Page 5 of 25
IM1.{8-14,26} | Heart Failure Clinical Evaluation — SDL Guide
Learning Objectives
- Recognise the clinical indications for a structured cardiovascular evaluation in suspected heart failure
- Explain the physiological basis of key clinical signs including raised JVP, S3, displaced apex, pulsus alternans, and pulsus paradoxus
- Demonstrate a systematic step-by-step CVS examination including history, pulse, accurate BP measurement, JVP measurement, precordial palpation, and auscultation
- Interpret clinical findings and map them to haemodynamic derangements and underlying aetiologies
- Generate and prioritise a differential diagnosis from an integrated history and examination in a patient with suspected heart failure
INSTRUCTIONS
This skills-arc SDL teaches you to perform, interpret, and present a complete cardiovascular examination in a patient with suspected heart failure. The spine is the clinical method itself — not the disease. Work through the six steps (indication → governing principles → technique → interpretation → applied practice → self-assessment) in order. Pay particular attention to the JVP measurement technique and the interpretation of heart sounds — both are high-yield examination stations in your final MBBS clinical. All content is aligned to NMC CBME 2024 competencies IM1.8–IM1.14 and IM1.26.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 252 — Heart Failure: Pathophysiology and Diagnosis (textbook)
- API Textbook of Medicine, 10th ed. — Section on Cardiovascular System: Heart Failure (textbook)
- Davidson's Principles and Practice of Medicine, 23rd ed., Ch. 17 — Cardiovascular Disease (textbook)
- Macleod's Clinical Examination, 14th ed. — The Cardiovascular System (textbook)
Version 1.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 58-year-old man walks into your ward clutching the bed rail, unable to complete a sentence without pausing for breath. His ankles are massively swollen. His wife says he has been sleeping upright on three pillows for the past month and woke last night gasping. As a final-year student on the ward round you are asked to examine him and present your findings. Where do you start? What are you looking for? How do you put the pieces together into a diagnosis? This module is your answer. Heart failure is not diagnosed by a machine — it is diagnosed at the bedside, by a clinician who knows what to look for, what each sign means physiologically, and how to synthesise a history and examination into a working differential. The signs — a raised jugular venous pressure, a displaced apex beat, a third heart sound, basal crepitations, bilateral pitting oedema — are not a checklist to be memorised but a physiological story to be read. You are about to learn to read that story with precision.
WHY THIS MATTERS
Heart failure is one of the most common cardiac diagnoses you will encounter in any general medical ward in India. The NMC competencies IM1.8 through IM1.14 and IM1.26 are set at SH (Skill, requiring supervised demonstration in a clinical setting) — meaning you are expected not merely to describe the clinical findings of heart failure but to perform the examination yourself, accurately and systematically. Every element of this module — history-taking, pulse assessment, BP measurement with recognition of pulsus paradoxus and alternans, JVP measurement, precordial palpation, and auscultation — is a competency you will be assessed on in your final MBBS clinical examination and, more importantly, will use on every ward call after qualification. An unrecognised raised JVP, a missed S3 gallop, or failure to detect pulsus alternans in a decompensated patient can delay the diagnosis that changes management. This is clinical medicine at its most essential.
RECALL
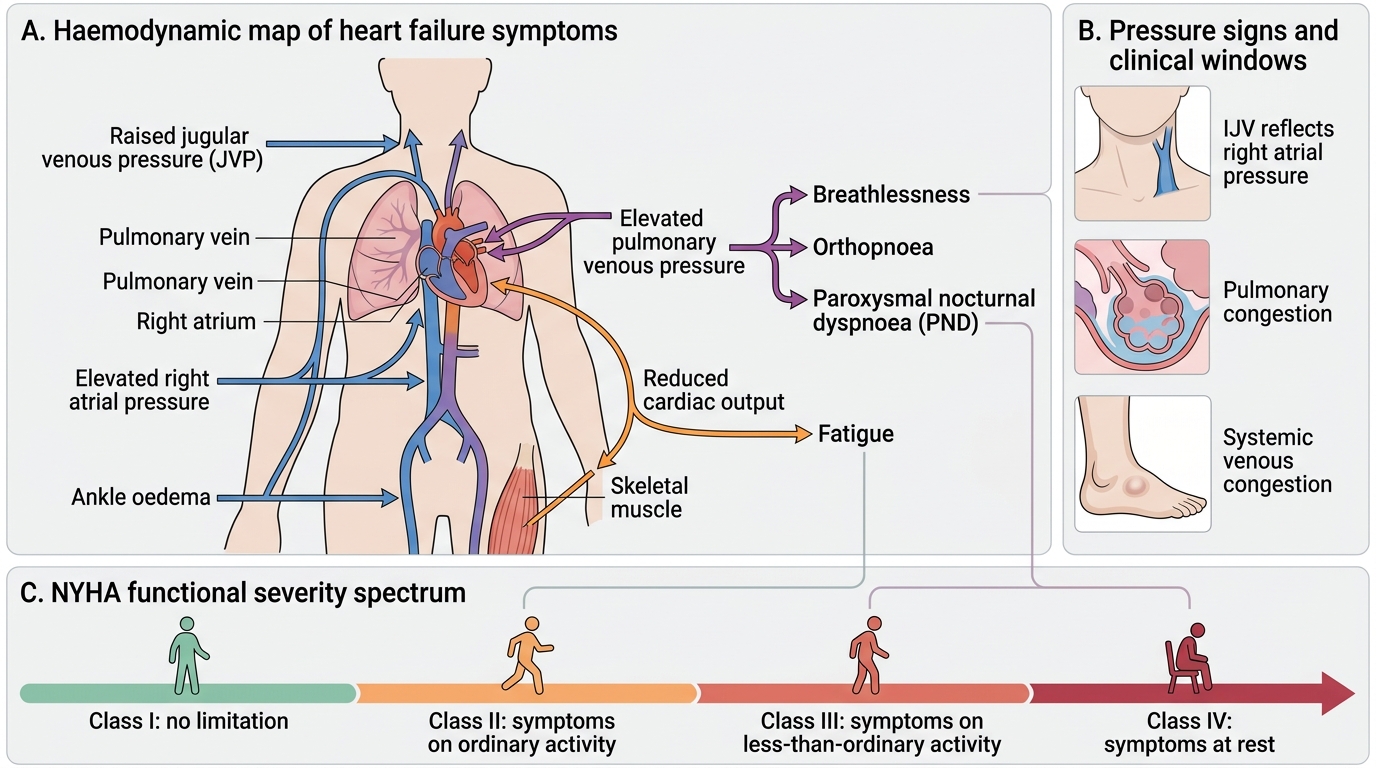
Before beginning the structured examination, activate your prior knowledge of the physiological substrate. The heart maintains cardiac output — the product of heart rate and stroke volume — and any failure of this pump affects both the forward flow (low output symptoms: fatigue, reduced effort tolerance) and the backward pressure (congestion: pulmonary oedema causing dyspnoea, systemic venous congestion causing JVP elevation and peripheral oedema). Recall the Frank-Starling mechanism: within physiological limits, increasing ventricular filling (preload) increases stroke volume; in heart failure, this mechanism is exhausted and the ventricle operates on a depressed Starling curve. Recall also that left-sided failure causes pulmonary congestion (dyspnoea, orthopnoea, PND, basal crepitations) while right-sided failure causes systemic venous congestion (raised JVP, hepatomegaly, peripheral oedema). Integrated CVS history and examination allows you to localise which side is predominantly failing, estimate severity (NYHA Class I–IV), and identify the underlying aetiology. Build on your knowledge of cardiac anatomy — the surface markings of the cardiac chambers, the auscultatory areas, and the production of heart sounds — as these underpin everything that follows.
When to Perform a Structured CVS Evaluation: Indications and Clinical Relevance
A structured cardiovascular system (CVS) evaluation for suspected heart failure is indicated whenever a patient presents with symptoms that suggest impaired cardiac pump function, elevated filling pressures, or both. Recognising these indications before approaching the patient is the first step of the IM-skills arc — the clinician who understands why they are examining will examine more purposefully and interpret more accurately.
The cardinal symptoms that mandate a focused CVS evaluation in the context of suspected heart failure are breathlessness, orthopnoea, paroxysmal nocturnal dyspnoea (PND), reduced exercise tolerance, ankle or leg swelling, and fatigue or weakness. Each of these maps to a specific haemodynamic derangement. Breathlessness on exertion reflects elevated left atrial and pulmonary venous pressure reducing lung compliance and triggering J-receptor activity in the lung parenchyma. Orthopnoea — breathlessness that worsens on lying flat — reflects the redistribution of interstitial fluid from the dependent parts of the body into the pulmonary circulation on recumbency, increasing pulmonary venous pressure. PND, which typically wakes the patient 1–3 hours after falling asleep, represents a more severe variant of the same mechanism, compounded by reduced adrenergic tone during sleep. The number of pillows required to sleep flat (the "pillow count") is a crude but clinically useful proxy for the severity of orthopnoea.
Additional symptoms that should trigger a CVS evaluation include palpitations (suggesting arrhythmia — atrial fibrillation is both a cause and a complication of heart failure), chest pain or heaviness (suggesting ischaemia as the underlying aetiology), abdominal distension or right upper quadrant discomfort (hepatic congestion from right heart failure), nocturia (redistribution of fluid from the periphery to the circulation when the patient lies supine at night, increasing renal perfusion and urine output), and weight gain (fluid retention as a marker of decompensation).
The urgency of evaluation scales with symptom acuity. A patient with acute breathlessness and oxygen saturation falling is an emergency; a patient with new-onset exertional dyspnoea in a known hypertensive requires the same structured approach but in an outpatient setting. The NYHA classification (Class I: no symptoms at ordinary activity; Class II: mild symptoms on ordinary exertion; Class III: symptoms on less-than-ordinary exertion; Class IV: symptoms at rest or minimal activity) provides the framework for estimating how urgently intervention is required.
Heart Failure Symptoms and Haemodynamic Mechanisms
Governing Principles: The Physiological Basis of Clinical Signs in Heart Failure
Every sign elicited in the cardiovascular examination of a heart failure patient has a specific physiological explanation. Understanding these explanations is not academic decoration — it is the mechanism that allows you to use each sign as a window into the patient's haemodynamics. A clinician who understands why the JVP is elevated will not merely note it as a positive finding but will use it to estimate right atrial pressure, gauge the response to treatment, and distinguish heart failure from other causes of a raised JVP. This section establishes the governing principles for each key sign before the technique of eliciting them is taught.
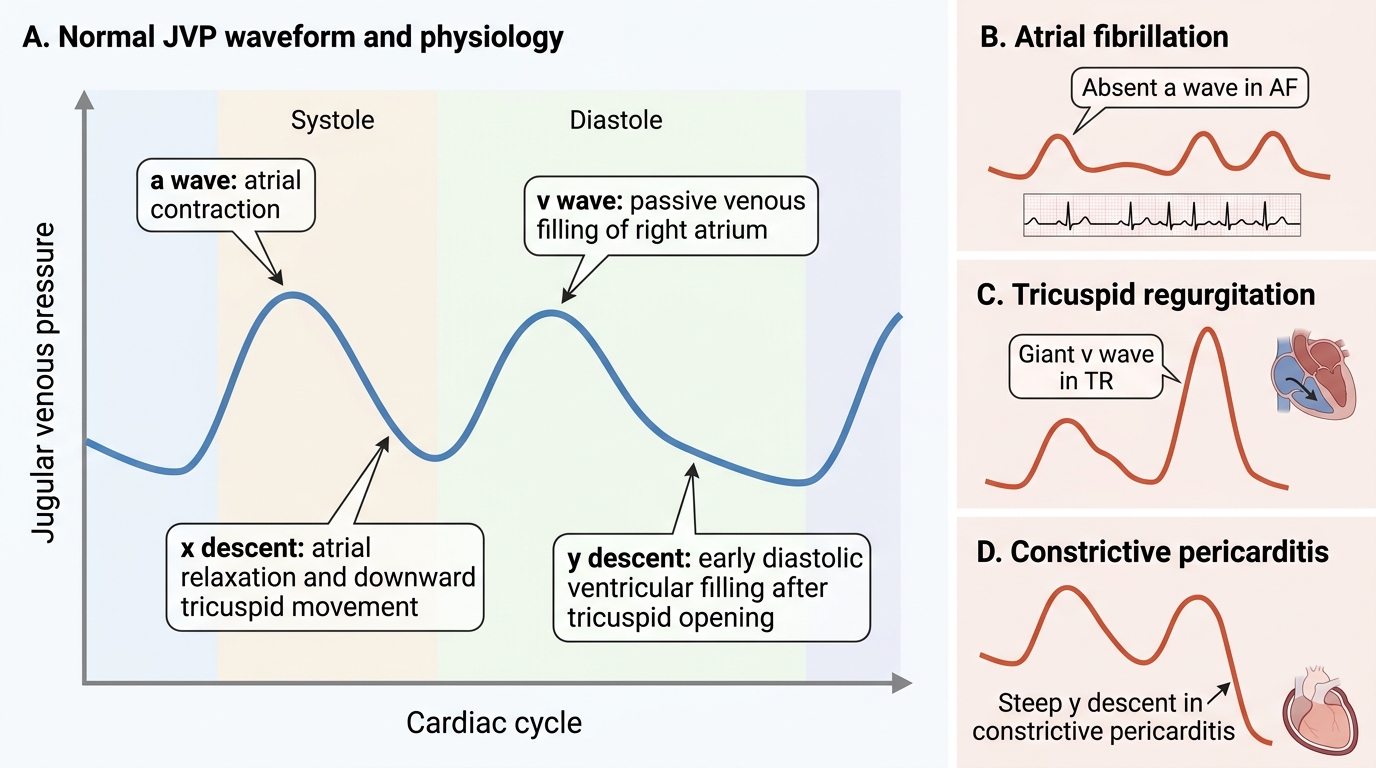
The jugular venous pulse and its physiological basis. The internal jugular vein (IJV) drains directly into the right atrium without intervening valves. The pressure in the IJV therefore reflects right atrial pressure directly. When the right heart fails — whether due to left heart failure causing pulmonary hypertension and secondary right heart strain, or due to primary right ventricular pathology, or due to pericardial disease (tamponade, constrictive pericarditis) — right atrial pressure rises and this is transmitted directly to the IJV. A normal JVP at 45° is ≤4 cm above the sternal angle (equivalent to ≤9 cm above the right atrium, using a fixed 5 cm correction for the sternal angle-to-RA distance). A raised JVP means elevated right atrial filling pressure, i.e., right ventricular preload excess. The JVP waveform carries additional information: the a wave reflects atrial contraction (absent in AF, giant in tricuspid stenosis and pulmonary hypertension), the x descent is active atrial relaxation, the v wave is passive filling of the atrium during ventricular systole (large v wave in tricuspid regurgitation — the regurgitant jet flows back into the right atrium), and the y descent is tricuspid valve opening with early diastolic ventricular filling (slow y descent in tricuspid stenosis; rapid steep y descent in constrictive pericarditis).
The third heart sound (S3) and its mechanism. The S3 gallop is the most specific sign for elevated left ventricular filling pressure and reduced left ventricular systolic function. It occurs in early diastole, during the period of rapid ventricular filling (the E phase of the E/A ratio on Doppler echocardiography). In a failing, dilated ventricle with reduced compliance, the sudden deceleration of the blood column rushing from the atrium into the ventricle causes vibration of the ventricular wall — this vibration is the S3. The S3 is best heard at the cardiac apex with the bell of the stethoscope (low-frequency sound), with the patient in the left lateral decubitus position. The presence of S3 in a patient over 40 years of age with cardiac symptoms should be treated as a sign of heart failure until proven otherwise. It was famously described as having the same rhythm as the word "Ken-tucky" — but the key clinical lesson is to listen specifically in early diastole after S2.
The fourth heart sound (S4) and diastolic dysfunction. The S4 is a late-diastolic sound produced by the atrial contraction into a stiff, non-compliant left ventricle — the A phase filling. It signifies impaired ventricular relaxation (diastolic dysfunction), as seen in hypertensive heart disease, hypertrophic cardiomyopathy, and severe concentric LV hypertrophy. S4 is absent in atrial fibrillation (no atrial contraction). The presence of both S3 and S4 ("summation gallop") at high heart rates is an ominous sign of severe LV dysfunction.
The apex beat — displacement, character, and significance. The apex beat is the outermost and lowest point of visible or palpable cardiac impulse. Normally it is in the 5th intercostal space at the mid-clavicular line. A displaced, diffuse, sustained apex beat reflects left ventricular dilatation and increased LV mass — the hallmark of systolic heart failure due to dilated cardiomyopathy or longstanding pressure/volume overload. A heaving (forceful, sustained) apex in its normal position suggests pressure overload (LVH from hypertension or aortic stenosis) without dilatation — the ventricle contracts powerfully but inefficiently. A parasternal heave (a sustained lift of the left parasternal region) indicates right ventricular hypertrophy from pulmonary hypertension.
Peripheral pulse variations and their mechanisms. The character of the pulse reflects the stroke volume and the rate of change of aortic pressure: pulsus alternans (alternating strong and weak beats in sinus rhythm) reflects severe LV systolic dysfunction — the failing ventricle cannot sustain a consistent stroke volume beat-to-beat. Pulsus paradoxus (an exaggerated fall in systolic BP of >10 mmHg during inspiration, detectable by pulse oximetry or auscultation with a sphygmomanometer) is the hallmark of cardiac tamponade — the fluid-filled pericardium makes both ventricles compete for a fixed space during inspiration, reducing LV stroke volume. A low-volume, rapid pulse suggests reduced cardiac output. A collapsing (water-hammer) pulse in wide-pulse-pressure states (aortic regurgitation, severe anaemia, AV fistula) reflects a high stroke volume ejected rapidly into a low-resistance circuit.
JVP Waveform: Physiology and Clinical Correlates
Procedure and Technique: Step-by-Step Bedside CVS Evaluation in Suspected Heart Failure
The structured CVS examination for suspected heart failure follows a systematic sequence: history, general inspection, pulse, blood pressure, JVP, precordial palpation, auscultation, and peripheral examination. Each step builds upon the preceding one, and no component should be skipped — a complete examination takes approximately 10–15 minutes when performed fluently.
Step 1 — History (IM1.8, IM1.26). Greet the patient and introduce yourself. Begin with open-ended questions: "Tell me about your breathing" and "What brings you here today?" Then systematically elicit: (a) presenting complaints with exact duration and progression; (b) dyspnoea: onset, relation to exertion (effort tolerance — how many metres or flights of stairs?), orthopnoea (number of pillows), PND (frequency, duration); (c) oedema: site of onset (feet, ankles, legs), rate of progression, pitting character; (d) palpitations: rate, rhythm, duration, precipitants; (e) chest pain or tightness and its characteristics; (f) precipitating and exacerbating factors — dietary indiscretion (salt, fluid), missed medications, intercurrent infection, ischaemic event, new drugs (NSAIDs, steroids, negative inotropes); (g) risk factors for underlying aetiologies: hypertension, diabetes, ischaemic heart disease, rheumatic fever in childhood, alcohol consumption, thyroid disease, family history of cardiomyopathy; (h) features of infective endocarditis — unexplained fever, rigors, weight loss, new regurgitant murmur, splinter haemorrhages, Janeway lesions, Osler nodes; (i) medication history including current cardiac drugs and adherence; (j) functional status: NYHA class derived from activities of daily living. Document all findings precisely for presentation.
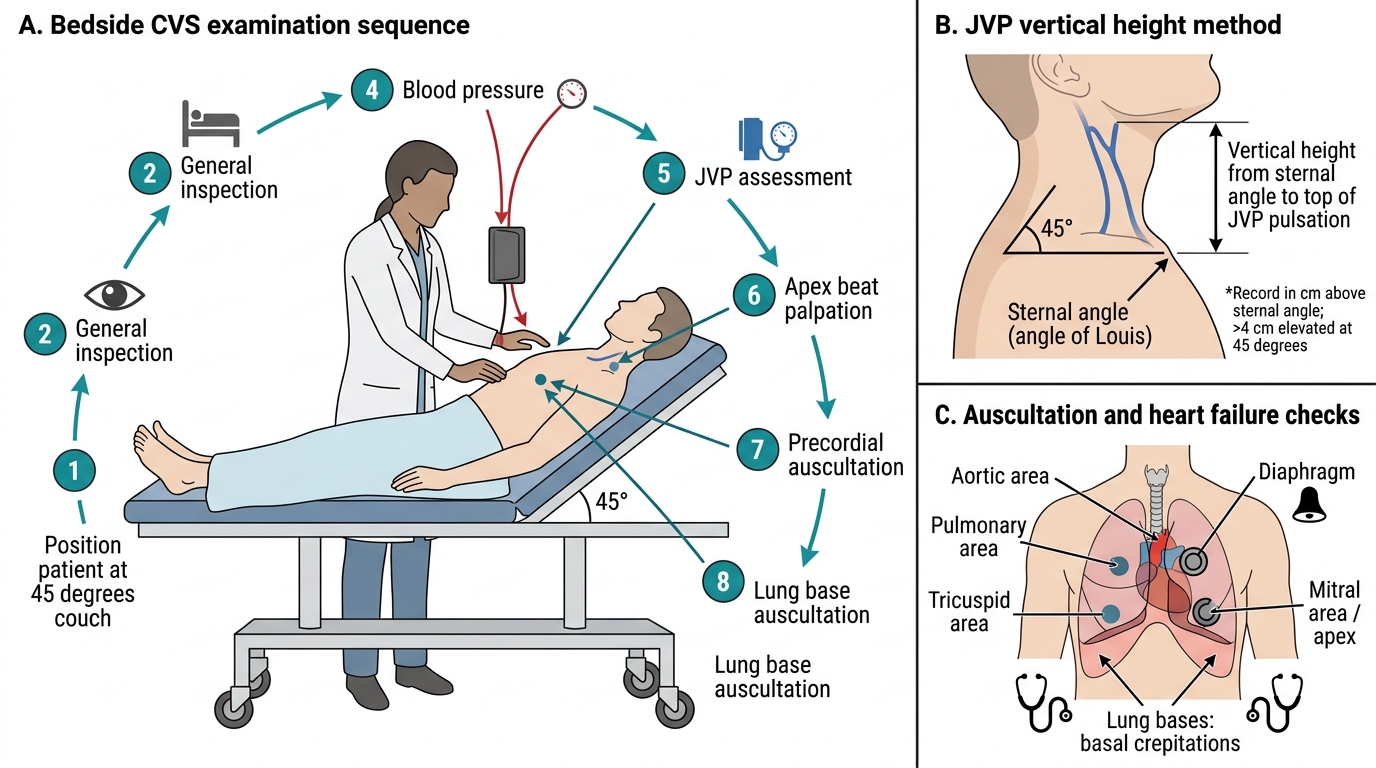
Step 2 — General inspection. Position the patient at 45° (essential for JVP). Observe at the foot of the bed: respiratory rate, use of accessory muscles, inability to complete full sentences (severe failure), nutritional status (cardiac cachexia in advanced failure), pallor (anaemia as precipitant), jaundice (hepatic congestion), and central cyanosis (examine the tongue for blue discolouration). Look for peripheral oedema (ankles, pretibial region, sacrum in bed-bound patients) and ascites (bulging flanks). Note any venous distension of the neck at this stage. Count and record the respiratory rate.
Step 3 — Peripheral pulse (IM1.10). Palpate the radial pulse with two or three fingers. Assess: (a) rate — count for 30 seconds and double; (b) rhythm — regular, regularly irregular (second-degree AV block), or irregularly irregular (atrial fibrillation — the most common rhythm in HF); (c) volume — small (reduced cardiac output), normal, or large/bounding (high-output states, aortic regurgitation); (d) character — plateau (slow-rising, aortic stenosis), collapsing/water-hammer (rapid upstroke + rapid collapse, aortic regurgitation; confirm by elevating the arm above the heart level), anachrotic (slow-rising with a notch, severe AS), pulsus bisferiens (double-peaked, HOCM or combined AR+AS); (e) check for pulsus alternans by lightly palpating — alternating strong and weak beats in sinus rhythm; (f) assess the left radial pulse — radio-radial delay suggests aortic arch pathology. Compare the radial to the carotid pulse character for confirmation of character abnormalities.
Step 4 — Blood pressure measurement (IM1.11). Use a properly calibrated sphygmomanometer. Select the correct cuff size (cuff bladder should encircle ≥80% of the arm circumference; an undersized cuff overestimates BP). Seat the patient with the arm at heart level. Palpate the brachial artery; inflate the cuff to 30 mmHg above the point where the radial pulse disappears. Place the stethoscope bell over the brachial artery. Deflate at 2 mmHg/second. Record: systolic BP = appearance of Korotkoff sound I (first clear tapping); diastolic BP = disappearance of sounds (Korotkoff V). Record in both arms (a >10 mmHg difference suggests subclavian stenosis or aortic dissection). Document pulse pressure (systolic − diastolic; widened >60 mmHg in AR, low <25 mmHg in cardiac tamponade or severe AS). Measure in both lying and standing positions to detect orthostatic hypotension (a fall of ≥20 mmHg systolic or ≥10 mmHg diastolic on standing). For pulsus paradoxus: inflate above systolic, deflate slowly; note the pressure at which sounds first appear only on expiration, then deflate further to note the pressure where sounds are heard throughout the respiratory cycle — a difference >10 mmHg is significant (tamponade, severe bronchospasm). For pulsus alternans: auscultate at the level where sounds are heard only in stronger beats; on further deflation, sounds should be heard on every beat — document the numerical difference.
Step 5 — Jugular venous pressure (IM1.12). Position the patient at 45° (not 90°, not 0°). Turn the head slightly to the left. Identify the internal jugular vein (IJV) — the IJV runs from the angle of the jaw to the clavicle in the triangle between the two heads of the sternocleidomastoid muscle. It is NOT visible as a tube (unlike the external jugular) but manifests as a subtle double-pulsation visible in the skin of the neck (the a and v waves). Distinguish JVP from carotid pulse: JVP has a double-pulsation visible at the neck (two elevations per cardiac cycle in sinus rhythm), is not palpable, can be abolished by gentle pressure at the base of the neck, and falls on inspiration in normal subjects. Measure: the vertical height of the uppermost point of pulsation above the sternal angle (of Louis) — a vertical line from the sternal angle, not a curved line along the neck. Normal JVP ≤4 cm above the sternal angle. A JVP >4 cm at 45° is elevated. If the JVP is very high, raise the patient to 90° — if the top of the pulsation is still visible, the JVP is markedly elevated. If the JVP is not visible at 45°, lay the patient to 30° — if it now becomes visible, the JVP is still elevated. The hepatojugular reflux (HJR) test: apply firm sustained pressure to the right upper quadrant for 10–15 seconds — a sustained rise in JVP of >4 cm for the duration of compression is positive and confirms elevated central venous pressure (CVP). Document: height in cm above the sternal angle, waveform pattern (if visible), and whether HJR is positive.
Step 6 — Precordial palpation (IM1.9). Stand at the right of the patient. Inspect for any visible pulsations (apex beat, sternal/parasternal lift). Palpate the apex beat using the palm and fingers: localise the outermost and lowest palpable impulse and record its position in intercostal space and relation to the mid-clavicular line. Assess character: tapping (normal), heaving/sustained (volume or pressure overload), thrusting (volume overload, AR), or absent/impalpable (COPD, obesity, pericardial effusion). Check for a parasternal heave (place the heel of the right hand over the left parasternal region — a sustained lift = RVH). Palpate for thrills (palpable murmurs): systolic thrill at the base (AS, PS), systolic thrill at the apex (MR), diastolic thrill at the apex (MS — rare). Palpate for the pulmonary component of the second heart sound (P2) — a palpable P2 at the pulmonary area indicates pulmonary hypertension.
Step 7 — Auscultation (IM1.13). Use both diaphragm (high-frequency sounds: S1, S2, AR, MR, systolic murmurs) and bell (low-frequency: S3, S4, MS, diastolic rumble). Auscultate in sequence at: (a) mitral area (cardiac apex, 5th ICS MCL) — S1 and S2 best heard, S3/S4 gallop, MS rumble, MR pan-systolic murmur; (b) tricuspid area (lower left sternal border, 4th-5th ICS) — TR pan-systolic, TS opening snap; (c) pulmonary area (left 2nd ICS) — P2 intensity, PS ejection systolic, pulmonary regurgitation (Graham-Steell murmur); (d) aortic area (right 2nd ICS) — A2 intensity, AS ejection systolic, AR early diastolic blowing murmur. For murmurs, systematically characterise: timing (systolic/diastolic/continuous), grade (I–VI for systolic; I–IV for diastolic using Levine grading), pitch (high/medium/low), quality (harsh, blowing, rumbling, musical), radiation (MR → axilla; AS → carotid; AR → 3rd-4th ICS LSB Erb's point; TR → does not radiate), and dynamic variation (murmurs increase with Valsalva release, exercise, straight leg raise; decrease with Valsalva strain). Left lateral decubitus position accentuates mitral murmurs (S3, S4, MS). Sitting forward in full expiration accentuates aortic regurgitation.
Step 8 — Peripheral examination. Examine for dependent pitting oedema (press for 10 seconds, grade 1+–4+ by depth and recovery time). Palpate the liver (hepatomegaly suggests RVH/congestion; pulsatile liver in TR). Percuss and measure ascites (shifting dullness, fluid thrill in gross ascites). Examine the lung bases posteriorly for basal crepitations (fine, inspiratory, bilateral, non-clearing with cough in pulmonary oedema — distinguish from coarse crepitations of pneumonia). Check for pleural effusion (bilateral in LVF; right-sided predominance in some cases).
Systematic Bedside CVS Examination in Suspected Heart Failure
SELF-CHECK
A 65-year-old man is being examined for suspected heart failure. His JVP is measured at 45°. The correct method for recording JVP height is to measure:
A. The curved distance along the neck surface from the clavicle to the uppermost pulsation
B. The vertical height from the sternal angle (of Louis) to the top of the venous pulsation
C. The horizontal distance from the sternocleidomastoid muscle to the pulse
D. The height from the right atrium directly to the top of the pulsation using ultrasound
Reveal Answer
Answer: B. The vertical height from the sternal angle (of Louis) to the top of the venous pulsation
JVP is measured as the vertical height from the sternal angle (angle of Louis) to the uppermost point of the JVP pulsation, regardless of the patient's position or the curvature of the neck. The sternal angle is used as a fixed anatomical reference because it lies approximately 5 cm above the right atrium in most positions. A JVP >4 cm above the sternal angle at 45° is elevated. The curved surface distance gives a falsely high reading and is not the accepted method. Ultrasound is not the bedside method for JVP estimation.