Page 12 of 16
FM13.21 | Environmental & Occupational Toxicology — SDL Guide
Learning Objectives
- Describe toxic pollution of the environment — air, water, and soil pollutants, their sources, pathways, and biological fate (FM13.21)
- Describe toxic hazards of occupation and industry — specific agents by occupation/industry with their clinical syndromes (FM13.21)
- Describe the health effects of chronic environmental and occupational toxic exposures including arsenicosis, methylmercury neurotoxicity, and occupational lung diseases (FM13.21)
- Describe the medicolegal aspects — Employees' Compensation Act 1923, occupational disease notification, environmental liability, and landmark Indian cases (FM13.21)
INSTRUCTIONS
Environmental and occupational toxicology represent the public health and legal dimensions of the subject — the harm caused not by individual poisoning events but by systematic toxic exposures affecting communities and workers over years. In India, where arsenic-contaminated groundwater affects millions in West Bengal and Assam, where bidi-rolling workers develop occupational lung disease without any single identifiable poisoning event, and where the legacy of Bhopal continues in litigation to this day, these competencies are directly relevant to the medico-legal physician, the occupational health practitioner, and the public health official. This module covers the agents, the syndromes, and the legal framework.
References
- KSN Reddy — Essentials of Forensic Medicine & Toxicology, 34th ed. (textbook)
- BV Subrahmanyam — Modi's Medical Jurisprudence and Toxicology, 24th ed. (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
In 1984, a gas leak at the Union Carbide pesticide plant in Bhopal, India, released 40 tonnes of methyl isocyanate (MIC) over a sleeping city. Within hours, over 3,000 people were dead. Over 500,000 individuals were exposed. Survivors developed chronic respiratory disease, neurological deficits, and reproductive harm. Forty years later, litigation over compensation remains active and the contaminated groundwater around the plant site continues to cause disease. The Bhopal disaster is the largest industrial chemical disaster in history, and it is an Indian story. Every physician who will practise in India carries a professional obligation to understand the legal and medical framework that governs industrial toxic exposure — because the next Bhopal may be smaller, quieter, and happening right now in a mine, a battery factory, or a field, without anyone calling it a disaster.
WHY THIS MATTERS
Environmental and occupational toxicology are not peripheral to the FM curriculum — they represent the interface between toxicology, public health law, and compensatory justice. The physician who can identify occupational lead poisoning in a battery-factory worker, document the clinical findings correctly, and navigate the Employees' Compensation Act 1923 is performing a medico-legal function as important as any autopsy. The physician who can assess an arsenic-affected community, determine the exposure pathway, and produce evidence for regulatory action is protecting thousands of lives with a single report. Understanding these responsibilities begins with knowing the agents, the exposures, and the law.
RECALL
From SDL tx2 (Classification and Toxicokinetics), you recall that metals are classified as mineral poisons (by origin) and are predominantly irritant or systemic toxins (by action). You recall that volume of distribution and renal clearance govern metal elimination, and that AAS (SDL tx5) is the definitive quantitative analytical method for metals. From Pathology (Year 2), you have begun studying chronic inflammatory and fibrotic tissue changes. Today we integrate these foundations to understand how chronic low-dose environmental and occupational toxic exposures produce the insidious, progressive multi-organ syndromes that are the hallmark of this subject area.
Toxic Pollution of the Environment: Air, Water and Soil
Environmental toxic pollution represents the contamination of natural media — air, water, and soil — with substances that cause harm to living organisms at concentrations normally present in a contaminated environment. Unlike acute poisoning events, environmental toxic exposure is typically chronic, low-dose, widespread, and disproportionately borne by populations with the least economic and political power to respond.
Air pollutants with direct human toxicity include both products of combustion and industrial emissions. Carbon monoxide (CO) is the most common cause of poisoning death from air pollution, produced by incomplete combustion of organic material in enclosed spaces (kerosene stoves, charcoal fires, diesel generators, vehicle exhaust in poorly ventilated garages). At ambient concentrations it causes chronic neurological symptoms — headache, cognitive impairment, fatigue — that may be mistaken for viral illness. Sulphur dioxide (SO₂) and nitrogen oxides (NOₓ) from industrial combustion and vehicle exhaust cause respiratory tract irritation, exacerbate asthma, and contribute to acid rain. Lead was historically emitted from leaded petrol exhaust — now phased out in India (unleaded petrol since 2000) — but continues to be released from battery smelting operations and lead-glazed pottery. Particulate matter (PM₂.₅) carries adsorbed polycyclic aromatic hydrocarbons (PAHs) and metals into the lung alveoli; chronic PM₂.₅ exposure is linked to lung cancer, cardiovascular disease, and neurodevelopmental effects in children.
Water pollutants causing significant morbidity in India include: arsenic in groundwater — the most important water-borne toxin in India. The Gangetic plains of West Bengal, Bihar, and Assam overlie geological formations where arsenic-rich pyrite deposits leach inorganic arsenic into tube-well water under reducing conditions. An estimated 10-20 million people in West Bengal and 6 million in Assam drink water with arsenic above the WHO guideline value of 10 µg/L (the Indian BIS standard is 50 µg/L as a provisional tolerance). Fluoride in groundwater — Rajasthan, Andhra Pradesh, and parts of Tamil Nadu have naturally fluoride-rich groundwater; chronic ingestion above 1.5 mg/L causes dental fluorosis (brown mottling and pitting of enamel); above 4 mg/L causes skeletal fluorosis (osteosclerosis, ligament calcification, crippling deformity). Lead in drinking water from old lead service pipes (a legacy infrastructure problem in urban India). Methylmercury in aquatic food chains — bacterial methylation of inorganic mercury in anaerobic sediments produces methylmercury, which bioaccumulates with each trophic level. The Minamata disease outbreak in Japan (1950s-1970s) — neurological devastation in coastal fishing communities caused by methylmercury discharged from the Chisso chemical plant — is the defining case in environmental toxicology. Methylmercury crosses the blood-brain barrier and the placenta, causing severe fetal neurotoxicity even when maternal symptoms are mild.
Soil pollution in India is dominated by persistent organochlorine pesticides (DDT, lindane/BHC, chlordane, endrin) that were heavily used in agriculture and malaria vector control programs. Although most are now banned or restricted under the Stockholm Convention (to which India is a signatory), their extreme lipid solubility and resistance to metabolic degradation means they persist in soil for decades and bioaccumulate through the food chain — from contaminated soil to earthworms to poultry to human adipose tissue. The phenomenon of biomagnification means that top predators (including humans) accumulate concentrations many times higher than ambient soil levels.
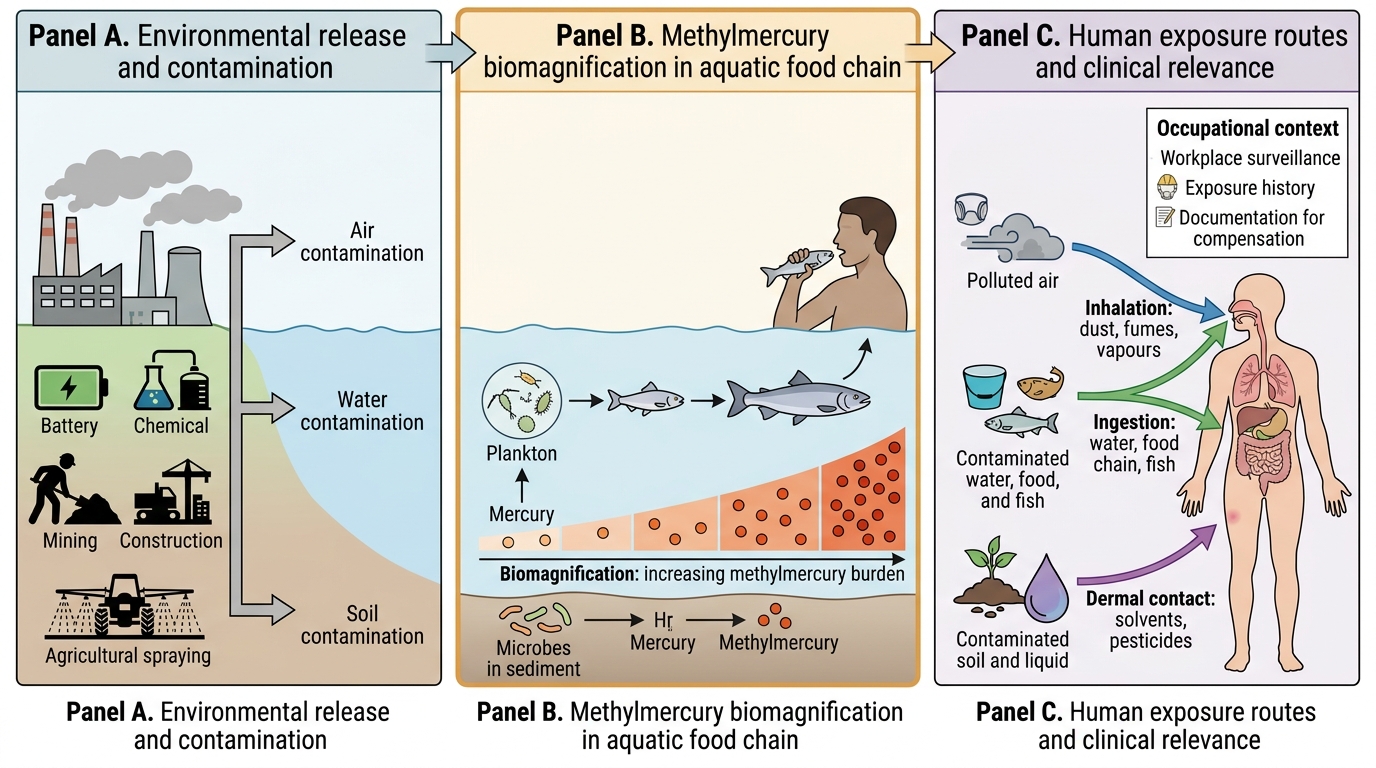
Environmental Toxin Pathways and Methylmercury Biomagnification
Occupational Toxic Hazards: Industry-Specific Exposures
Occupational toxicology addresses the health hazards arising from exposure to toxic substances in the workplace. In India, with its enormous informal industrial sector, millions of workers in battery manufacturing, chemical production, agricultural application, construction, and mining are exposed to toxic agents with limited regulatory oversight and variable personal protective equipment compliance. The physician's role is to recognise the occupational exposure pattern, diagnose the toxicological syndrome, document it for compensation purposes, and contribute to surveillance data.
The following are the major industry-specific hazards in the Indian context:
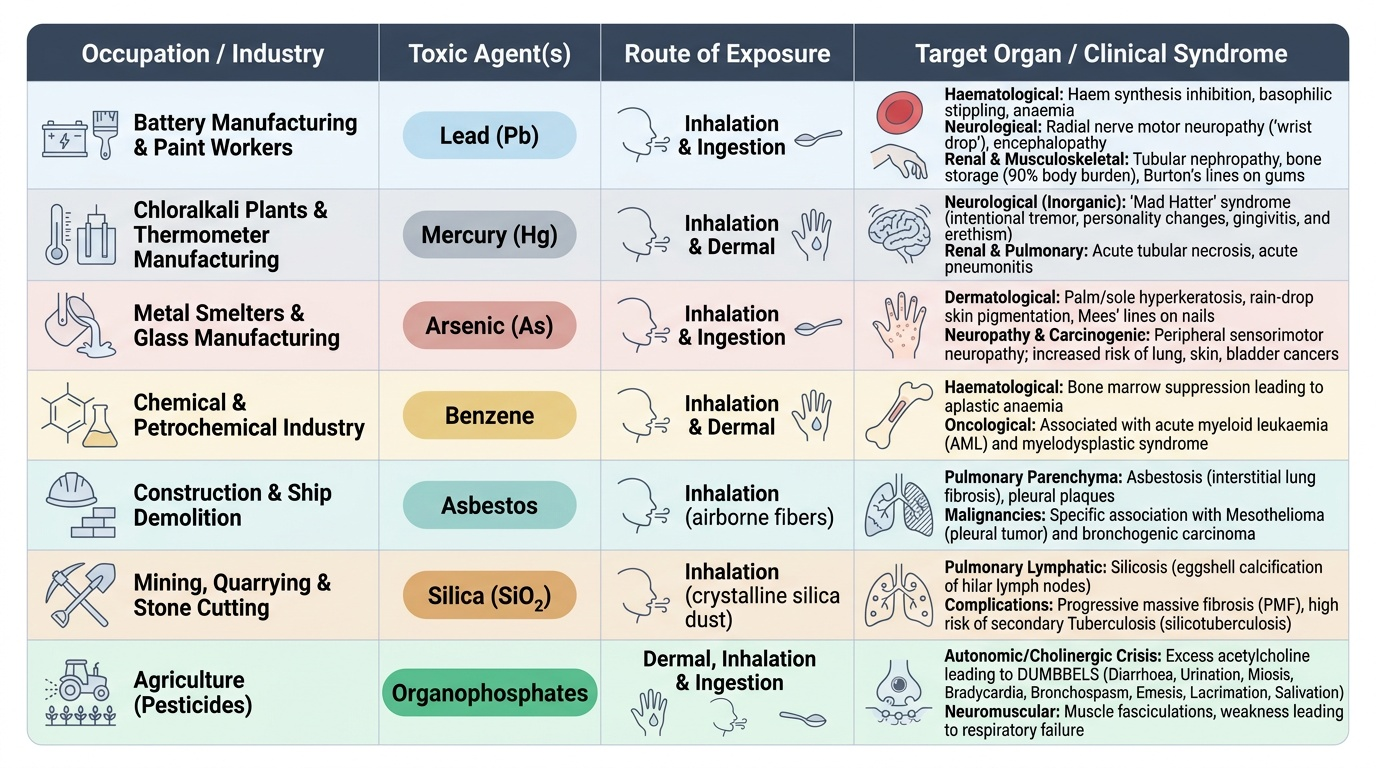
Lead (Pb): occupational lead exposure occurs in battery manufacturing workers (the largest single source in India), lead smelters, lead-paint workers, plumbers and pipe fitters (joining lead solder), and printing industry workers (historically). Lead is absorbed primarily by inhalation of lead dust/fume (occupational) and by ingestion. It is stored in bone (90% of body burden; half-life ~27 years), from which it can be remobilised during pregnancy, acidosis, or hypocalcaemia. Inorganic lead toxicity: haematological (inhibits haem synthesis — basophilic stippling on blood film; anaemia); neurological (peripheral motor neuropathy — 'wrist drop' from radial nerve involvement; encephalopathy in severe cases); renal (tubular nephropathy); and in children, cognitive impairment at blood lead levels as low as 5 µg/dL (no safe threshold). Radiologically, lead lines (dense metaphyseal bands) in children's long bones and lead lines on the gums (Burton's lines — blue-black discolouration of the gingival margin) are classic clinical signs.
Mercury: occupational mercury exposure occurs in chloralkali plants (producing chlorine and caustic soda using mercury electrolytic cells), thermometer and barometer manufacturing, gold amalgam processing (artisanal small-scale gold mining), fluorescent lamp manufacturing, and dental amalgam preparation. Inorganic mercury (vapour or dust) primarily causes neurological ('Mad Hatter' syndrome — intentional tremor, personality change, gingivitis — erethism); renal; and pulmonary toxicity. Organic methylmercury (Minamata disease) — primarily from dietary fish consumption in contaminated areas — causes severe cerebellar ataxia, constriction of visual fields, sensorineural hearing loss, and fetal neurological catastrophe.
Arsenic: occupational exposure in smelter workers (arsenic is a contaminant of copper, lead, and gold ores), pesticide production workers, wood preservative (CCA) workers, and semiconductor industry. Arsenic accumulates in hair, nails, and bone. Chronic arsenic poisoning (arsenicosis) — covered in the next section.
Benzene: occupational exposure in rubber and chemical industry workers, shoe manufacturing (solvent exposure), petroleum refinery workers, and laboratories using benzene as a solvent. Benzene is an established Group 1 carcinogen — chronic exposure causes bone marrow toxicity (aplastic anaemia; acute myeloid leukaemia, AML). Short-term exposure causes CNS depression, skin/mucous membrane irritation. The haematological effect is the primary occupational health concern: workers exposed above the permissible exposure limit (1 ppm TWA) require regular complete blood counts.
Asbestos: occupational exposure in construction workers (ceiling board, roof sheet installation), shipbuilding, insulation installation, and brake-lining manufacturing. Two principal asbestos types: chrysotile (white asbestos — most commonly used globally, less carcinogenic) and crocidolite (blue asbestos — now banned; most potently carcinogenic). Asbestos fibres deposited in lung alveoli and pleura cause: asbestosis (progressive pulmonary fibrosis — exposure-dose dependent); pleural plaques (calcified fibrohyaline lesions — marker of asbestos exposure, rarely symptomatic); mesothelioma (malignant tumour of the pleural or peritoneal mesothelium — pathognomonically linked to crocidolite asbestos; latency 20-40 years; no safe threshold of exposure; median survival 12-18 months after diagnosis).
Silica: occupational exposure in miners (coal, gold, granite, stone quarrying), stone cutters, sandblasters, and ceramic/glass workers. Crystalline silica (quartz, cristobalite) — but NOT amorphous silica — causes silicosis: progressive nodular pulmonary fibrosis with characteristic rounded opacities on chest X-ray (upper lobe predominance). Silicosis predisposes to tuberculosis (a lethal synergy: 'silicotuberculosis') and is a Group 1 carcinogen for lung cancer.
Organophosphate pesticides in agricultural workers — acute poisoning as the dominant occupational health risk in rural India (see SDL tx3). Chronic low-level OP exposure causes delayed peripheral neuropathy (OPIDN — organophosphate-induced delayed neuropathy) affecting large motor fibres.
Provided image
SELF-CHECK
A 45-year-old male battery-factory worker presents with bilateral foot drop and wrist drop, anaemia, and abdominal colic. Blood film shows basophilic stippling. Which toxic agent is most likely, and which clinical sign differentiates this from other peripheral neuropathies?
A. Mercury poisoning; intentional tremor (erethism) differentiates it from other causes
B. Organophosphate poisoning; SLUDGE symptoms are the differentiating feature
C. Lead poisoning; motor neuropathy (foot drop/wrist drop) with basophilic stippling on blood film is the distinguishing combination
D. Arsenic poisoning; Mees lines on fingernails differentiate it from other neuropathies
Reveal Answer
Answer: C. Lead poisoning; motor neuropathy (foot drop/wrist drop) with basophilic stippling on blood film is the distinguishing combination
Battery-factory worker + motor peripheral neuropathy (wrist drop = radial nerve; foot drop = peroneal) + anaemia + abdominal colic + basophilic stippling on blood film = lead poisoning. Basophilic stippling on blood film (aggregated ribosomal RNA in red cells, because lead inhibits pyrimidine 5'-nucleotidase) is the hallmark haematological finding. Mercury causes intentional tremor and erethism — not motor neuropathy or basophilic stippling. Organophosphate causes cholinergic toxidrome, not peripheral motor neuropathy. Arsenic causes mixed sensorimotor neuropathy, not predominantly motor with basophilic stippling.
Health Effects of Chronic Environmental Toxic Exposure
Chronic environmental toxic exposures produce insidious, progressive syndromes that develop over years rather than hours. Their clinical recognition requires a high index of suspicion and systematic examination, because early features are non-specific and the exposure history may not be volunteered by the patient.
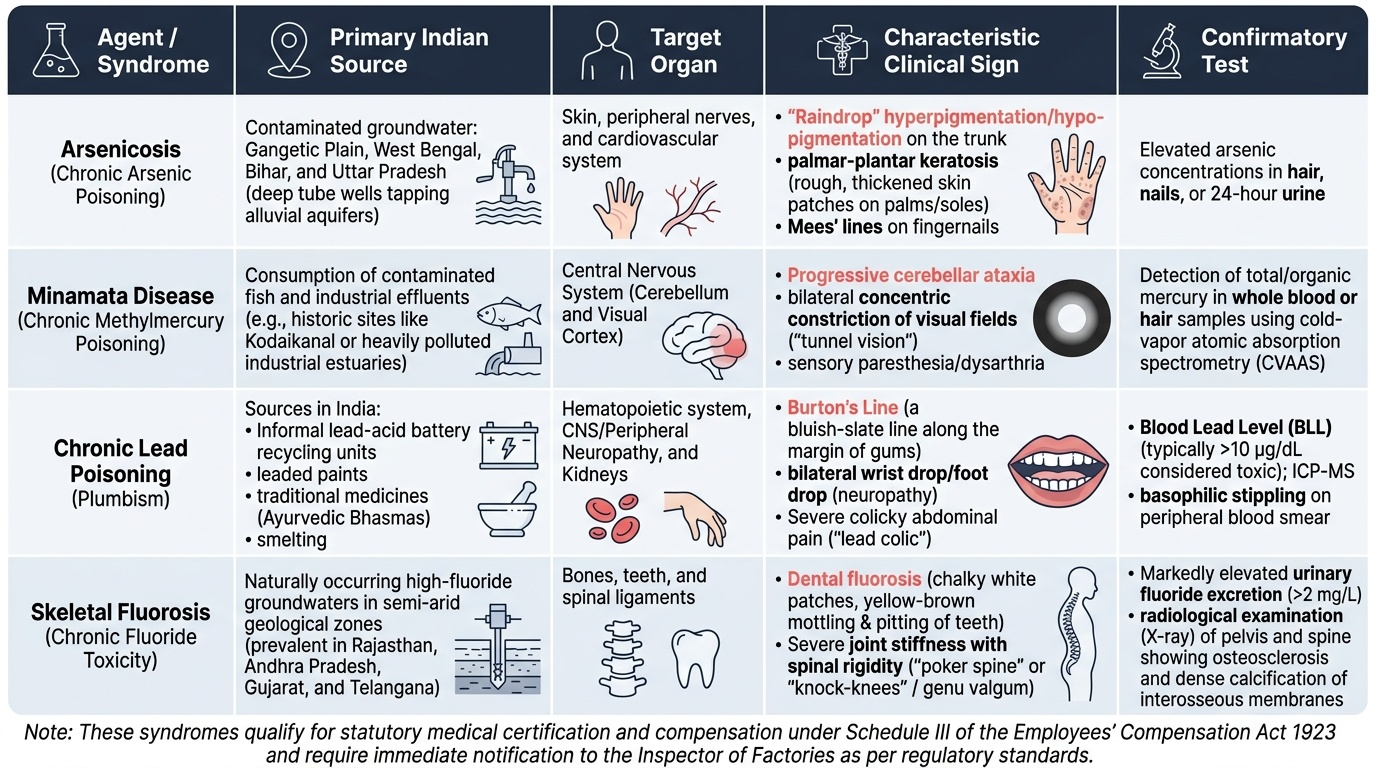
Arsenicosis (chronic arsenic poisoning): the dominant environmental toxin in large parts of India. Clinical features develop after years of exposure to arsenic above 50 µg/L in drinking water:
- Skin changes (the most specific clinical feature): melanosis (hyperpigmentation — 'rain-drop on dusty road' pattern on trunk and extremities); keratosis (hyperkeratosis — hard, rough, 'shotgun pellet' nodules on the palms and soles); leucomelanosis (alternating hyperpigmented and depigmented areas); Bowen's disease (in-situ squamous carcinoma of the skin — arsenical in origin)
- Peripheral neuropathy: predominantly sensory ('stocking-glove' distribution), mixed sensorimotor in advanced cases
- Mees lines: transverse white lines across all nails — a useful clinical sign of acute/subacute arsenic exposure (each line corresponds to a period of heavy exposure; nail growth rate ~1 mm/week allows approximate dating)
- Vascular disease: Blackfoot disease (peripheral vascular occlusion — described in Taiwan; less common in India) and Raynaud phenomenon
- Internal malignancies: bladder cancer, lung cancer, and hepatocellular carcinoma are significantly elevated in arsenic-exposed populations
- IARC classification: arsenic is a Group 1 carcinogen for lung, bladder, and skin cancer
Methylmercury neurotoxicity (Minamata disease): the clinical syndrome from organic methylmercury exposure — whether occupational, dietary (contaminated fish), or accidental:
- Cerebellar signs: ataxia (truncal and limb), dysarthria, dysdiadochokinesia
- Sensory disturbance: circumoral (perioral) and distal extremity paraesthesia — bilateral and symmetric
- Visual field constriction: concentric narrowing of visual fields (tunnel vision) — a characteristic feature distinguishing Minamata disease from other cerebellar disorders
- Sensorineural hearing loss
- Fetal Minamata disease (congenital methylmercury poisoning): severe neurological catastrophe — cerebral palsy, mental retardation, seizures, hypotonia — in infants born to mothers with relatively mild symptoms, because methylmercury crosses the placenta with high efficiency and the developing brain is exquisitely sensitive
Chronic lead poisoning: blood lead level (BLL) >10 µg/dL in children is associated with cognitive impairment, reduced IQ, attention deficit, and antisocial behaviour; no safe threshold has been established for neurodevelopmental effects. Burton's lines (blue-black lead sulphide deposits at the gingival margin), basophilic stippling of red cells, normochromic normocytic or hypochromic microcytic anaemia (lead inhibits haem synthesis), and motor peripheral neuropathy in adults. Radiological findings: lead lines at the metaphyses of long bones (dense transverse bands from lead phosphate deposition).
Skeletal fluorosis: chronic fluoride ingestion above 4 mg/L for >10 years causes: dental fluorosis (mottling, brown staining, pitting of enamel — cosmetic and structural compromise); skeletal fluorosis (osteosclerosis of spine and pelvis, calcification of interosseous membranes and ligaments, crippling 'poker spine'). Endemic in Rajasthan, Gujarat, Andhra Pradesh, and parts of Tamil Nadu. The diagnosis is clinical and confirmed by serum and urine fluoride levels and X-ray findings.
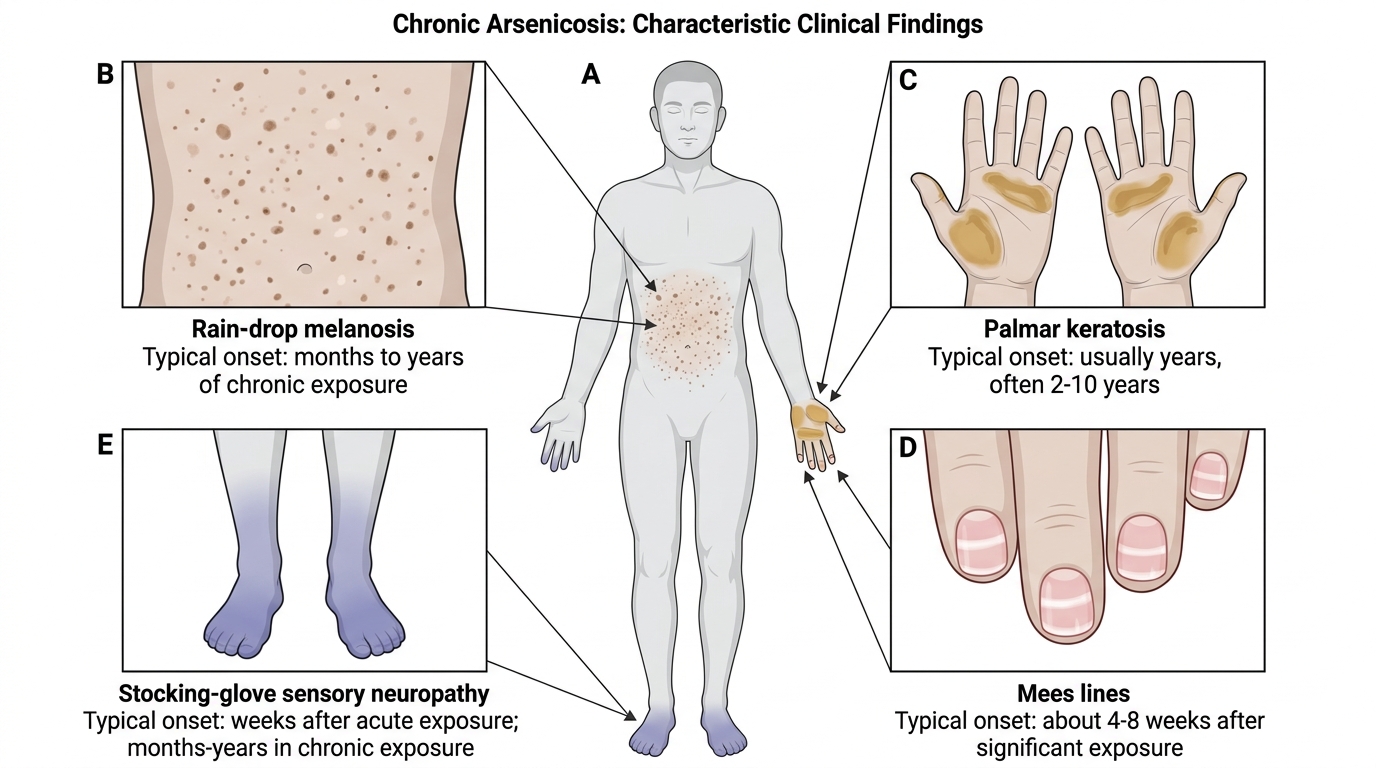
Clinical Findings in Arsenicosis
Medicolegal Aspects: Compensation, Notification and Legal Liability
The medicolegal framework governing environmental and occupational toxicology in India encompasses worker compensation, occupational disease notification, environmental protection law, and civil/criminal liability for industrial pollution. A physician practising in occupational health, community medicine, or forensic medicine must be conversant with the primary statutes.
Employees' Compensation Act 1923 (formerly Workmen's Compensation Act — amended and renamed): provides mandatory compensation to employees for injuries and occupational diseases arising out of and in the course of employment. Schedule III of the Act lists specific occupational diseases for which compensation is payable without the employee having to prove negligence — these include: occupational lung diseases (silicosis, asbestosis, pneumoconiosis), occupational skin diseases (contact dermatitis from industrial chemicals), lead poisoning, mercury poisoning, arsenic poisoning, and poisoning from other specified substances. The physician's role is critical: the occupational disease must be medico-legally certified by a qualified physician with documentation of the occupational exposure history, clinical examination findings, and relevant investigations (e.g., blood lead level, chest X-ray, spirometry).
Factories Act 1948 places obligations on factory occupiers to prevent occupational disease: provision of personal protective equipment, periodic medical examination of workers in specified hazardous processes, maintenance of health records, and notification of occupational diseases to the Inspector of Factories. Mines Act 1952 applies the equivalent framework to mining operations. Non-compliance is a criminal offence.
Environment Protection Act 1986 is the umbrella legislation governing environmental pollution in India. It empowers the Central Government to set standards for emission and discharge of pollutants. The Central Pollution Control Board (CPCB) and State Pollution Control Boards (SPCBs) are the regulatory bodies for industrial air and water discharge. Section 15 of the Act provides for criminal liability (imprisonment up to 5 years + fine) for violations of emission standards. Industrial units causing environmental pollution may also face civil liability in tort (public nuisance, negligence causing damage to persons).
Bhopal Gas Tragedy (1984) — medicolegal significance: the Union Carbide India Limited (UCIL) plant in Bhopal released methyl isocyanate (MIC), causing the largest industrial chemical disaster in history. Medico-legal lessons: (1) the right to know principle — communities have a right to information about hazardous substances in their vicinity; (2) precautionary principle — industrial operators must implement safeguards proportionate to the worst-case hazard, not just routine operations; (3) polluter pays principle — the responsible corporation is liable for remediation and compensation; (4) corporate criminal liability — the long-running debate over whether Union Carbide and its executives could be held criminally accountable under Indian law tested the limits of corporate liability doctrine; (5) adequacy of compensation — the 1989 settlement of US$470 million has been widely criticised as grossly inadequate given the scale of harm, and litigation continues. The Bhopal case drove major reforms in Indian industrial safety regulation and the Environment Protection Act 1986.
Consumer Protection Act 2019 allows workers and community members to seek redress for 'deficient services' causing harm — this has been extended in case law to industrial entities whose pollution caused identifiable harm to identifiable individuals. NMC Act 2020 requires physicians to report occupational diseases to relevant health authorities where mandated — failure to do so can constitute professional misconduct.
Provided image
Key legislation summary:
• Employees' Compensation Act 1923 — Schedule III occupational diseases; compensation without proof of negligence
• Factories Act 1948 — occupational safety obligations; notification of occupational disease to Factories Inspector
• Mines Act 1952 — same framework for mining sector
• Environment Protection Act 1986 — CPCB/SPCB regulation; criminal liability Section 15; Bhopal-driven reforms
• Stockholm Convention — India signatory; phase-out of persistent organic pollutants (DDT, lindane, PCBs)
CLINICAL PEARL
The mesothelioma latency trap in asbestos claims: A key medico-legal challenge in asbestos-related disease is the 40-year latency between first asbestos exposure and mesothelioma development. A construction worker first exposed to asbestos at age 25 in 1980 develops mesothelioma in 2020 at age 65 — when the original employer may no longer exist, records of workplace exposure may be unavailable, and the statute of limitations may have elapsed under strict application. Indian courts have extended the limitation period in latent occupational disease cases (the 'discovery rule' — the limitation period begins when the patient discovers the disease and its cause, not at the time of exposure). The physician's documentation of the occupational exposure history — specifically naming the employer, the dates of employment, the nature of the work, and the type of asbestos material handled — is the primary evidence the claimant can use to establish liability decades later. A well-documented occupational history written in 2024 may be the pivotal evidence in a 2050 mesothelioma compensation claim.
SELF-CHECK
A bidi-factory worker in West Bengal has been rolling beedis for 20 years in a poorly ventilated room. She now has progressive breathlessness, Mees lines on her nails, and skin melanosis with palmar keratosis. What is the most likely diagnosis, and which Act provides her the right to compensation without proving employer negligence?
A. Asbestosis; Factories Act 1948
B. Arsenicosis from contaminated drinking water; Environment Protection Act 1986
C. Silicosis; Employees' Compensation Act 1923 Schedule III
D. Chronic OP poisoning; Mines Act 1952
Reveal Answer
Answer: B. Arsenicosis from contaminated drinking water; Environment Protection Act 1986
Mees lines + skin melanosis + palmar keratosis = arsenicosis (chronic arsenic poisoning). West Bengal is an arsenic-endemic region where groundwater contamination is the primary exposure route. Bidi rolling itself does not involve asbestos, silica, or OP pesticides. The arsenic exposure is environmental (drinking water), not occupational. However, arsenicosis is a listed occupational disease in Schedule III of the Employees' Compensation Act 1923 when the exposure is occupational. In this case, the exposure is environmental — she may pursue compensation through civil litigation under the Environment Protection Act 1986 or file a complaint with the SPCB. The correct answer notes arsenicosis as the diagnosis and Environment Protection Act 1986 as the relevant statute for environmental (non-occupational) arsenic exposure.
SELF-CHECK
Methylmercury poisoning (Minamata disease) produces a neurological syndrome that differs from inorganic mercury poisoning. Which feature is MOST characteristic of methylmercury neurotoxicity specifically?
A. Peripheral motor neuropathy with wrist drop and basophilic stippling
B. Intentional tremor, erethism (personality change), and gingivitis
C. Constriction of visual fields, cerebellar ataxia, and circumoral paraesthesia
D. Renal tubular dysfunction and Fanconi syndrome
Reveal Answer
Answer: C. Constriction of visual fields, cerebellar ataxia, and circumoral paraesthesia
Constriction of visual fields (concentric tunnel vision), cerebellar ataxia, and circumoral paraesthesia are the hallmark features of methylmercury (organic mercury) neurotoxicity — the Minamata disease syndrome. These features reflect the high affinity of methylmercury for the visual cortex and cerebellar granule cells. Intentional tremor + erethism + gingivitis = inorganic mercury vapour poisoning (occupational — 'Mad Hatter' syndrome). Peripheral motor neuropathy + basophilic stippling = lead poisoning. Renal tubular dysfunction (Fanconi syndrome) is associated with cadmium (Itai-itai disease) and inorganic mercury nephropathy, not methylmercury.
KEY TAKEAWAYS
Environmental toxins causing significant morbidity in India: air — CO (combustion, enclosed spaces); SO₂/NOₓ (industrial/vehicle emissions); water — arsenic in groundwater (West Bengal, Assam — millions exposed; WHO guideline 10 µg/L; India BIS 50 µg/L provisional); fluoride (Rajasthan, AP — dental + skeletal fluorosis above 4 mg/L); methylmercury (aquatic food chain biomagnification — Minamata disease prototype); soil — persistent organochlorine pesticides (DDT, lindane — bioaccumulate, lipid-soluble, banned/restricted).
Occupational hazards by industry: battery workers/smelters → lead (wrist drop, basophilic stippling, Burton's lines, radiological lead lines in children); chloralkali/thermometer → mercury (inorganic: erethism, tremor, gingivitis; organic methylmercury: cerebellar ataxia, tunnel vision, circumoral paraesthesia, fetal catastrophe); chemical/rubber industry → benzene (Group 1 carcinogen; aplastic anaemia, AML); construction/shipbuilding → asbestos (chrysotile < crocidolite in carcinogenicity; asbestosis, pleural plaques, mesothelioma — 40-year latency); mining/stone-cutting → silica (silicosis — nodular fibrosis upper lobe; predisposes to TB).
Chronic syndromes: arsenicosis (melanosis, palmar keratosis, Mees lines, sensorimotor neuropathy, bladder/lung/skin cancer); Minamata disease (cerebellar ataxia, constricted visual fields, circumoral paraesthesia); chronic lead (cognitive impairment in children at any BLL, Burton's lines, motor neuropathy in adults); skeletal fluorosis (osteosclerosis, poker spine).
Legal framework: Employees' Compensation Act 1923 (Schedule III — compensation without proving negligence for listed occupational diseases); Factories Act 1948 / Mines Act 1952 (worker safety obligations, notification); Environment Protection Act 1986 (CPCB/SPCB regulation, Section 15 criminal liability); NMC Act 2020 and CPA 2019 (physician reporting duties, professional accountability). Bhopal 1984: landmark case for right-to-know, precautionary principle, polluter-pays doctrine.
REFLECT
You are a junior resident in a district hospital in West Bengal. A 40-year-old farmer presents with progressive skin darkening, hard nodules on his palms, and tingling in both feet. On direct questioning, he says his entire village drinks from tube wells and 'the water is a bit yellowish.' You suspect arsenicosis. Walk through: which investigations would confirm the diagnosis; how would you document the exposure history to support both clinical management and any future environmental legal action; to which authority would you report this as a potential cluster case; and under which statute could affected villagers seek compensation from the government or the tube-well operator? Finally, consider: why has India adopted a provisional tolerance of 50 µg/L for arsenic in drinking water when the WHO standard is 10 µg/L, and what are the public health ethics of that gap?