encountered in India (FM13.6)
- Describe basic methodologies in treatment of poisoning: decontamination, supportive therapy, antidote therapy, and enhanced elimination (FM13.8)
- List specific antidotes for major poisons encountered in India with their mechanisms and critical time windows
- Match enhanced elimination methods (forced diuresis, haemodialysis, haemoperfusion) to appropriate poison classes
INSTRUCTIONS
Poisoning management is one of the highest-stakes clinical scenarios you will face — irreversible organ failure and death can occur within hours if the correct sequence of interventions is not initiated promptly. In India, organophosphate pesticides, paracetamol, corrosives, and alcohol account for the majority of emergency poisoning admissions. This module gives you the evidence-based framework for managing any acute poisoning: stabilise first, then decontaminate, then target the specific poison with an antidote, then accelerate elimination if feasible. Getting the sequence right matters — activated charcoal given to an unconscious patient without airway protection causes aspiration pneumonia, not treatment.
References
- KSN Reddy — Essentials of Forensic Medicine & Toxicology, 34th ed. (textbook)
- BV Subrahmanyam — Modi's Medical Jurisprudence and Toxicology, 24th ed. (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 16-year-old girl is brought to the emergency department by her parents. She admits to having taken 'a handful of tablets' from her mother's medicine cabinet approximately 2 hours ago. The tablets are paracetamol 500 mg — roughly 25 tablets (12.5 g). She is fully conscious, has no abdominal pain yet, and her liver function tests are currently normal. Her parents ask why she needs hospital admission if she 'seems fine.' Twelve hours later, she develops right hypochondrial pain. Twenty-four hours after ingestion, her ALT is 2,800 U/L and rising. A management decision made in the first 8 hours — specifically, whether N-acetylcysteine was started on time using the Rumack-Matthew nomogram — will determine whether she leaves the hospital with a functioning liver or requires a transplant.
WHY THIS MATTERS
Every doctor in India — from the rural PHC physician to the urban intensivist — must be able to initiate the first four hours of poisoning management. The four pillars covered in this module (decontamination, supportive care, antidotes, enhanced elimination) form a universal framework applicable to any poison, known or unknown. Critically, the timing of each intervention is as important as the intervention itself: gastric lavage after 2 hours for most poisons adds no benefit and increases aspiration risk; pralidoxime for organophosphate poisoning is ineffective if delayed beyond 24-48 hours (cholinesterase ageing). This module teaches not just what to do, but when.
RECALL
From the preceding module (tx2), you know the major toxidromes and the ADME framework. Recall that volume of distribution (Vd) predicts dialysability — low Vd = dialysable; high Vd = tissue-bound, dialysis ineffective. From Pharmacology (Year 1), you recall that activated charcoal adsorbs drugs in the GI lumen by non-specific binding, and that receptor antagonists can reverse agonist effects (the basis of naloxone for opioids). From Physiology, you know that urinary pH affects tubular reabsorption of weak acids and bases — the pharmacological basis of forced alkaline diuresis. Today we translate this knowledge into actionable management.
Clinical Diagnosis of Poisoning: History, Examination and Toxidromes
Accurate diagnosis is the prerequisite for rational management. In acute poisoning, the diagnosis must be established rapidly — often before laboratory results are available — using the clinical history, physical examination findings, and toxidrome recognition.
The history in poisoning has three components that must all be pursued simultaneously. The patient's own account (when available and reliable) gives the substance and quantity; witness and family accounts provide circumstantial context; and physical evidence from the scene (containers, blister packs, agricultural equipment) is often the most reliable source. Key history elements: alleged substance (brand name if possible), estimated quantity, route of exposure, exact time of ingestion, any first-aid measures already taken (emesis induced at home? lavage started in transit?), and the patient's past medical history (prior suicide attempts, prescribed medications, alcohol use — all modify management). In the medico-legal record, each piece of information must be attributed to its source.
On general examination, the physician assesses: level of consciousness (GCS), vital signs (temperature, pulse rate, rhythm, blood pressure, respiratory rate, oxygen saturation), pupil size and reactivity, skin colour and moisture, breath odour, and the presence of any injections marks, chemical burns, or bite wounds. Toxidrome recognition is the core diagnostic skill — see the table in SDL tx2. For common Indian poisons: organophosphate presents as cholinergic toxidrome (miosis, bradycardia, SLUDGE: Salivation, Lacrimation, Urination, Defaecation, GI cramps, Emesis — plus nicotinic muscle fasciculations and eventual paralysis); paracetamol presents with nausea/vomiting initially but no specific toxidrome — diagnosis is based on history and the nomogram; corrosives present with oral/pharyngeal burns, odynophagia, and haematemesis; opioids with the classic triad of miosis, respiratory depression, and coma; alcohol with ataxia, dysarthria, disinhibition, and in severe poisoning, respiratory depression.
Investigations in acute poisoning serve two purposes: to guide specific management (paracetamol level for NAC decision; salicylate level for alkalinisation; lithium level for haemodialysis threshold) and to detect complications (metabolic acidosis, renal failure, coagulopathy). Essential initial investigations: blood glucose (hypoglycaemia common with insulin, sulphonylureas, severe hepatic poisoning), serum electrolytes with anion gap calculation (elevated anion gap metabolic acidosis = MUDPILES: Methanol, Uraemia, Diabetic ketoacidosis, Propylene glycol, Isoniazid/Iron, Lactic acidosis, Ethylene glycol, Salicylates), arterial blood gas, ECG, liver function tests, renal function, full blood count, and coagulation profile (prothrombin time).
Decontamination: GI and External
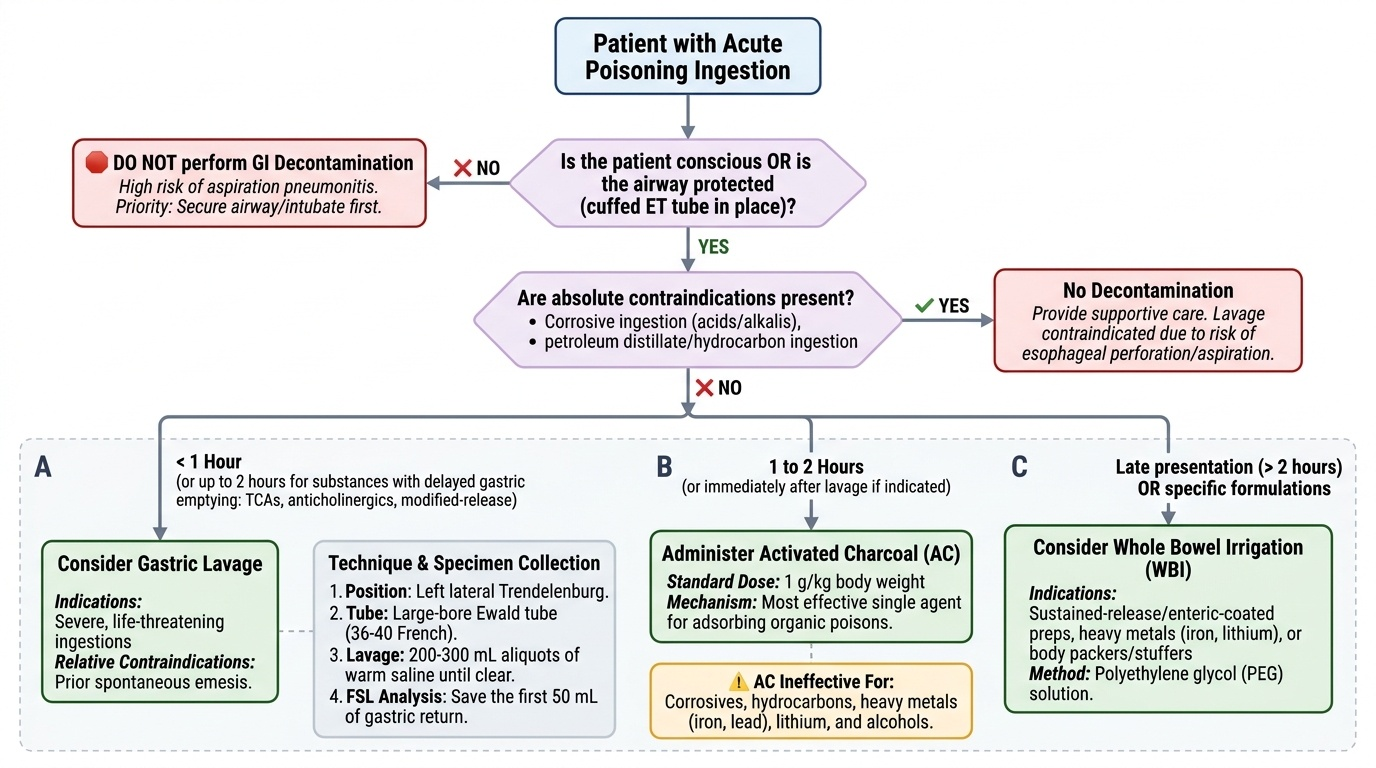
Decontamination is the process of removing or inactivating the poison before it is absorbed into the systemic circulation. External decontamination and gastrointestinal decontamination have different indications and priorities. Decontamination is a time-critical intervention — its benefit diminishes rapidly after ingestion, and its risks are constant regardless of timing.
Provided image
External decontamination is the first priority when a patient has been exposed to a poison via the skin or eyes. Contaminated clothing must be removed immediately (with appropriate personal protective equipment for the treating staff, particularly with OP pesticides which can cause secondary contamination). Skin must be irrigated copiously with large volumes of water for a minimum of 15-20 minutes — no attempt should be made to neutralise an acid burn with alkali or vice versa, as the exothermic neutralisation reaction causes additional thermal injury. Eye decontamination requires prolonged saline or water irrigation (minimum 30 minutes), and the eye must be examined for corneal injury after irrigation.
Gastric lavage is the most widely used GI decontamination technique in Indian emergency practice. Its use requires careful risk-benefit analysis. It is most effective when performed within 1 hour of ingestion (up to 2 hours for substances with delayed gastric emptying — tricyclic antidepressants, anticholinergic agents, modified-release preparations). Contraindications are critical: lavage is absolutely contraindicated in corrosive ingestion (acid or alkali — rigid lavage tube causes oesophageal perforation through already necrosed tissue) and in petroleum distillate/hydrocarbon ingestion (risk of aspiration pneumonitis). It is relatively contraindicated in an unconscious patient without a cuffed endotracheal tube in place, and should not be performed in patients who have had prior spontaneous emesis of most of the ingested material. The technique requires a large-bore Ewald tube (36-40 French), patient placed in left lateral Trendelenburg position, and 200-300 mL aliquots of warm saline instilled and drained until the return is clear — the first 50 mL of gastric contents should be saved for FSL analysis.
Activated charcoal (AC) is the most effective single GI decontamination agent for most organic poisons. The standard dose is 1 g/kg body weight (adult dose typically 50-100 g) as a slurry in water. AC works by adsorbing the poison in the GI lumen through non-specific Van der Waals binding, preventing absorption. Its benefit is greatest within 1 hour of ingestion. A critical list of substances for which AC is ineffective and should NOT be relied upon: iron, lead, lithium, alcohols (methanol, ethanol, isopropanol), strong inorganic acids, strong alkalis, potassium, cyanide, and fluoride — these substances are either not adsorbed by carbon or displace from the charcoal surface. AC must not be administered to an unconscious patient without a protected airway (aspiration of charcoal causes severe aspiration pneumonitis).
Whole bowel irrigation (WBI) uses polyethylene glycol electrolyte solution (PEG-ELS, as used for bowel preparation) administered by nasogastric tube at 1-2 L/hour until rectal effluent is clear. It is indicated for poisons not adsorbed by AC (iron tablets, sustained-release preparations, body packers with concealed drug packets), and for toxic ingestions presenting after the window for other decontamination methods.
Induced emesis with syrup of ipecacuanha has fallen out of favour and is no longer recommended in routine poisoning management — it causes prolonged vomiting that delays activated charcoal administration, and is contraindicated in unconscious patients, corrosive ingestion, and petroleum distillate ingestion. It should not be routinely used.
SELF-CHECK
A 4-year-old child swallowed iron tablets from his mother's prescription approximately 90 minutes ago. He is conscious and alert. Which decontamination approach is most appropriate?
A. Activated charcoal 1 g/kg orally — iron is well adsorbed by charcoal
B. Gastric lavage followed by whole bowel irrigation with PEG-ELS
C. Induced emesis with ipecac syrup as the first step
D. No decontamination — observe only as the child is conscious
Reveal Answer
Answer: B. Gastric lavage followed by whole bowel irrigation with PEG-ELS
Iron is one of the specific substances NOT adsorbed by activated charcoal — charcoal is contraindicated or ineffective for iron poisoning. The appropriate approach is gastric lavage (within the 2-hour window, child is conscious, and iron tablets are not corrosive) followed by whole bowel irrigation with PEG-ELS to clear unabsorbed tablets from the intestine. Induced emesis with ipecac is no longer recommended. Observation alone would be inappropriate given the significant iron ingestion.
Supportive Therapy: Stabilising the Poisoned Patient
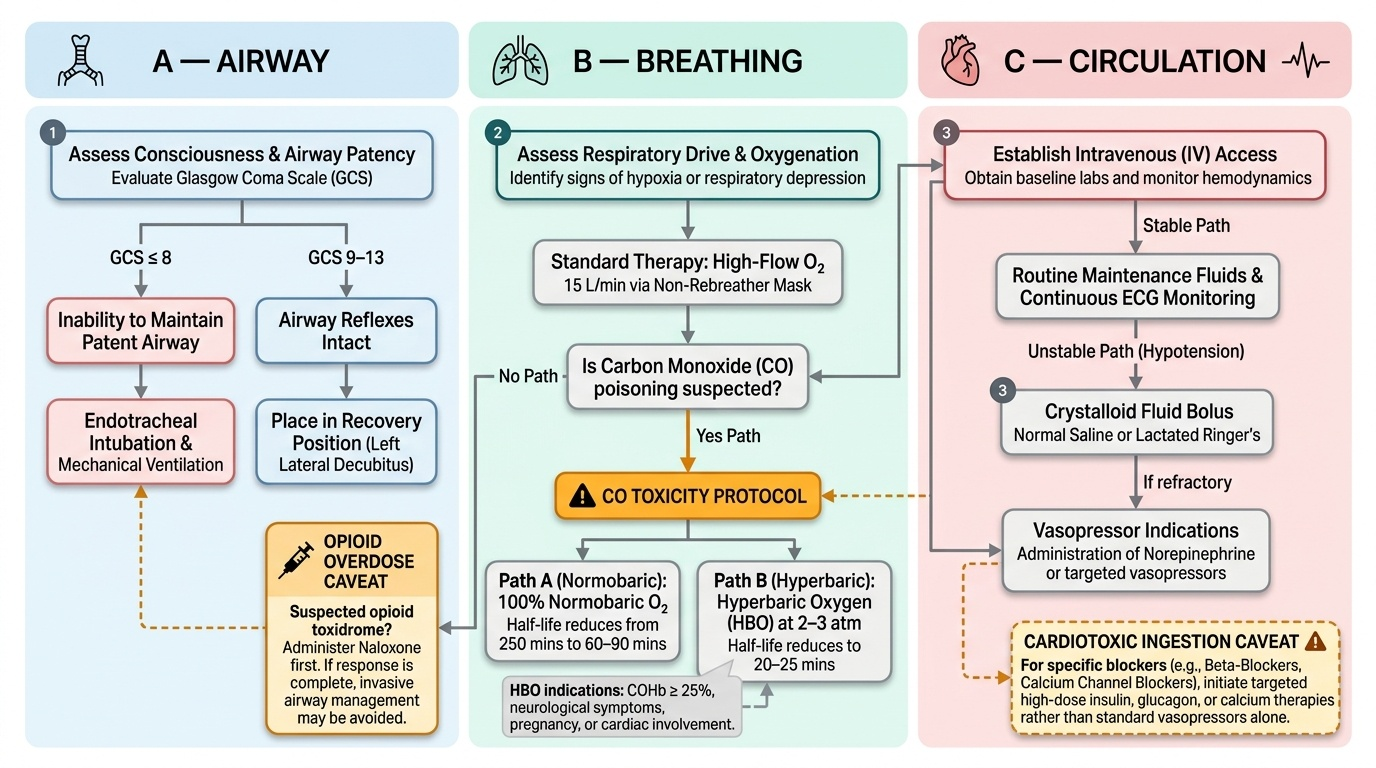
Supportive care is the backbone of poisoning management. For the vast majority of poisons — those with no specific antidote — excellent supportive care is the only treatment. Even for poisons with specific antidotes, supportive care prevents death from the immediate physiological derangements while the antidote takes effect. The approach is systematically organised around the ABC (Airway, Breathing, Circulation) framework, followed by management of specific complications.
Airway management is the first priority in any unconscious or obtunded patient. The Glasgow Coma Scale (GCS) guides decision-making: a GCS ≤8 generally indicates the inability to maintain a patent airway and protect against aspiration, requiring endotracheal intubation and mechanical ventilation. The recovery position (left lateral decubitus) is appropriate for patients with GCS 9-13 who are protecting their airway. Patients with respiratory depression from opioid overdose should first receive naloxone (see antidotes) before intubation — if the response is complete, invasive airway management may be avoided.
Breathing and oxygenation: high-flow oxygen (15 L/min via non-rebreather mask) is appropriate for most poisoning presentations. Note the important exception in CO poisoning — high-flow 100% oxygen is the definitive treatment, accelerating the elimination of carboxyhaemoglobin from 250 minutes (on room air) to approximately 60-90 minutes. Hyperbaric oxygen (HBO) at 2-3 atmospheres reduces this further to 20-25 minutes and is indicated for severe CO poisoning (carboxyhaemoglobin >25%, neurological symptoms, pregnancy, or cardiac involvement) where available.
Circulation: establish IV access immediately (two large-bore peripheral IVs). Hypotension in poisoning is managed with IV crystalloid resuscitation (500 mL bolus of 0.9% NaCl or Ringer's lactate, reassess, repeat). Vasopressors (noradrenaline, dopamine) are required when hypotension persists despite adequate fluid resuscitation — particularly relevant in tricyclic antidepressant poisoning (quinidine-like effect causing myocardial depression) and beta-blocker/calcium channel blocker overdose. Dysrhythmias are managed according to their type and the causative poison — sodium bicarbonate for TCA-induced QRS widening (sodium channel blockade reversal); magnesium sulphate for torsades de pointes (QTc prolongation); atropine for bradycardia in OP poisoning.
Seizure management: benzodiazepines (diazepam IV 0.1-0.2 mg/kg, or lorazepam) are first-line for seizures from poisoning. Phenytoin is contraindicated in cocaine, theophylline, or tricyclic antidepressant-induced seizures (worsens outcome). For refractory seizures from OP poisoning, midazolam or phenobarbital may be required.
Temperature regulation: hyperthermia from sympathomimetic or serotonin syndrome requires aggressive cooling (ice packs, cooling blankets, IV cooled fluids) as hyperthermia above 41°C causes rhabdomyolysis, disseminated intravascular coagulation, and death. Hypothermia (ethanol, sedative-hypnotics in a cold environment) requires rewarming.
Fluid and electrolyte management: aggressive IV hydration is essential for rhabdomyolysis (target urine output 1-2 mL/kg/hr), for prevention of renal failure in paracetamol poisoning, and as the vehicle for forced alkaline diuresis. Hypoglycaemia must be corrected promptly (IV dextrose 50% — 50 mL in adults, 2 mL/kg D25 in children).
Provided image