Page 1 of 16
FM13.{1-2,4} | Introduction to Toxicology: Definitions, History & Law — SDL Guide
Learning Objectives
- Define toxicology, forensic toxicology, clinical toxicology, and poison with medico-legal precision (FM13.2)
- Outline the history of toxicology from ancient poisoning through Orfila's foundational contributions to modern Indian forensic science (FM13.1)
- Describe the physician's documentation and reporting duties when a poisoning case is encountered (FM13.4)
- Explain the legal framework governing poisons in India — Poisons Act 1919, NDPS Act 1985, Drugs & Cosmetics Act 1940, and relevant IPC sections (FM13.4)
INSTRUCTIONS
Poisoning cases place unique obligations on every physician — clinical, legal, and ethical simultaneously. In India, where organophosphate, medication, and snake-bite poisonings account for thousands of deaths annually (NCRB data), the treating doctor is often the first medico-legal officer on the scene. This module builds the definitional and legal foundation you need before approaching any specific poison. Understanding what a poison legally is, who Orfila was and why his work matters, and precisely which Acts and IPC sections govern your duties will directly determine whether your records help or hurt in a criminal investigation.
References
- KSN Reddy — Essentials of Forensic Medicine & Toxicology, 34th ed. (textbook)
- BV Subrahmanyam — Modi's Medical Jurisprudence and Toxicology, 24th ed. (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 28-year-old agricultural worker is brought unconscious to the emergency department. His family reports he 'drank something from the field.' His clothes smell of a pungent chemical, his pupils are pin-point, he is salivating profusely, and his pulse is 52/min. Within minutes of arrival, the treating intern is confronted with three simultaneous demands: stabilise the patient, take a proper history for the medico-legal record, and decide whether to call the police. The intern has no idea which Act requires police notification, whether the sample she just collected must go in formalin, or what the difference between 'forensic toxicology' and 'clinical toxicology' even is. The consequences of getting any one of these wrong could be clinical harm, a compromised investigation, or personal professional liability.
WHY THIS MATTERS
Every physician who works in an emergency department, a rural primary health centre, or a medico-legal unit will encounter poisoning cases. India has one of the highest poisoning-related mortality burdens in the world. Beyond clinical management, poisoning cases carry mandatory legal obligations: failure to notify the police, improper viscera preservation, or inaccurate record-keeping can make or break a criminal prosecution and expose the physician to liability under the Consumer Protection Act 2019 and the NMC Act 2020. The definitions you learn today are not academic niceties — they are the precise legal vocabulary used in court testimony, FSL reports, and inquest proceedings.
RECALL
From your Year-1 Pharmacology: you already understand the basic concept of a drug as a substance that alters body function. You recall that dose determines effect — even water is toxic in excess. From Physiology, you understand receptor-mediated signalling. From Biochemistry, you know the basics of hepatic metabolism (CYP450 enzymes) and renal excretion. Today we build on these foundations to define what distinguishes a 'poison' from a 'drug' in both scientific and legal terms, and to place toxicology in its historical and legal context.
Core Definitions in Toxicology
The language of toxicology carries precise meanings that differ from everyday usage, and in a medico-legal context these distinctions matter enormously. Toxicology is the scientific study of the adverse effects of chemical substances on living organisms — encompassing detection, mechanisms of harm, treatment, and prevention. The term is derived from the Greek toxikon (arrow poison) and logos (study), reflecting its ancient origins in weaponised plant extracts. Within toxicology, two major applied branches serve distinct professional functions.
Forensic toxicology is the application of toxicological principles and analytical methods to medico-legal investigations — answering legal questions such as 'did this substance cause this death?' and 'was this person impaired at the time of the incident?' It serves the criminal justice system, working at the intersection of chemistry, pathology, and law. Clinical toxicology, by contrast, is concerned with the diagnosis, management, and prevention of poisoning in living patients — the emergency physician's domain. The two disciplines often overlap: a patient who survives a poisoning attempt becomes a forensic case when the circumstances are suspicious.
The term poison has both a scientific and a legal meaning. Scientifically, a poison is any substance that, when introduced into or applied to a living organism in a sufficient quantity, by any route of administration, is capable of causing harm, disease, or death by its own chemical or physiological action. This definition deliberately omits intent — the same substance is a poison whether taken accidentally, suicidally, or homicidally. Legally in India, 'poison' is contextualised by the Poisons Act 1919 and the NDPS Act 1985 (discussed below). A distinction must be drawn between a toxin (a poison of biological origin — produced by a living organism, such as botulinum toxin or snake venom) and a venom (a toxin that is actively injected, usually by a specialised anatomical apparatus such as a fang or sting). All venoms are toxins, but not all toxins are venoms.
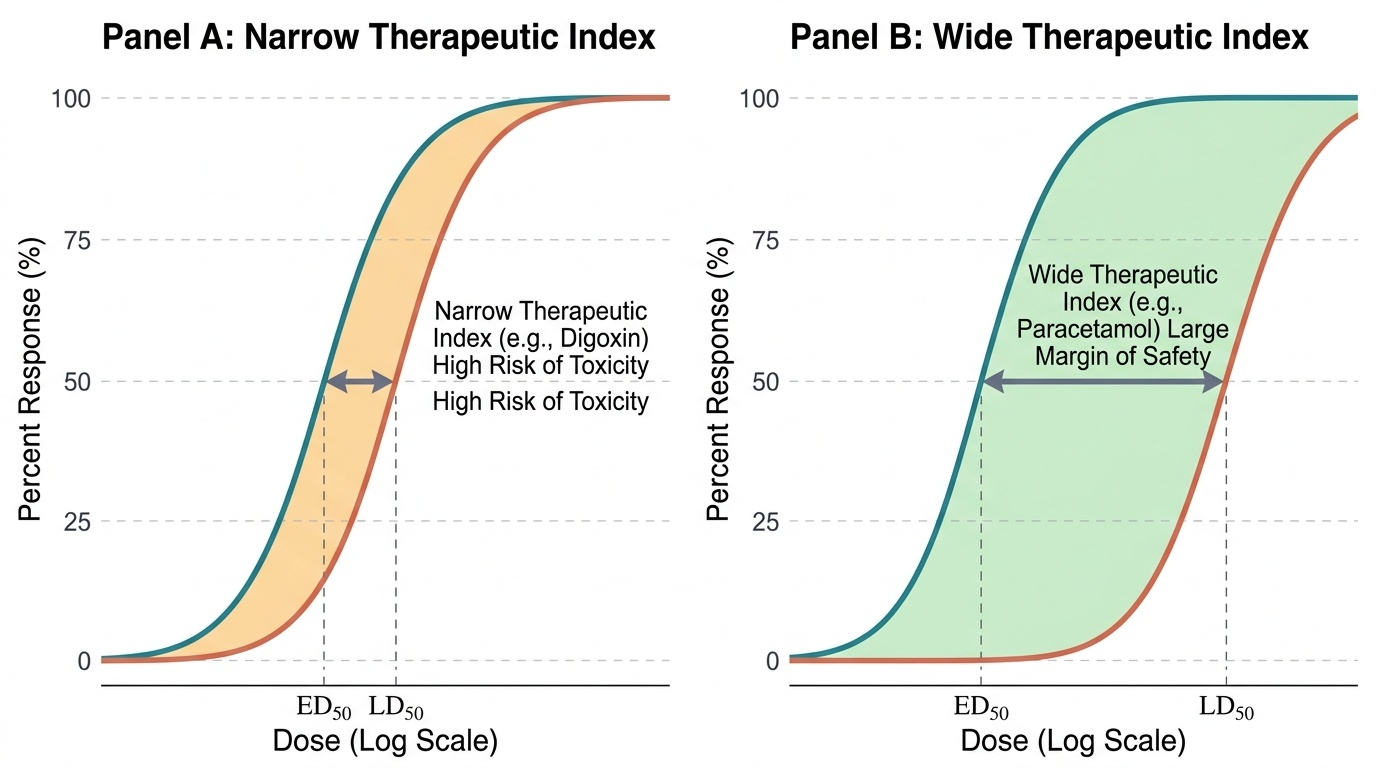
Two pharmacological concepts underpin toxicological risk assessment. LD50 (Lethal Dose 50) is the dose of a substance that kills 50% of a defined test population under specified experimental conditions. It is expressed in mg/kg body weight and is always qualified by species, route of administration, age, and sex — a bare LD50 without these qualifiers is meaningless for risk assessment. The therapeutic index (TI) is the ratio LD50/ED50 (where ED50 is the effective dose for 50% of the population), and it quantifies the margin of safety between a therapeutic and a lethal dose. A narrow therapeutic index — as seen with digoxin, lithium, warfarin, phenytoin, and aminoglycosides — means that the toxic dose is only marginally above the therapeutic dose, and small deviations in dosing or patient factors (renal function, drug interactions) can precipitate toxicity.
Provided image
- Toxicology = science of adverse chemical effects on organisms
- Forensic toxicology = toxicology in service of legal investigation
- Clinical toxicology = diagnosis and management of poisoning in the living
- Poison = any substance causing harm by chemical/physiological action in sufficient quantity
- Toxin = biologically produced poison (bacterial, plant, or animal)
- Venom = toxin actively injected via a specialised apparatus
- LD50 = dose killing 50% of test population (species/route/sex/age specific)
- Therapeutic index = LD50/ED50 — narrow TI drugs require tighter monitoring
SELF-CHECK
A pharmaceutical company reports that Drug X has an LD50 of 5 mg/kg in male Wistar rats via intraperitoneal injection and an ED50 of 0.5 mg/kg. Which statement correctly describes this drug's therapeutic index?
A. Therapeutic index = 10; the drug has a wide margin of safety
B. Therapeutic index = 10; but this cannot be extrapolated directly to humans without qualification
C. Therapeutic index = 0.1; the drug has a narrow margin of safety
D. Therapeutic index = 2.5; typical of narrow-TI drugs requiring monitoring
Reveal Answer
Answer: B. Therapeutic index = 10; but this cannot be extrapolated directly to humans without qualification
TI = LD50/ED50 = 5/0.5 = 10. Option A is mathematically correct but incomplete — the TI value is correct, but it was derived in rats via IP injection and cannot be directly extrapolated to human oral dosing without qualification. Option B correctly states both the value and the critical limitation. A TI of 10 is actually relatively wide, not narrow (narrow TI drugs like digoxin have TIs approaching 2-3 in clinical practice).
History of Toxicology: From Ancient Poisons to Forensic Science
The history of toxicology is, in many respects, a history of human ingenuity in both applying and defending against chemical harm. Understanding this history matters not as trivia but because it contextualises the legal frameworks and analytical methods still in use today — Indian forensic science laboratories follow procedures whose intellectual lineage runs directly back to 19th-century European analytical chemistry.
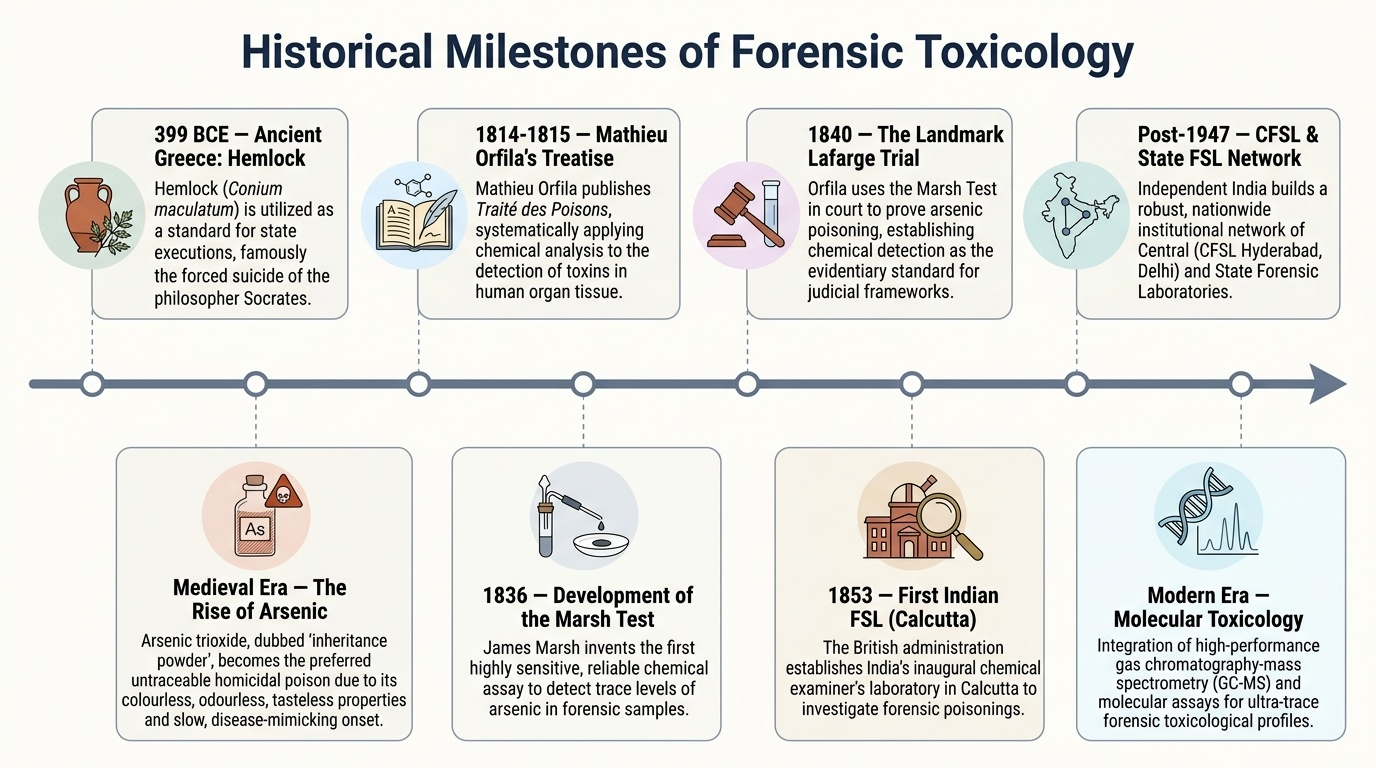
The ancient world had extensive knowledge of poisons. In Greece, hemlock (Conium maculatum) was used for state execution — most famously in the death of Socrates in 399 BCE. The Roman and medieval periods saw widespread use of arsenic (as arsenic trioxide, 'inheritance powder') for homicidal poisoning, owing to its colourless, odourless, tasteless properties and slow onset mimicking natural illness. The challenge for investigators was that there was no reliable way to prove arsenic had been administered — until the 19th century.
The founding of modern forensic toxicology is attributed to Mathieu Joseph Bonaventure Orfila (1787–1853), a Spanish-born chemist working in Paris who published Traité des Poisons (Treatise on Poisons) in 1814–1815. Orfila was the first to systematically apply chemical analysis to forensic investigation of poisoning deaths, demonstrating that poisons could be detected in body tissues and organs even after burial. His landmark contribution was the application of the Marsh test (developed by James Marsh in 1836) in the famous Lafarge poisoning trial of 1840, which established analytical chemistry as the foundation of forensic toxicology. Before Orfila, courts relied on symptoms and circumstantial evidence; after him, chemical detection became the evidentiary standard.
In India, the development of forensic science infrastructure paralleled the British colonial administration's need to investigate suspicious deaths. The first Forensic Science Laboratory (FSL) in India was established in Calcutta in 1853, primarily for chemical analysis of suspected poison cases. The Chemical Examiner to Government — a position that persisted long after independence — was the predecessor of the modern FSL. Post-independence, India developed a network of Central and State FSLs, with the Central Forensic Science Laboratory (CFSL) in Hyderabad (and later Delhi and Chandigarh) serving as the apex laboratory. The Directorate of Forensic Science Services under the Ministry of Home Affairs oversees this network today.
Modern toxicology has expanded far beyond Orfila's arsenic tests. Instrumental analytical methods — chromatography, mass spectrometry, and atomic absorption spectroscopy — now allow detection of poisons at nanogram and picogram concentrations. The discipline encompasses occupational toxicology, environmental toxicology, clinical pharmacology, and regulatory science. Nevertheless, the core medico-legal function that Orfila pioneered — using chemical evidence to answer legal questions about cause of death — remains the defining mission of forensic toxicology.
Provided image
Key historical milestones:
• 399 BCE — Socrates executed by hemlock; first documented medico-legal use of plant poison
• ~1500-1800 CE — Arsenic era: 'inheritance powder' widely used for homicidal poisoning; no analytical detection available
• 1814-15 — Orfila publishes Traité des Poisons; founds modern forensic toxicology
• 1836 — James Marsh develops the Marsh test for arsenic
• 1840 — Orfila applies Marsh test in Lafarge trial — first forensic chemical evidence admitted in court
• 1853 — India's first FSL established in Calcutta
• 20th century — Chromatographic and spectroscopic methods transform analytical sensitivity and specificity
• Post-2000 — LC-MS/MS becomes the gold standard for forensic drug analysis
Physician's Duties in a Poisoning Case: Documentation and Reporting
When a poisoning case presents to any clinical setting, the treating physician simultaneously takes on the role of a medico-legal first responder. The quality of the physician's documentation and the timeliness of their reporting can determine whether a criminal investigation succeeds or fails. This role is not optional — it is a statutory duty under Indian law, and failure carries professional and legal consequences.
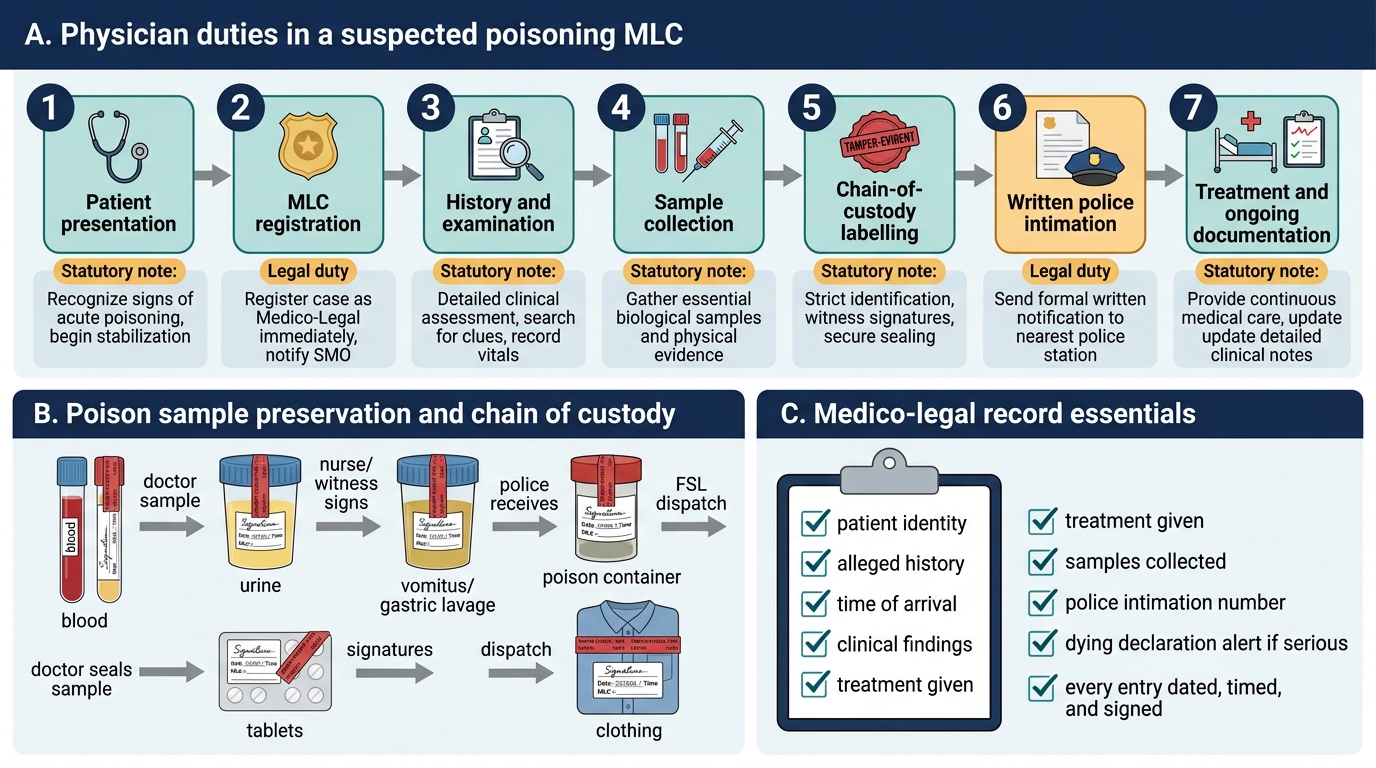
The clinical record in a suspected poisoning case must be written with particular care because it will almost certainly be subpoenaed. History-taking must document: the exact time of alleged exposure, the route of exposure, the identity and quantity of the alleged substance (if known), where the substance was found (scene details), who was present, any first aid given before hospital arrival, and any witnesses. If the patient is conscious and competent, their own account must be recorded verbatim. If they are unconscious, the history must come from relatives or bystanders, and the source of each piece of information must be clearly documented.
Physical examination findings should be recorded systematically and with sufficient specificity to support later medico-legal interpretation — not merely clinical management. This includes: exact pupil size and reactivity (e.g., 'pupils 2 mm bilaterally, non-reactive to light' rather than 'pinpoint pupils'), precise descriptions of any skin findings (colour, distribution, pattern of burns or blisters), odour noted (garlic odour of OP/arsenic, bitter almond odour of cyanide, alcohol), nature of vomitus if observed, and any items brought in by the family (containers, blister packs, leaves).
Mandatory police intimation is required whenever a physician suspects or has reasonable grounds to believe that a case involves suicidal, homicidal, or accidental poisoning — essentially in all but clearly accidental domestic exposures without suspicious circumstances. This obligation derives from the Code of Criminal Procedure (CrPC) provisions under which a medical officer receiving an MLC (medico-legal case) must inform the nearest police station without delay. Failure to notify is a serious professional lapse and may constitute obstruction of justice. The written intimation should include: case name and age, date and time of presentation, alleged substance, present condition of the patient, and hospital/MLC registration number.
Chain of custody for samples is critical. Any body fluid or material collected as evidence must be: labelled with patient name, registration number, date and time of collection, and the collector's signature; sealed in the presence of a witness (ideally a police officer); and documented in the MLC register with matching entries. Breaking the chain of custody renders the sample inadmissible as evidence.
Physician Duties in a Poisoning MLC
Key documentation duties:
• Record verbatim history (patient or witness account) with source identified
• Detailed physical findings — precise measurements, not clinical shorthand
• MLC registration number assigned to the case
• Written police intimation — prompt, complete, signed
• Sample labelling and sealing with chain-of-custody documentation in the MLC register
• No disclosure of case details to any party other than the investigating police officer without patient consent or court order (confidentiality obligations)
Legal Framework Governing Poisons in India
The legal regulation of poisons in India is distributed across several statutes, each addressing a different aspect of poison control and medico-legal accountability. A physician practising in India must be conversant with this framework not only to fulfil statutory duties but to correctly advise patients, handle poison prescriptions, and give accurate court testimony.
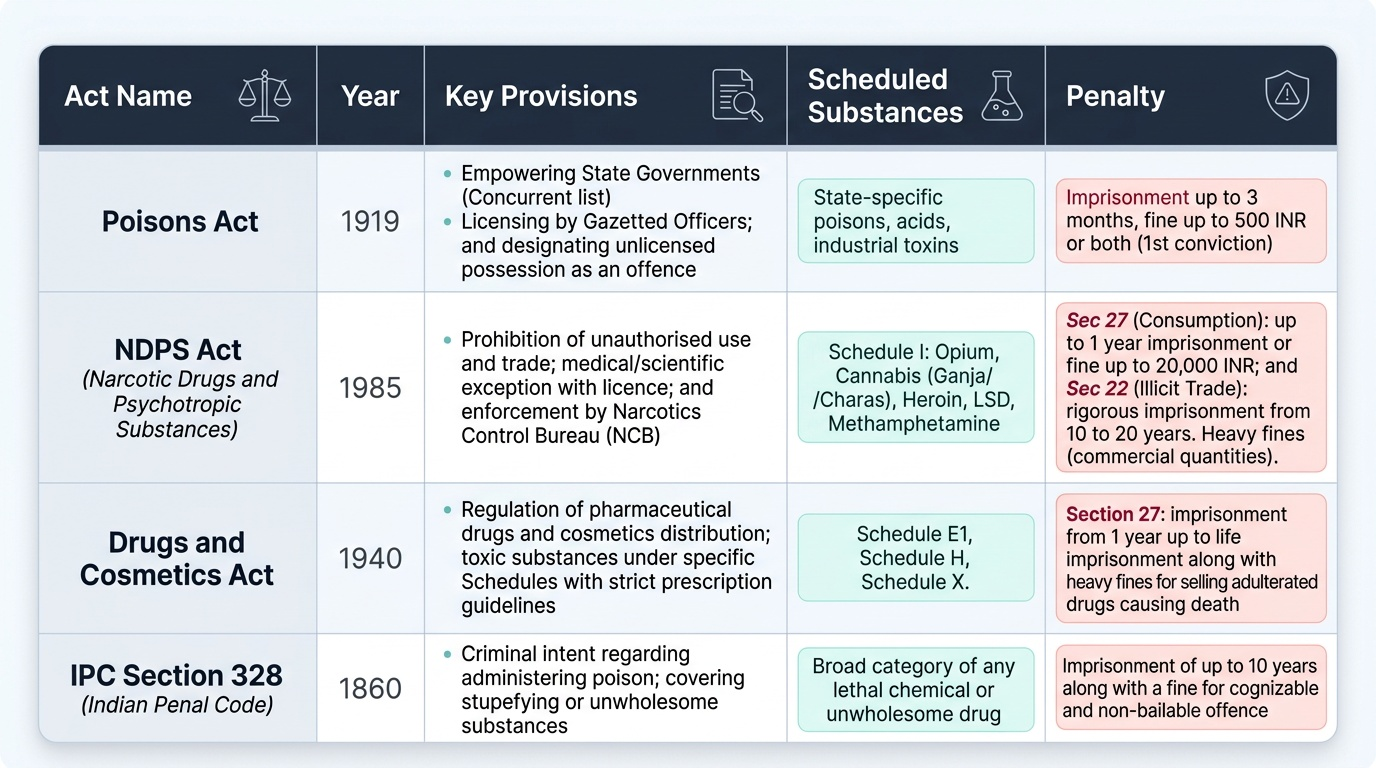
The Poisons Act 1919 is the oldest and most basic statute. It empowers state governments (under the concurrent list) to regulate the import, possession, manufacture, sale, and transport of scheduled poisons. Each state can define its own list of 'scheduled poisons' and prescribe conditions under which they may be obtained — typically requiring a licence from a gazetted officer. The Act is relevant medico-legally because unlicensed possession of a scheduled poison can itself constitute an offence, and evidence of purchase is admissible in poisoning investigations.
The Narcotic Drugs and Psychotropic Substances (NDPS) Act 1985 is the most important piece of legislation for the forensic toxicologist dealing with drug-related deaths and impairment. It prohibits manufacture, trade, consumption, use, possession, transportation, import, and export of narcotic drugs and psychotropic substances except for medical/scientific purposes with a licence. Schedule I of the NDPS Act lists prohibited narcotic drugs and psychotropic substances for which no legitimate use is permitted. Section 22 deals with offences relating to psychotropic substances; Section 27 provides for punishment for personal consumption of narcotic drugs or psychotropic substances. The Act is enforced by the Narcotics Control Bureau (NCB) at the central level. Critically, the NDPS Act does not merely regulate — it criminalises. A physician who prescribes controlled substances outside the Act's framework may face prosecution.
The Drugs and Cosmetics Act 1940 (and its Rules) classifies pharmaceuticals into schedules. Schedule H drugs require a prescription and cannot be sold over the counter; Schedule X drugs (benzodiazepines, barbiturates, certain opioids) require a prescription from a registered medical practitioner and must be retained by the pharmacist. The Act is relevant when a prescription drug is suspected in an overdose — the prescriber's and pharmacist's records become part of the investigation.
Under the Indian Penal Code (IPC), several sections directly concern poisoning. IPC Section 328 makes it an offence (punishable up to 10 years imprisonment) to administer a stupefying, intoxicating, or unwholesome drug or substance to a person with intent to commit, or to facilitate the commission of, an offence. This is distinct from IPC Section 304A (causing death by negligence), which applies when a physician's error results in a fatal outcome. IPC Sections 272–274 address adulteration of food or drugs intended for sale — relevant in cases of food poisoning or counterfeit medicines.
Physician liability in poisoning cases is now governed primarily by the Consumer Protection Act 2019 (which replaced the 1986 Act), treating medical services as a 'service' for which the consumer may file a complaint. Professional standards are set by the NMC Act 2020 (which replaced the IMC Act 1956). Documentation failures, delay in police notification, and breach of chain of custody are all potential grounds for proceedings under these statutes.
Provided image
| IPC Section | Offence | Maximum Punishment |
|---|---|---|
| Sec 272 | Adulteration of food/drink to make it noxious | 6 months or fine |
| Sec 274 | Adulteration of drugs | 6 months or fine |
| Sec 328 | Causing hurt by administering poison/intoxicant with intent | 10 years + fine |
| Sec 304A | Causing death by negligence | 2 years or fine or both |
| Sec 299–304 | Culpable homicide / murder (when poison is used as weapon) | Life imprisonment / death |
SELF-CHECK
A patient presents with suspected intentional self-poisoning by an unknown substance. She is conscious and refuses to allow the doctor to call the police. Which statement best describes the physician's legal obligation?
A. The physician must respect patient autonomy and withhold police notification unless the patient consents
B. The physician has a discretionary right to call the police but is not legally obligated
C. The physician must notify the police regardless of patient refusal because it is a statutory medico-legal duty
D. Notification is only required for homicidal poisoning, not suicidal attempts
Reveal Answer
Answer: C. The physician must notify the police regardless of patient refusal because it is a statutory medico-legal duty
Mandatory police intimation in all suspected poisoning cases (suicidal, homicidal, or suspicious accidental) is a statutory duty under CrPC MLC provisions — it is non-discretionary and is not subject to patient veto. Patient autonomy governs treatment decisions but cannot override the physician's statutory duty to report to authorities in medico-legal cases. Failure to report is a professional lapse and may constitute obstruction of justice.
CLINICAL PEARL
The NDPS Section 27 trap for prescribers: Many physicians believe that Section 27 of the NDPS Act 1985 (punishment for personal consumption of narcotic/psychotropic substances) applies only to addicts caught in possession. In fact, the medicolegal relevance for prescribers is different: if a physician prescribes an NDPS-listed drug outside the permitted medical framework — without a valid Schedule X prescription retained in the pharmacist's records — they can be implicated when that prescription is traced in an overdose investigation. Always retain a copy of Schedule X prescriptions, write legibly, include the indication and duration, and never leave blank prescription pads with the patient. Additionally, formalin (formaldehyde) is absolutely contraindicated as a viscera preservative for FSL samples — a fact that trips many students. Formalin cross-links proteins and destroys volatile organic compounds, rendering GC-based analysis impossible. Solid viscera must be preserved in saturated NaCl or rectified spirit (not rectified spirit if ethanol itself is the suspected poison).
SELF-CHECK
Which of the following statements about the NDPS Act 1985 is CORRECT?
A. Schedule I of the NDPS Act lists drugs approved for medical use with a prescription
B. Section 22 deals with personal consumption of narcotic drugs
C. Section 27 provides punishment for consumption of narcotic drugs or psychotropic substances
D. The NDPS Act 1985 was replaced by the Drugs and Cosmetics Act 1940
Reveal Answer
Answer: C. Section 27 provides punishment for consumption of narcotic drugs or psychotropic substances
Section 27 of the NDPS Act 1985 provides for punishment for consumption (personal use) of narcotic drugs or psychotropic substances. Schedule I lists PROHIBITED substances (not approved for medical use). Section 22 deals with offences relating to psychotropic substances (production/manufacturing/transport/sale), not personal consumption. The NDPS Act 1985 remains in force; it was not replaced by the Drugs and Cosmetics Act 1940 (a separate, older statute).
KEY TAKEAWAYS
This module has built the definitional and legal foundation for your study of toxicology in forensic medicine. Toxicology is the science of adverse chemical effects; forensic toxicology serves legal investigation; clinical toxicology serves the living patient. A poison is any substance causing harm by chemical action in sufficient quantity, regardless of intent — distinguished from a toxin (biologically produced) and a venom (injected by a specialised apparatus). LD50 and therapeutic index quantify risk and safety margin respectively and are always context-qualified.
Mathieu Orfila (1787–1853) founded modern forensic toxicology by applying analytical chemistry to legal investigations; India's first FSL was established in Calcutta in 1853, parallel to this development. The legal framework governing poisons in India spans the Poisons Act 1919 (possession/sale), NDPS Act 1985 (narcotic/psychotropic substances — Schedule I prohibited; Section 22 psychotropic offences; Section 27 personal consumption), and Drugs & Cosmetics Act 1940 (Schedule H and X prescription drugs). IPC Section 328 (administering poison with intent, up to 10 years) and Sections 272–274 (adulteration) are the core criminal provisions. Physician duties in any poisoning case include: detailed documentation (verbatim history, precise physical signs), mandatory police intimation (statutory, non-discretionary), and maintenance of chain of custody for all samples. Professional accountability is governed by NMC Act 2020 and Consumer Protection Act 2019 (NOT their predecessor Acts).
REFLECT
Consider the case of the agricultural worker you met at the start of this module. Now that you know the legal framework: if the patient dies despite treatment and the family alleges the hospital delayed calling the police, what documentation in the MLC register would protect you? If a police officer pressures you to change your recorded findings, what is your legal position? And at a broader level: does India's current poison regulatory framework adequately prevent agricultural pesticide suicides, which account for a significant proportion of poisoning deaths in rural areas? What policy change would you recommend and on what evidence?