Page 18 of 25
IM1.25 | Adult Congenital Heart Disease Presentations — SDL Guide
Learning Objectives
- Enumerate the major causes of adult presentations of congenital heart disease
- Describe and distinguish the distinguishing features between cyanotic and acyanotic congenital heart disease
- Identify the clinical signs, haemodynamic consequences, and complications of the common adult CHD lesions
- Discuss the Eisenmenger syndrome and its clinical implications
- Outline the principles of management of adult congenital heart disease including antibiotic prophylaxis and the role of interventional/surgical correction
INSTRUCTIONS
Congenital heart disease is no longer a purely paediatric specialty. Advances in paediatric cardiac surgery and catheter-based intervention over the past five decades mean that more than 95% of children with CHD now survive to adulthood — and in India, many patients with undiagnosed or surgically uncorrected CHD present for the first time in adult medicine clinics. This module covers the major adult CHD presentations and the fundamental distinction between cyanotic and acyanotic lesions.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 256 — Congenital Heart Disease in the Adult (textbook)
- API Textbook of Medicine, 10th ed., Ch. 10 — Congenital Heart Disease in Adults (textbook)
- ESC Guidelines for the Management of Adult Congenital Heart Disease, 2020 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 28-year-old woman is referred to the cardiology outpatient clinic with a 3-year history of worsening exertional dyspnoea and recent-onset exertional pre-syncope. She had an unremarkable childhood health history and was never investigated for a cardiac condition. On examination she is strikingly cyanosed — her lips, tongue, and fingertips are a dusky blue-grey. Her fingers show severe digital clubbing. Peripheral oxygen saturation is 82% on room air. Auscultation reveals a loud single S2, no murmur, and the JVP is elevated. A chest radiograph shows a large heart, reduced pulmonary vascular markings ('black lung fields'), and a right aortic arch. An echocardiogram reports: complete ventricular septal defect (VSD), an overriding aorta receiving blood from both ventricles, right ventricular hypertrophy, and severe pulmonary hypertension with bidirectional shunting — predominantly right-to-left. The echocardiographer labels this Eisenmenger syndrome complicating a VSD. She is told the window for corrective surgery has passed. This is the most important lesson in adult CHD: the window for correction closes when pulmonary vascular resistance irreversibly exceeds systemic — and once that threshold is crossed, surgery is contraindicated and the condition is managed palliatively. This module teaches you to recognise the signs, understand the haemodynamics, and know the management options before that window closes.
WHY THIS MATTERS
Adult congenital heart disease (ACHD) is encountered increasingly in internal medicine and general cardiology practice as the survivor population grows. In India, where echocardiographic screening in childhood is not universal and access to paediatric cardiac surgery is unevenly distributed, a significant proportion of CHD reaches adulthood undiagnosed or uncorrected. A final-year MBBS graduate must be able to identify the clinical features that suggest congenital heart disease in an adult, distinguish cyanotic from acyanotic lesions (as the haemodynamic mechanisms and prognosis differ fundamentally), recognise Eisenmenger syndrome, and understand the principles of management including the indications for antibiotic prophylaxis, the timing of intervention, and the specific risks of pregnancy in ACHD. The NMC IM1.25 competency requires you to enumerate the causes and describe the distinguishing features between cyanotic and acyanotic CHD at the KH level.
RECALL
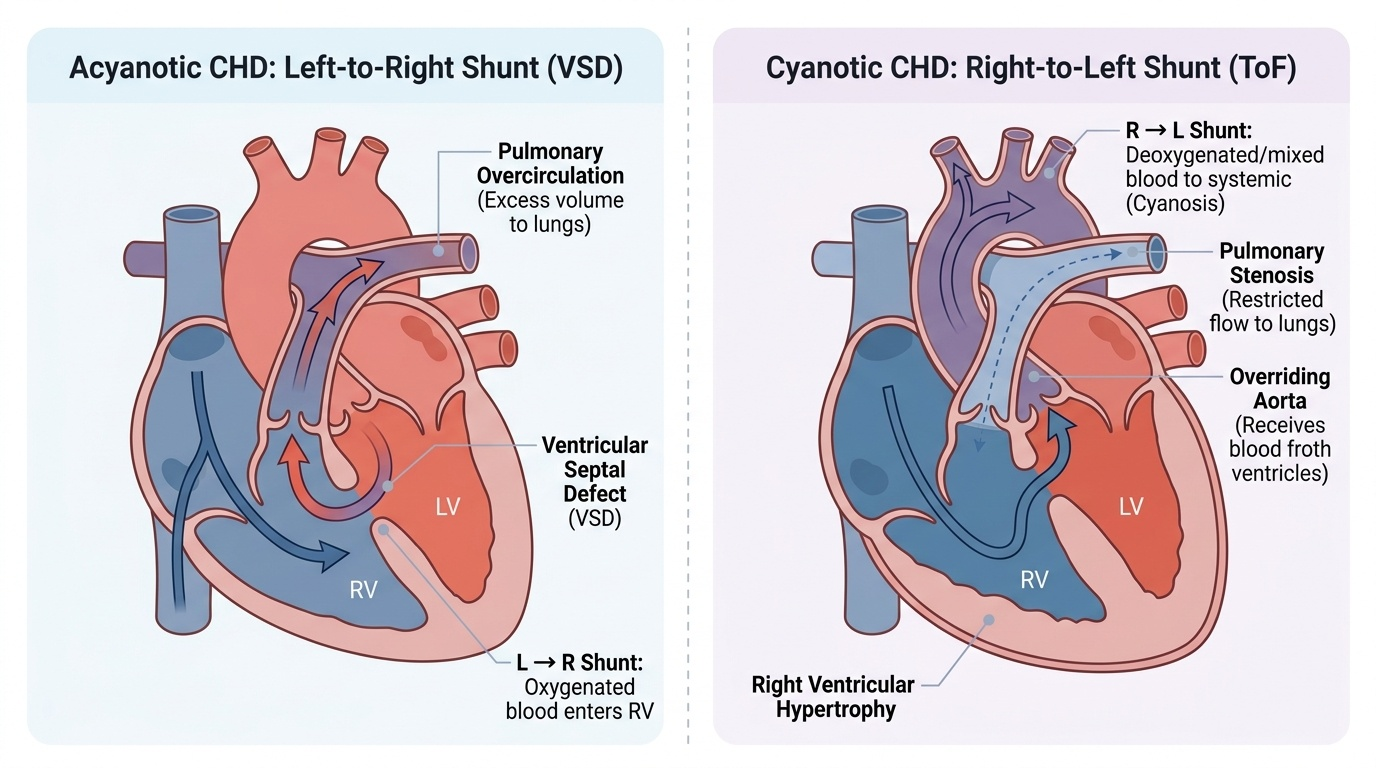
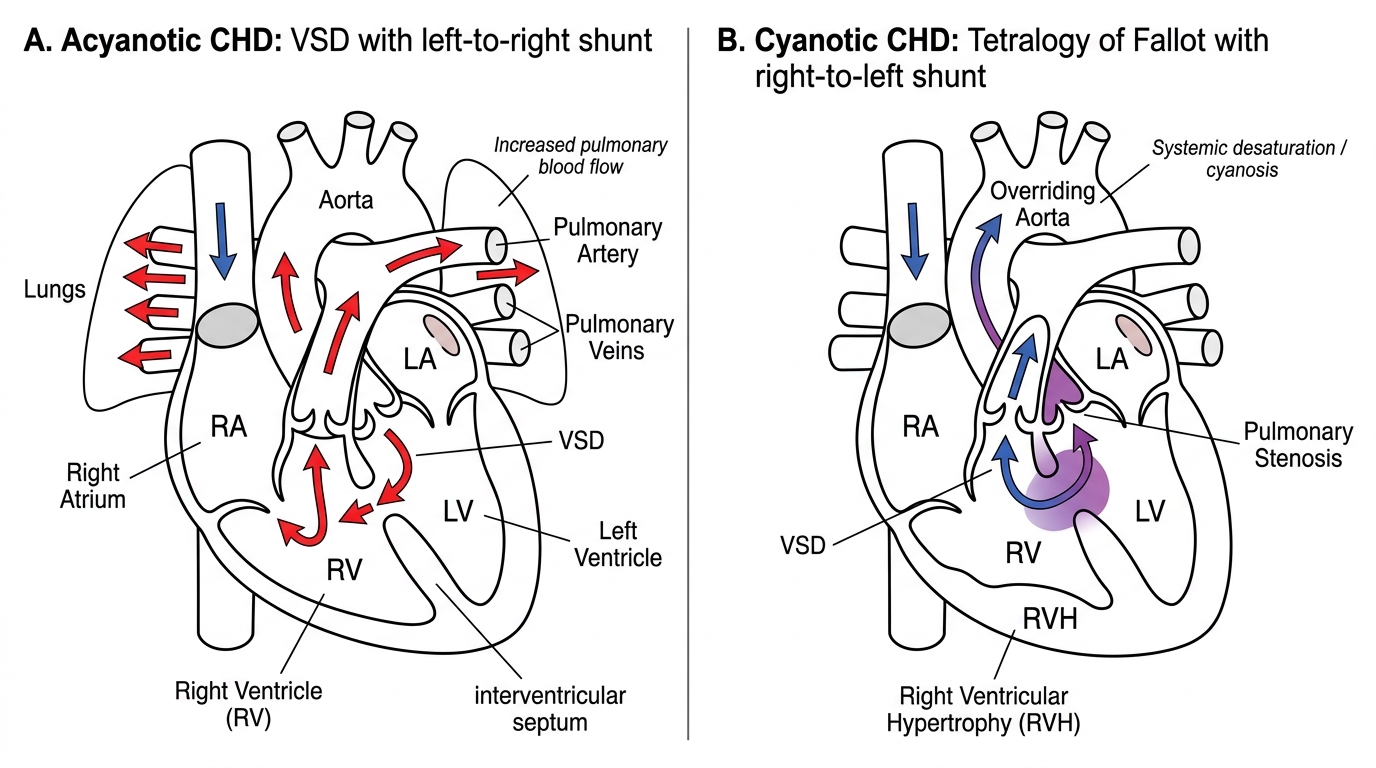
Recall the basic embryology: the normal heart develops from the cardiac tube by rightward looping, septation of the common atrium and ventricle, and spiral division of the truncus arteriosus. Errors in this process produce congenital defects. Recall the direction of blood flow: in the normal heart, the right heart (low pressure) receives deoxygenated blood from the systemic veins and sends it to the lungs; the left heart (high pressure) receives oxygenated blood from the pulmonary veins and sends it to the systemic circulation. A communication between left and right — whether at atrial, ventricular, or arterial level — produces a shunt. A left-to-right shunt (L→R) occurs when left-sided pressure exceeds right-sided pressure, pushing oxygenated blood back into the pulmonary circulation — this initially causes volume overload of the right heart and pulmonary circulation but does NOT cause cyanosis (oxygenated blood is added to the right side, not deoxygenated blood to the left). A right-to-left shunt (R→L) occurs when right-sided pressure exceeds left-sided pressure (or when the right and left outflows are mixed, as in Tetralogy of Fallot), pushing deoxygenated blood into the systemic circulation — this causes central cyanosis because deoxygenated blood bypasses the lungs.
Clinical Presentation: Acyanotic vs Cyanotic Congenital Heart Disease
The fundamental clinical and haemodynamic division in congenital heart disease is between acyanotic and cyanotic lesions. This distinction is determined by the direction of any intracardiac shunt and whether deoxygenated blood reaches the systemic circulation. Understanding this division provides the framework for classifying any CHD lesion and predicting its major complications.
Provided image
Acyanotic congenital heart disease comprises lesions that either (1) produce a left-to-right shunt (oxygenated blood crosses from left to right heart) or (2) obstruct outflow without a shunt. In left-to-right shunts, the systemic arterial blood remains fully oxygenated — there is no cyanosis. However, the pulmonary circulation receives excess volume from the recirculated left-sided blood, leading to pulmonary overcirculation, pulmonary hypertension over time, and right heart volume/pressure overload. The common acyanotic shunt lesions are:
- Ventricular septal defect (VSD): The most common CHD overall (accounting for ~35% of all CHD). A defect in the interventricular septum produces a L→R shunt at the ventricular level. The murmur is a harsh pansystolic murmur heard best at the left lower sternal border (4th intercostal space), transmitted throughout the praecordium. Small defects (maladie de Roger) are haemodynamically insignificant with a loud murmur. Large defects produce pulmonary overcirculation, heart failure in infancy, and risk of Eisenmenger syndrome in adulthood if uncorrected.
- Atrial septal defect (ASD): A defect in the interatrial septum — most commonly the ostium secundum type (central fossa ovalis, 70%). Less common: ostium primum (inferior septum, associated with AV canal defect), sinus venosus (near SVC or IVC), and coronary sinus type. The L→R shunt at atrial level causes right atrial and right ventricular volume overload. The murmur is an ejection systolic murmur at the left upper sternal border (increased flow across the pulmonary valve) with fixed splitting of S2 — the characteristic auscultatory finding. Fixed splitting means the normal inspiratory widening of S2 is absent; instead, P2 is delayed throughout the respiratory cycle because the RV stroke volume is always increased. Adults with large unrepaired ASD present with AF, right heart failure, and paradoxical embolism.
- Patent ductus arteriosus (PDA): Persistence of the foetal ductus arteriosus connecting the aorta to the pulmonary artery beyond 3 months of postnatal life. Produces a continuous 'machinery' murmur heard best at the left infraclavicular area — the murmur is continuous because the pressure gradient from aorta to pulmonary artery persists throughout both systole and diastole. Bounding pulses (wide pulse pressure) are characteristic. A large PDA causes pulmonary overcirculation and Eisenmenger if uncorrected.
Cyanotic congenital heart disease comprises lesions that produce a right-to-left shunt (deoxygenated blood crosses to the systemic circulation, bypassing the lungs) or where the pulmonary and systemic circulations are mixed. The clinical hallmarks are: central cyanosis (blue discolouration of the lips, tongue, and mucous membranes — unlike peripheral cyanosis which affects only the extremities), digital clubbing (from chronic hypoxia causing periosteal hypertrophy), and secondary polycythaemia (compensatory rise in haemoglobin and red cell mass in response to systemic hypoxia). The two most clinically important cyanotic CHD lesions in adults are:
- Tetralogy of Fallot (ToF): The most common cyanotic CHD, accounting for ~10% of all CHD. The classic tetrad consists of: (1) VSD, (2) overriding aorta (aortic root sits above the VSD, receiving blood from both ventricles), (3) right ventricular outflow tract obstruction (RVOTO — infundibular stenosis, pulmonary stenosis, or both), and (4) right ventricular hypertrophy (RVH, a consequence of the RVOTO and elevated RV pressure). The RVOTO means pulmonary blood flow is reduced; the RV pressure exceeds LV pressure, causing R→L shunting across the VSD. Deoxygenated blood preferentially exits via the overriding aorta → central cyanosis. Characteristic feature: 'boot-shaped heart' (coeur en sabot) on CXR — elevated apex (RVH) and concave pulmonary bay (small pulmonary trunk). Most ToF patients are now repaired in infancy; adults presenting with residual ToF are post-repair patients with residual pulmonary regurgitation, RV dilatation, or residual VSD.
- Transposition of the great arteries (TGA): The aorta arises from the right ventricle and the pulmonary artery from the left ventricle — creating two parallel circuits without mixing. Incompatible with life unless a mixing lesion (ASD, VSD, PDA) provides communication. In adults, this is seen in the context of surgically palliated or corrected TGA.
Acyanotic versus Cyanotic Congenital Heart Disease
Pathophysiology and Aetiology of Common Adult CHD
The pathophysiology of adult congenital heart disease is shaped by two processes: the primary haemodynamic consequence of the congenital defect, and the secondary consequences that develop over decades of abnormal loading conditions on the cardiac chambers and pulmonary vasculature. Understanding how a simple shunt evolves into Eisenmenger syndrome, or how a bicuspid aortic valve develops calcific stenosis in the 5th decade, transforms CHD from a static anatomical diagnosis into a dynamic longitudinal disease process that spans a lifetime and demands a different management framework at each stage of progression.
Aetiology of congenital heart disease:
The aetiology of CHD is multifactorial. In most cases (80–85%), no single cause is identifiable — sporadic genetic mutations or polygenic susceptibility combined with environmental factors during the first trimester of cardiac development. Identifiable causes include:
- Chromosomal abnormalities: Down syndrome (trisomy 21) — AV septal defect (AVSD/AV canal defect), VSD; Turner syndrome (45X0) — bicuspid aortic valve, coarctation of the aorta; DiGeorge syndrome (22q11.2 deletion) — truncus arteriosus, interrupted aortic arch, Tetralogy of Fallot; Noonan syndrome (RAS/MAPK pathway mutations) — pulmonary stenosis, HCM.
- Single-gene mutations: GATA4 and NKX2.5 mutations — ASD; TBX5 (Holt-Oram syndrome) — ASD + limb defects; MYH7, MYBPC3 — hypertrophic cardiomyopathy.
- Teratogenic exposures in the first trimester: Rubella (especially in India where vaccination coverage has historically been incomplete) — PDA, pulmonary artery stenosis, VSD, cataracts; thalidomide — multiple cardiac and limb defects; valproate — heart defects; alcohol — ASD, VSD; maternal diabetes — VSD, TGA, HOCM.
- Maternal systemic lupus erythematosus: Anti-Ro/SS-A antibodies cross the placenta and cause congenital complete heart block in the foetus — the mother's connective tissue disease is the cause, not a chromosomal anomaly.
Haemodynamic evolution of acyanotic L→R shunts:
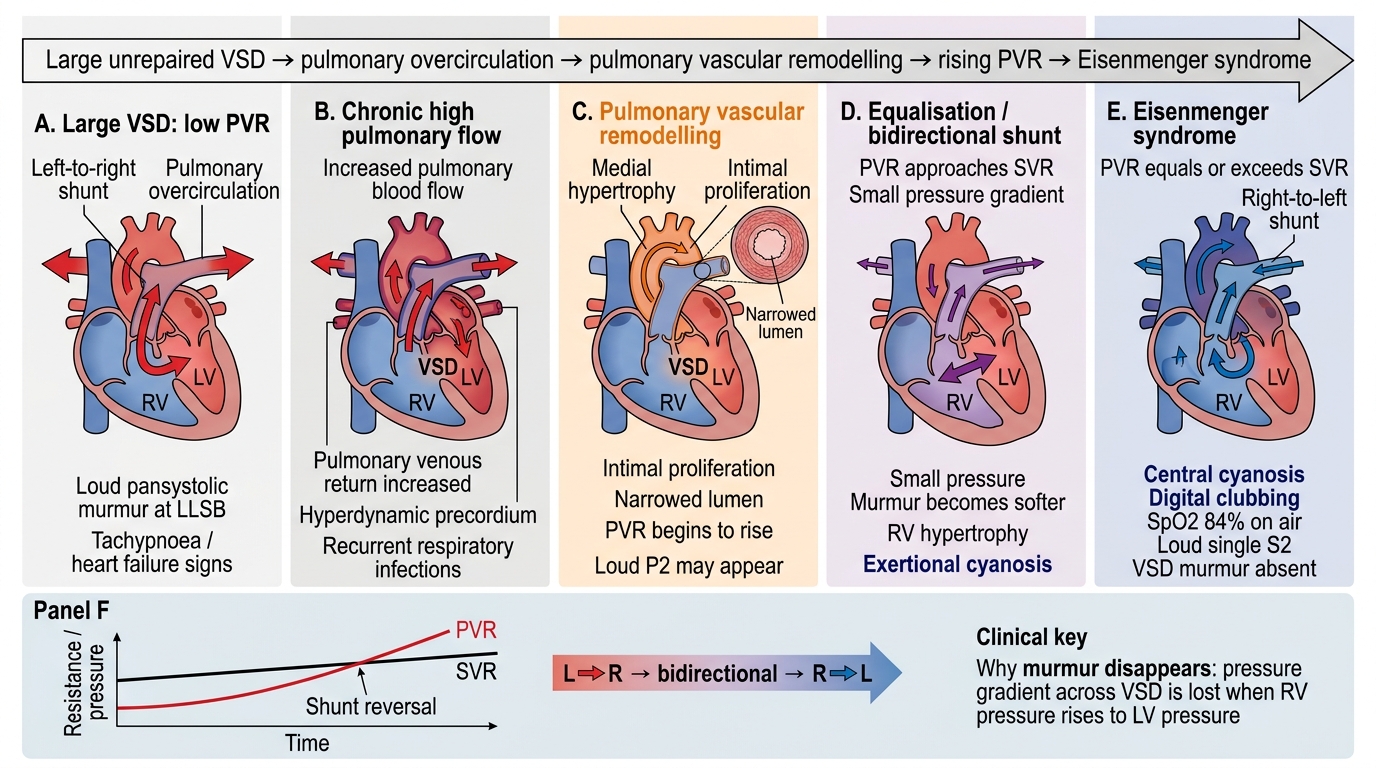
In an unrepaired left-to-right shunt (VSD, ASD, PDA), the pulmonary circulation receives excess blood volume. The initial pulmonary vascular response is vasodilatory accommodation; over years to decades, the sustained high-flow, high-pressure stimulus to the pulmonary arterioles triggers irreversible structural changes — medial hypertrophy, intimal fibrosis, and obliterative arteriopathy (Heath-Edwards classification stages I–VI). This progressively raises pulmonary vascular resistance (PVR). When PVR equals systemic vascular resistance (SVR), the net shunt across the defect becomes zero. When PVR exceeds SVR, the shunt reverses to right-to-left — deoxygenated blood now enters the systemic circulation. This is Eisenmenger syndrome — the endpoint of irreversible pulmonary arterial hypertension caused by a long-standing left-to-right shunt. Eisenmenger syndrome is characterised by: central cyanosis and clubbing (R→L shunt), secondary polycythaemia (Hgb often 18–22 g/dL), pulmonary arterial hypertension with a loud P2, elevated JVP with prominent 'a' wave, right heart failure, and haemoptysis (from pulmonary artery aneurysms or in situ thrombosis). The auscultatory finding changes dramatically: the original loud VSD murmur (from a large pressure gradient across the defect) disappears (pressures equalise) and is replaced by the signs of severe pulmonary hypertension (loud P2, right-sided S4, Graham Steell murmur of pulmonary regurgitation).
Bicuspid aortic valve (BAV):
The most common CHD in adults, affecting 1–2% of the general population. Most patients are diagnosed in adulthood when degenerative changes supervene. BAV has two cusps instead of three; the abnormal valve is prone to accelerated degenerative calcific change (producing aortic stenosis, typically presenting in the 5th–6th decade — 20 years earlier than tricuspid degenerative AS), regurgitation, and infective endocarditis. Crucially, BAV is associated with aortic root and ascending aorta dilatation (aortopathy) due to abnormal medial smooth muscle structure — independent of the haemodynamic severity of the valve lesion. This means even a haemodynamically minor BAV requires regular aortic imaging. Coarctation of the aorta occurs in ~20% of BAV patients.
Coarctation of the aorta:
A narrowing of the aorta, typically at the level of the aortic isthmus (just beyond the origin of the left subclavian artery). Classically presents in young adults (if not diagnosed in childhood) with: hypertension in the upper limbs with normal or low blood pressure in the lower limbs, radio-femoral delay (the femoral pulse arrives delayed compared to the radial pulse — because blood must traverse the collateral circulation to reach the lower body), and a continuous murmur over the back (from enlarged intercostal collateral arteries). Chest X-ray shows rib notching (3rd–8th ribs, from dilated intercostal collaterals) and the '3-sign' (indentation at the coarctation site producing a figure-3 contour of the aortic knuckle). Complications in adults: systemic hypertension, LVH, aortic dissection, infective endocarditis, and premature CAD from long-standing hypertension.
Evolution of Large VSD to Eisenmenger Syndrome
SELF-CHECK
A 35-year-old man with a known, previously unrepaired large VSD presents to the cardiology clinic. He was told as a child that he had a 'hole in the heart' but did not receive surgery. On examination: SpO₂ 84% on air, central cyanosis, digital clubbing, JVP elevated, loud single S2, no audible VSD murmur. What has happened to his VSD, and why has the murmur disappeared?
A. The VSD has spontaneously closed — the murmur is gone because the defect is sealed
B. Eisenmenger syndrome has developed — PVR now equals or exceeds SVR, reversing the shunt to right-to-left; the pressure gradient across the VSD is lost, abolishing the murmur
C. The murmur is now heard posteriorly — he needs a back auscultation
D. The cyanosis is from a new pulmonary embolism unrelated to the VSD
Reveal Answer
Answer: B. Eisenmenger syndrome has developed — PVR now equals or exceeds SVR, reversing the shunt to right-to-left; the pressure gradient across the VSD is lost, abolishing the murmur
Eisenmenger syndrome is the end-stage complication of a large unrepaired left-to-right shunt. The original loud VSD murmur (pansystolic, LLSB) was generated by the high-pressure gradient pushing blood from LV to RV. As pulmonary vascular resistance rises and equals systemic vascular resistance, the pressure gradient across the VSD disappears — there is no longer a directional shunt generating turbulence, so the murmur disappears. The shunt has now reversed to right-to-left (RV pressure > LV pressure), causing deoxygenated blood to enter the systemic circulation → central cyanosis, clubbing, polycythaemia. The VSD is structurally present but functionally reversed. This is not spontaneous closure.
Diagnosis, Investigations, and Key Clinical Signs
The clinical diagnosis of adult CHD requires careful integration of history (childhood symptoms, previous diagnoses, family history, maternal exposure history), physical examination (cyanosis, clubbing, murmur characteristics, splitting of S2), and targeted investigations. A structured approach prevents both over-investigation and missed diagnoses in what can be a subtle and varied presentation.
History: Key questions in adult CHD: Was there any cardiac diagnosis in childhood? Were any surgical or catheter procedures performed on the heart? Is there a family history of CHD or sudden cardiac death? Are there associated syndromic features (short stature, webbed neck for Turner; learning disability and typical facies for Down syndrome; limb defects for Holt-Oram)? In women: any history of cyanosis or murmur during prior pregnancies? Presenting symptoms in adult CHD vary by lesion: palpitations (AF is common in ASD, Ebstein anomaly), exertional dyspnoea and reduced exercise tolerance, syncope or pre-syncope (in severe RVOTO as in ToF or pulmonary stenosis), haemoptysis (Eisenmenger — from pulmonary artery in situ thrombosis or aneurysm rupture), paradoxical embolism and stroke (from ASD with PFO, where paradoxical thrombus crosses from right to left atrium).
Key examination findings:
| Lesion | Auscultation | Other signs |
|---|---|---|
| ASD | ESM LUSB + fixed split S2 | Right ventricular heave; AF in 40s–50s |
| VSD | Pansystolic murmur LLSB | Thrill at LLSB in moderate VSDs |
| PDA | Continuous machinery murmur left infraclavicular | Bounding pulses, wide pulse pressure |
| Pulmonary stenosis | ESM LUSB; loud ejection click | RV heave; post-stenotic pulmonary dilatation on CXR |
| Coarctation | Systolic murmur + continuous back murmur | Radiofemoral delay; BP arm > leg; rib notching on CXR |
| Eisenmenger (any shunt) | Loud single P2; no original shunt murmur | Central cyanosis; clubbing; polycythaemia; elevated JVP |
| ToF (repaired) | Pulmonary regurgitation murmur (early diastolic, soft) | RV enlargement; RBBB on ECG |
Investigations in adult CHD:
- 12-lead ECG: Right axis deviation (RAD) and right bundle branch block (RBBB) pattern suggest right ventricular volume or pressure overload — seen in ASD (volume overload → RBBB + RAD); right ventricular hypertrophy (RVH) in pulmonary stenosis, ToF, Eisenmenger (RAD, dominant R in V1, T-wave inversion V1–V4). Left axis deviation (LAD) and left-superior axis in ASD ostium primum (associated with AV canal defect that disrupts the inferior conduction system).
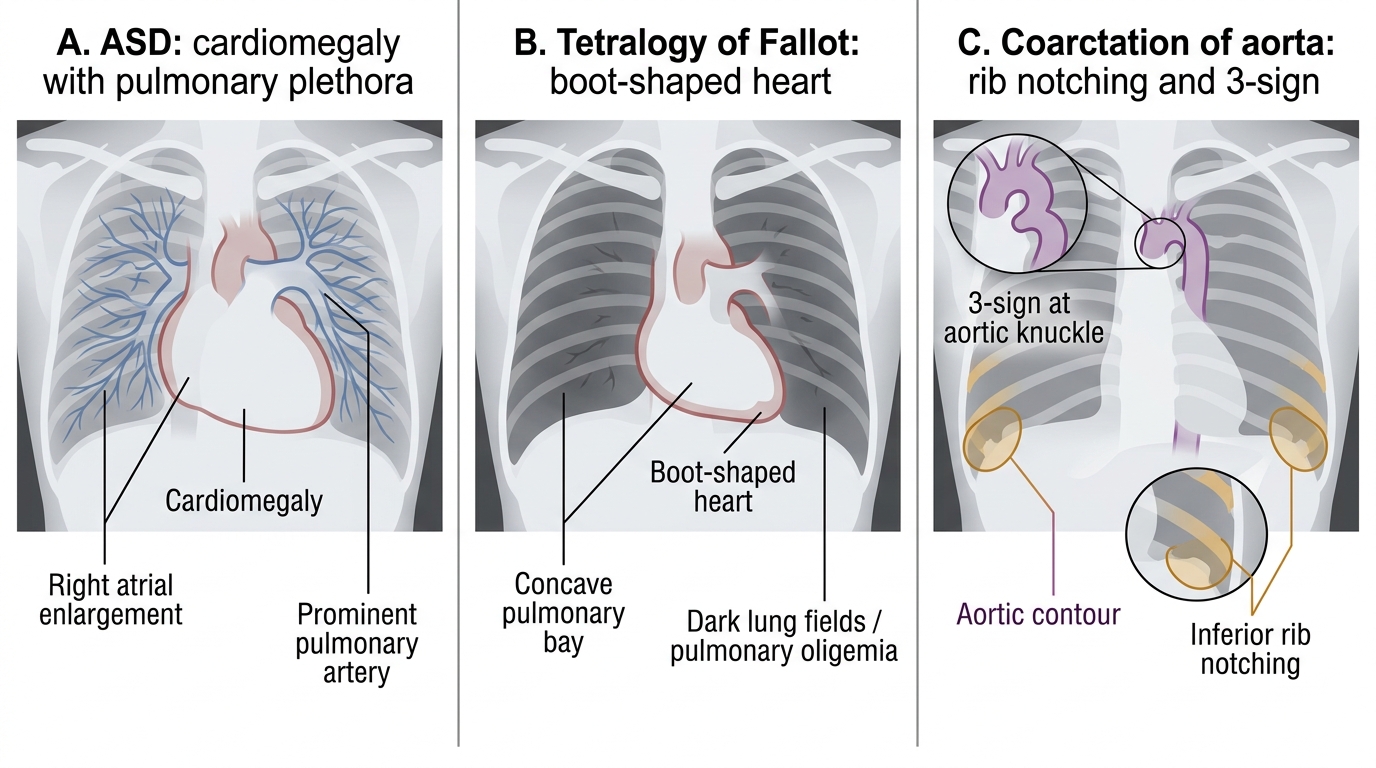
- Chest radiograph: Cardiomegaly pattern by chamber involvement; pulmonary vascularity — plethoric ('black lung fields' in severe pulmonary HTN from Eisenmenger; 'shunt vascularity' in uncomplicated L→R shunts); boot-shaped heart in ToF; rib notching in coarctation; right aortic arch in ToF.
- Echocardiography: The cornerstone of CHD diagnosis and follow-up. TTE demonstrates intracardiac anatomy, shunt direction and velocity (Doppler), and estimates pulmonary artery pressure (PA systolic pressure from the tricuspid regurgitation jet peak velocity using the modified Bernoulli equation). TOE provides superior visualisation of ASD morphology, pulmonary veins, and intracardiac devices. Contrast echo (agitated saline 'bubble study') demonstrates R→L shunting — bubbles appear in the left heart within 3 beats of injection, confirming patent foramen ovale (PFO) or ASD with R→L component.
- Cardiac MRI: The gold standard for RV volume quantification, aortic morphology (in BAV, coarctation), and evaluation of complex congenital anatomy. Essential in ACHD follow-up for monitoring RV dilatation post-ToF repair.
- Cardiac catheterisation: Measures pulmonary artery pressure and PVR directly — essential in Eisenmenger for reversibility testing (vasodilator challenge to assess whether PVR can be reduced, which would indicate operability). Also used for pre-procedural haemodynamic assessment before ASD/VSD closure.
Chest X-Ray Signs in Congenital Heart Disease
SELF-CHECK
A 32-year-old woman presents with progressive exertional dyspnoea and palpitations over 3 years. On auscultation: a soft ejection systolic murmur at the left upper sternal border and a widely fixed split S2. ECG shows right bundle branch block and right axis deviation. Echocardiogram confirms a 2.5 cm ostium secundum ASD with left-to-right shunting. Which finding is MOST specific for ASD compared to other cardiac causes of similar symptoms?
A. Right bundle branch block on ECG
B. Fixed splitting of S2
C. Ejection systolic murmur at the left upper sternal border
D. Right axis deviation on ECG
Reveal Answer
Answer: B. Fixed splitting of S2
Fixed splitting of S2 — where the A2-P2 split does not change with respiration — is the most characteristic and specific auscultatory sign of ASD. It occurs because the ASD ensures that right ventricular filling (and therefore stroke volume) is augmented throughout the respiratory cycle, so the normal inspiratory widening of S2 (which depends on differential increases in RV vs LV filling during inspiration) is abolished. The P2 is always delayed. RBBB and RAD occur in many right heart volume/pressure overload states and are not specific for ASD. The ejection systolic murmur is from increased pulmonary flow and is also non-specific.