Page 3 of 16
FM13.3 | Poisons: Classification, Toxicokinetics & Diagnosis — SDL Guide (Part 2)
Diagnosis of Poisoning in the Living
The clinical diagnosis of acute poisoning requires a structured approach that integrates history, physical examination findings, and targeted investigations into a coherent clinical picture. Because the patient is frequently unable to give a reliable history (unconscious, confused, or deliberately concealing the substance taken), the physician must be a skilled clinical detective — reading the body's signs as a toxidrome.
The history must be obtained from every available source: the patient (if conscious), witnesses (family, bystanders, emergency responders), emergency medical records, and the scene itself. Scene information is often the most reliable — a container found near the patient, agricultural spray equipment, empty blister packs, or a suicide note. The physician must document: the alleged substance (with brand name if available), estimated dose, route of exposure, time of exposure, any emesis before arrival, and any first aid measures already given. The history must be recorded in the MLC register verbatim with source attribution.
On physical examination, the recognition of toxidromes is the key skill. A toxidrome is a cluster of signs produced by a specific pharmacological mechanism, allowing identification of the poison class even when the agent is unknown.
| Toxidrome | Pupils | Heart Rate | BP | Skin | Key Signs |
|---|---|---|---|---|---|
| Cholinergic (muscarinic — OP/carbamate) | Miosis | Bradycardia | Low | Wet, sweating | SLUDGE: Salivation, Lacrimation, Urination, Defaecation, GI cramps, Emesis |
| Anticholinergic (atropine, antihistamines, TCA) | Mydriasis | Tachycardia | High | Dry, flushed | 'Blind as a bat, mad as a hatter, hot as hades, dry as a bone' |
| Sympathomimetic (cocaine, amphetamines) | Mydriasis | Tachycardia | High | Diaphoretic | Agitation, hyperthermia, seizures |
| Opioid | Miosis | Bradycardia | Low | Pale, cool | Respiratory depression, coma — triad |
| Sedative-hypnotic (BZD, barbiturates) | Normal/miosis | Normal/low | Low | Normal | CNS and respiratory depression without miosis |
| Serotonin syndrome | Normal/mydriasis | Tachycardia | High | Diaphoretic | Hyperthermia, clonus, rigidity, agitation |
Additional examination clues include: perioral burns (corrosive ingestion), specific odours (garlic/onion = OP or arsenic; bitter almond = cyanide; alcohol = ethanol; fruity = methanol or acetone; petroleum = hydrocarbon), cherry-red skin (CO poisoning), jaundice (hepatotoxic poison — paracetamol, phosphorus), track marks (IV drug use), and bite marks (snake, spider).
Initial investigations in the emergency setting should include: blood glucose (hypoglycaemia from insulin/sulphonylurea; hyperglycaemia from sympathomimetics), serum electrolytes and anion gap (elevated anion gap metabolic acidosis = methanol, ethylene glycol, cyanide, salicylates — the MUDPILES mnemonic), arterial blood gas, ECG (QRS widening = tricyclic antidepressants; QTc prolongation = many agents), renal and liver function, complete blood count, and urinalysis. Specific drug levels (paracetamol, salicylate, lithium, digoxin, methanol, ethanol) should be sent when clinically indicated.
Diagnosis of Poisoning in the Dead
When a body is brought for medico-legal autopsy with suspected poisoning as the cause of death, the forensic physician must systematically examine the scene context, the external body, and the internal organs to establish or exclude a poisoning aetiology. The challenge is that many poisons leave no specific macroscopic findings, and the conclusion will ultimately rest on the FSL chemical analysis — making the correct collection and preservation of viscera critically important.
The scene and circumstantial information must be documented before focusing on the body: what was found near the deceased (containers, agricultural equipment, pharmacy bags, blister packs), the position of the body, any vomitus or unusual staining, odours at the scene, and witness statements recorded by the police. This contextual information significantly focuses the FSL analysis and the autopsy examination.
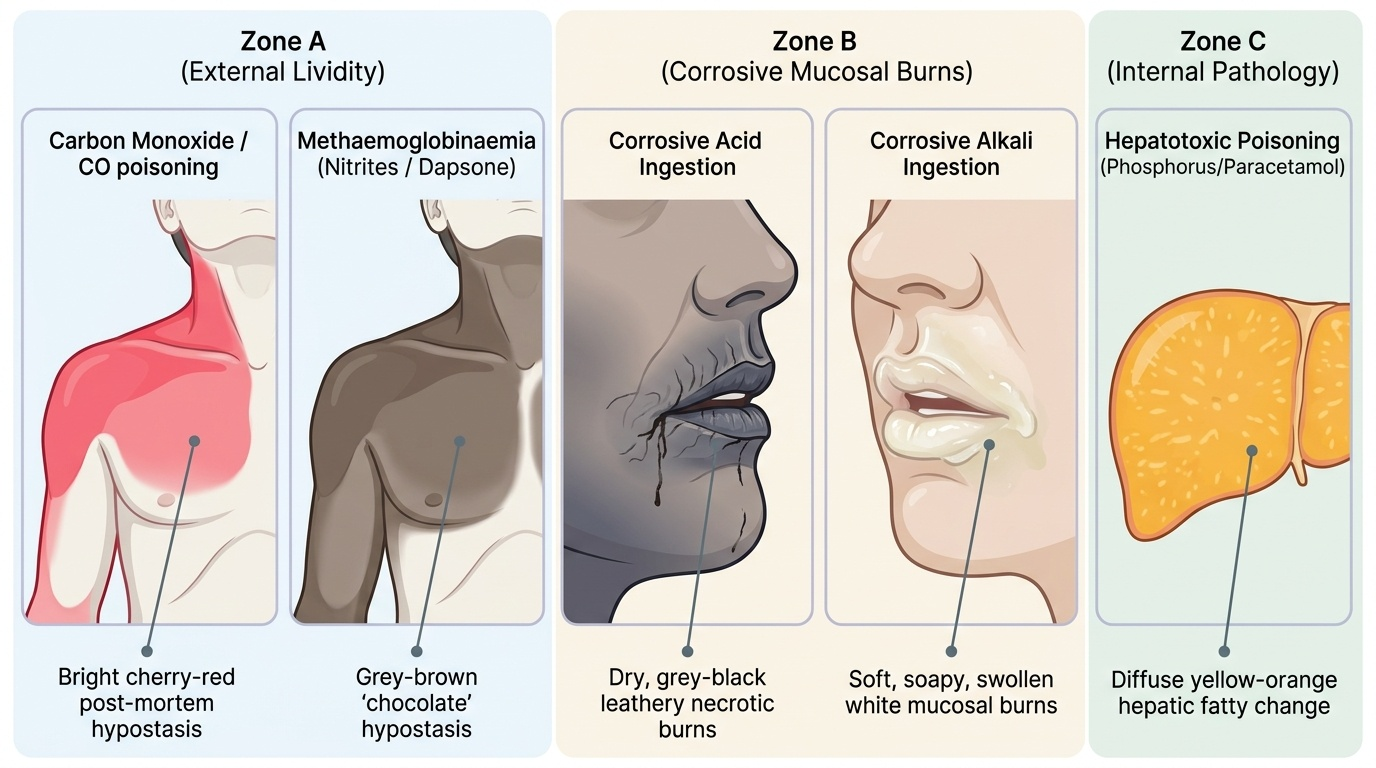
External examination may reveal specific poison-class clues: perioral and perinasal burns (corrosive ingestion — acid produces grey/black necrosis; alkali produces white saponification burns); skin colour (cherry-red lividity pathognomonic of CO poisoning; grey-brown cyanosis suggests methaemoglobinaemia from nitrites/dapsone); skin surface changes (scaling, hyperpigmentation, keratosis in chronic arsenic); needle marks (IV drug use); and specific odours on opening the body cavities (garlic from OP/arsenic, bitter almond from cyanide, alcohol).
Internal examination provides the most valuable post-mortem evidence. The gastric contents and their odour should be documented and a sample preserved before washing the stomach. GI mucosal findings: corrosive agents produce sloughing, necrosis, and perforation of the gastric mucosa — the distribution of mucosal damage (proximal = acid damage concentrated at pylorus; diffuse = alkali) can suggest the class of corrosive. Organ-specific changes: yellow discolouration of the liver (hepatocytic fatty change) is characteristic of phosphorus, paracetamol, and carbon tetrachloride hepatotoxicity; congested, heavy lungs suggest pulmonary irritant (paraquat); renal cortical pallor suggests nephrotoxic metals. Blood appearance: in CO poisoning the blood and all organs appear bright cherry-red due to carboxyhaemoglobin; in cyanide poisoning the venous blood may be bright red (histotoxic hypoxia — tissues cannot utilise O₂, so venous blood remains oxygenated).
Provided image
Key post-mortem poison-class indicators:
• Cherry-red lividity + bright red blood = carbon monoxide
• Perioral/pharyngeal burns = corrosive acid or alkali
• Yellow liver + GI haemorrhage = phosphorus, paracetamol, CCl₄
• Garlic/onion odour = organophosphate, arsenic
• Bitter almond odour = cyanide (HCN)
• Grey-brown discolouration = methaemoglobinaemia (nitrite, dapsone)
• Haemorrhagic gastric mucosa + intact mucosa overlying = irritant poisons (arsenic, antimony)
SELF-CHECK
A 35-year-old male presents with miosis, bradycardia (HR 48), excessive salivation, urinary incontinence, and muscle fasciculations. Which toxidrome does this represent, and what is the most likely poison class?
A. Anticholinergic toxidrome — antihistamine overdose
B. Sympathomimetic toxidrome — cocaine or amphetamine ingestion
C. Cholinergic (muscarinic) toxidrome — organophosphate or carbamate poisoning
D. Opioid toxidrome — heroin or morphine overdose
Reveal Answer
Answer: C. Cholinergic (muscarinic) toxidrome — organophosphate or carbamate poisoning
The combination of miosis, bradycardia, salivation, urinary incontinence (SLUDGE features), and fasciculations (nicotinic effect) is the cholinergic toxidrome produced by excess acetylcholine at muscarinic and nicotinic receptors. This is classic for organophosphate (OP) or carbamate poisoning — inhibition of acetylcholinesterase allows acetylcholine to accumulate. The anticholinergic toxidrome is the exact opposite (mydriasis, tachycardia, dry skin, flushing). The opioid triad is miosis + respiratory depression + coma, without the secretory/motor features of cholinergic excess.
Medicolegal Significance of Poison Classification
In a medico-legal report, the classification of the poison involved is not a background detail — it directly determines the legal framework applied and the inferences drawn about intent, manner of death, and culpability. Understanding the medicolegal significance of each classification category is therefore a core competency for a forensic physician.
The manner of death in poisoning cases is classified as: natural (rare — accidental exposure to environmental toxin in a person with no intent), accidental (unintentional ingestion — occupational exposure, accidental domestic ingestion by children, medication error), suicidal (intentional self-poisoning), homicidal (intentional poisoning of another), or undetermined (when the circumstances do not conclusively point to one category). The classification of the poison itself provides clues: a highly toxic substance available only to the deceased's family (e.g., a restricted Schedule I NDPS substance found in the victim's food) suggests homicide; an empty bottle of the deceased's own prescription medication beside the body suggests suicide. However, these inferences must be stated with appropriate evidentiary qualification in the FSL report — they cannot be definitively determined by the pathologist alone without the investigating officer's findings.
The IPC section applicable depends on classification and circumstances. A homicidal poisoning with a non-scheduled poison causing death is charged under IPC 302 (murder) or 304 (culpable homicide). Use of a poison to facilitate another offence (e.g., stupefying a victim before robbery or sexual assault) attracts IPC 328. For corrosive acids used as a weapon (acid attacks), specific provisions under IPC 326A (voluntarily causing grievous hurt by acid) now carry minimum 10-year imprisonment under the Criminal Law Amendment Act 2013. Accidental poisoning causing death of another may attract IPC 304A (negligence).
The FSL analytical protocol is determined by the suspected poison class: metal/mineral poisons → AAS; volatile organic poisons (alcohol, solvents) → GC; drugs of abuse and prescription drugs → TLC screening then HPLC/LC-MS confirmation; alkaloids (organophosphates, plant alkaloids) → TLC + GC; CO → spectrophotometric co-oximetry. The correct classification thus ensures that the appropriate analysis is requested, and that no critical evidence is missed by using an inappropriate analytical method.
Key medicolegal implications of classification:
• Corrosives = visible injuries; circumstantial evidence of intent (homicidal acid attack vs suicidal ingestion)
• NDPS substances (neurotic/sedative poisons) = triggers NDPS Act provisions; chain-of-custody samples essential
• Agricultural pesticides (OPs — irritant/neurotic class) = commonest suicidal poison in India; NCRB data used in epidemiological evidence
• Homicidal use of any poison class = IPC 302/304 depending on intent; poison class must be certified in the cause-of-death certificate by the forensic physician
CLINICAL PEARL
The 'garlic odour' trap in forensic practice: Garlic or onion odour at post-mortem is associated with both organophosphate poisoning (from the sulphur-containing OP compounds) and arsenic poisoning (from arsine gas release in decomposed cases). Do not assume the odour alone confirms one over the other — both must be considered. Similarly, 'bitter almond odour' suggesting cyanide is famously undetectable by approximately 40% of the population due to a genetic trait (inability to smell HCN). A negative odour finding does NOT exclude cyanide. For the FSL, direct spectrophotometric measurement of blood cyanide (or thiocyanate as metabolite) is the definitive test. On the classification front: a common examination error is to classify arsenic as a 'metallic irritant' and fail to note that it is simultaneously a remote (systemic) irritant AND a hepatotoxic AND nephrotoxic poison — its multi-organ involvement is what makes chronic arsenic poisoning the complex medicolegal entity it is in endemic areas like West Bengal and Assam.
SELF-CHECK
Phosphorus poisoning characteristically produces which post-mortem finding, and under which classification category (by action) does phosphorus fall?
A. Cherry-red lividity; asphyxiant poison
B. Yellow liver discolouration with fatty change; irritant (remote/hepatotoxic) poison
C. Perioral burns with grey mucosal necrosis; corrosive poison
D. Pulmonary oedema with haemorrhagic lungs; cardiac poison
Reveal Answer
Answer: B. Yellow liver discolouration with fatty change; irritant (remote/hepatotoxic) poison
Yellow phosphorus causes severe hepatotoxicity — the liver shows fatty change and yellow discolouration post-mortem (the 'phosphorus liver'). Phosphorus is classified as an irritant poison (remote systemic irritant) acting primarily on the liver and kidneys, not as a corrosive. Cherry-red lividity is CO (asphyxiant); perioral grey burns are corrosive acid; pulmonary oedema is seen with irritant gases (paraquat, phosgene) but is not the characteristic phosphorus finding.