Page 1 of 25
IM1.1-7 | Heart Failure Foundations and Aetiology — SDL Guide
Learning Objectives
- Define and stage heart failure using LVEF-based classification (HFrEF ≤40%, HFmrEF 41–49%, HFpEF ≥50%), NYHA functional class I–IV, and ACC/AHA stages A–D
- Describe the epidemiology, aetiology, and pathogenesis of the common causes of heart failure including ischaemic, hypertensive, valvular (rheumatic), and cardiomyopathic
- Differentiate left from right heart failure and systolic from diastolic dysfunction in terms of mechanism, haemodynamics, and clinical features
- Explain the compensatory neurohormonal mechanisms (Frank-Starling, RAAS, SNS, BNP) and how they become maladaptive in chronic heart failure
- Enumerate and explain the factors that exacerbate heart failure: ischaemia, arrhythmias, anaemia, thyrotoxicosis, infection, dietary factors, and drugs
- Describe the pathogenesis of atrial fibrillation and ventricular arrhythmias in heart failure, apply the CHA₂DS₂-VASc score for anticoagulation decisions
- Outline a systematic diagnostic approach (BNP, ECG, CXR, echocardiography) and describe the principles of pharmacological and device management
INSTRUCTIONS
Heart failure is the final common pathway of numerous cardiac diseases and is one of the most important clinical syndromes in internal medicine. This module builds your understanding from the ground up: epidemiology and aetiology, the haemodynamic and neurohormonal mechanisms that drive symptoms, the three LVEF-based phenotypes that determine treatment, and the principles of evidence-based management. Competencies IM1.1–IM1.7 are all addressed — from defining and staging HF to understanding arrhythmias. Read actively: link each mechanism to the drug that blocks it, and connect each sign and symptom to its haemodynamic origin.
References
- Harrison's Principles of Internal Medicine, 21st ed., Chapters 252–253 — Heart Failure (textbook)
- API Textbook of Medicine, 10th ed., Section on Cardiology — Heart Failure (textbook)
- Davidson's Principles and Practice of Medicine, 24th ed., Chapter 18 — Heart Failure (textbook)
- ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2021 (guideline)
- ACC/AHA/HFSA Guideline for the Management of Heart Failure 2022 (guideline)
Version 1.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 58-year-old man with longstanding hypertension and diabetes presents to the emergency department at 2 AM, unable to lie flat for the past three nights. His wife says he has been sleeping propped up on four pillows. On examination he is breathless at rest, his neck veins are distended to the angle of the jaw, bilateral crackles are heard at both lung bases, and his ankles are swollen to the mid-shin. His chest X-ray shows cardiomegaly, upper lobe venous diversion, bilateral haziness, and a small right pleural effusion. His echocardiogram reports a left ventricular ejection fraction of 32%. He is in decompensated heart failure — but before you can treat him, you need to understand exactly which type of failure he has, why his heart arrived at this state, and what physiological storm is now keeping it there. Heart failure is not a single disease. It is the final common pathway of dozens of cardiac and systemic insults, and the student who understands its mechanisms — RAAS activation, sympathetic overdrive, ventricular remodelling — will understand not only how patients deteriorate but why every drug in the modern treatment armamentarium works.
WHY THIS MATTERS
Heart failure is one of the most common reasons for hospital admission in India and across the world. According to registry data from the Indian Heart Failure Registry (INDUS-HF), patients with heart failure in India tend to be younger than their Western counterparts (mean age approximately 53–55 years), have a higher prevalence of rheumatic valvular disease and ischaemic heart disease as underlying causes, and carry a 30-day in-hospital mortality of approximately 8–10%. For the final-year MBBS student, competency in heart failure spans NMC codes IM1.1–IM1.7: you must define and stage heart failure using LVEF-based and functional classification systems, distinguish left from right and systolic from diastolic failure, explain compensatory neurohormonal mechanisms, enumerate exacerbating factors, and describe the arrhythmic complications. This SDL covers the foundations — the epidemiology, pathophysiology, classification, and aetiological framework — that underpin all subsequent clinical decision-making in the diagnosis and management of heart failure.
RECALL
Before engaging with heart failure, activate what you already know about cardiac physiology. The cardiac output (CO) is the product of heart rate (HR) and stroke volume (SV). Stroke volume in turn depends on three determinants: preload (the ventricular filling pressure, governed by venous return and compliance), afterload (the resistance the ventricle must overcome to eject — primarily systemic vascular resistance in the left ventricle and pulmonary vascular resistance in the right ventricle), and contractility (the intrinsic force-generating capacity of the myocardium, independent of loading conditions). The Frank-Starling mechanism states that within physiological limits, greater ventricular filling stretches the myofibrils and increases the strength of the subsequent contraction — more preload → more SV. The left ventricle ejects against the systemic circulation (high pressure, high resistance), while the right ventricle ejects against the pulmonary circulation (low pressure, low resistance). Blood arrives at the left atrium via the pulmonary veins after gas exchange, and arrives at the right atrium via the superior and inferior venae cavae from the systemic circulation. Recall also that ejection fraction (EF) = SV / End-diastolic volume, expressed as a percentage; the normal LVEF is ≥55–60%. These physiological anchors will allow you to derive, rather than memorise, the mechanisms of heart failure.
Clinical Presentation of Heart Failure
Heart failure (HF) is a clinical syndrome in which the heart is unable to pump sufficient blood to meet the metabolic demands of the body, or can do so only at the cost of elevated filling pressures. This definition captures two key elements: impaired output and elevated venous back-pressure — and the symptoms of heart failure arise from both. A student who understands these two haemodynamic derangements can derive virtually every symptom and sign without rote memorisation.
The symptoms of heart failure are classically divided into those arising from forward failure (reduced cardiac output) and those arising from backward failure (elevated venous and capillary pressures upstream of the failing ventricle). In practice, both components coexist in most patients with established failure.
Symptoms from backward failure of the left ventricle (left heart failure — elevated pulmonary venous pressure):
- Dyspnoea on exertion is the cardinal symptom, arising from elevated pulmonary capillary wedge pressure and reduced pulmonary compliance. It is the earliest and most sensitive symptom.
- Orthopnoea — breathlessness that worsens on lying flat, relieved by sitting upright. Mechanism: lying flat redistributes fluid from the legs and splanchnic circulation into the pulmonary circulation, raising pulmonary venous pressure. Patients report the number of pillows they need to sleep comfortably — a semiquantitative severity marker.
- Paroxysmal nocturnal dyspnoea (PND) — sudden awakening from sleep 1–2 hours after lying down, with severe breathlessness and sometimes wheeze (cardiac asthma). Mechanism: same as orthopnoea but delayed — fluid redistribution plus reduced sympathetic tone and respiratory reserve during sleep.
- Acute pulmonary oedema — the extreme end of acute left heart failure: frothy pink sputum, severe respiratory distress, basal crackles, and in severe cases, diffuse wheeze. A medical emergency.
Symptoms from backward failure of the right ventricle (or biventricular failure — elevated systemic venous pressure):
- Bilateral ankle and pedal oedema — pitting, worse in the evening. Hepatomegaly, right upper quadrant discomfort from hepatic capsule stretch.
- Ascites in severe cases from portal venous hypertension.
- Anorexia and nausea from gut oedema and hepatic congestion.
Symptoms from forward failure (reduced cardiac output):
- Fatigue and exercise intolerance — inadequate skeletal muscle perfusion.
- Nocturia — supine redistribution of peripheral oedema at night increases renal perfusion and GFR.
- Cardiac cachexia in advanced failure — cytokine-mediated wasting.
- Confusion and cold peripheries in cardiogenic shock.
Physical signs in heart failure: On examination, look for displaced and diffuse apex beat (left ventricular dilatation), S3 gallop rhythm (pathological third heart sound — indicates elevated filling pressures and a volume-loaded ventricle; best heard at the apex in expiration), S4 gallop (stiff/non-compliant ventricle vibrating against atrial systole), elevated jugular venous pressure (JVP), bilateral crackles at the lung bases (not cleared by coughing), pitting oedema, hepatomegaly, and in severe cases pleural effusions (more common on the right due to bilateral lymphatic drainage asymmetry). Pulsus alternans — alternating strong and weak pulse — signals severe LV dysfunction.
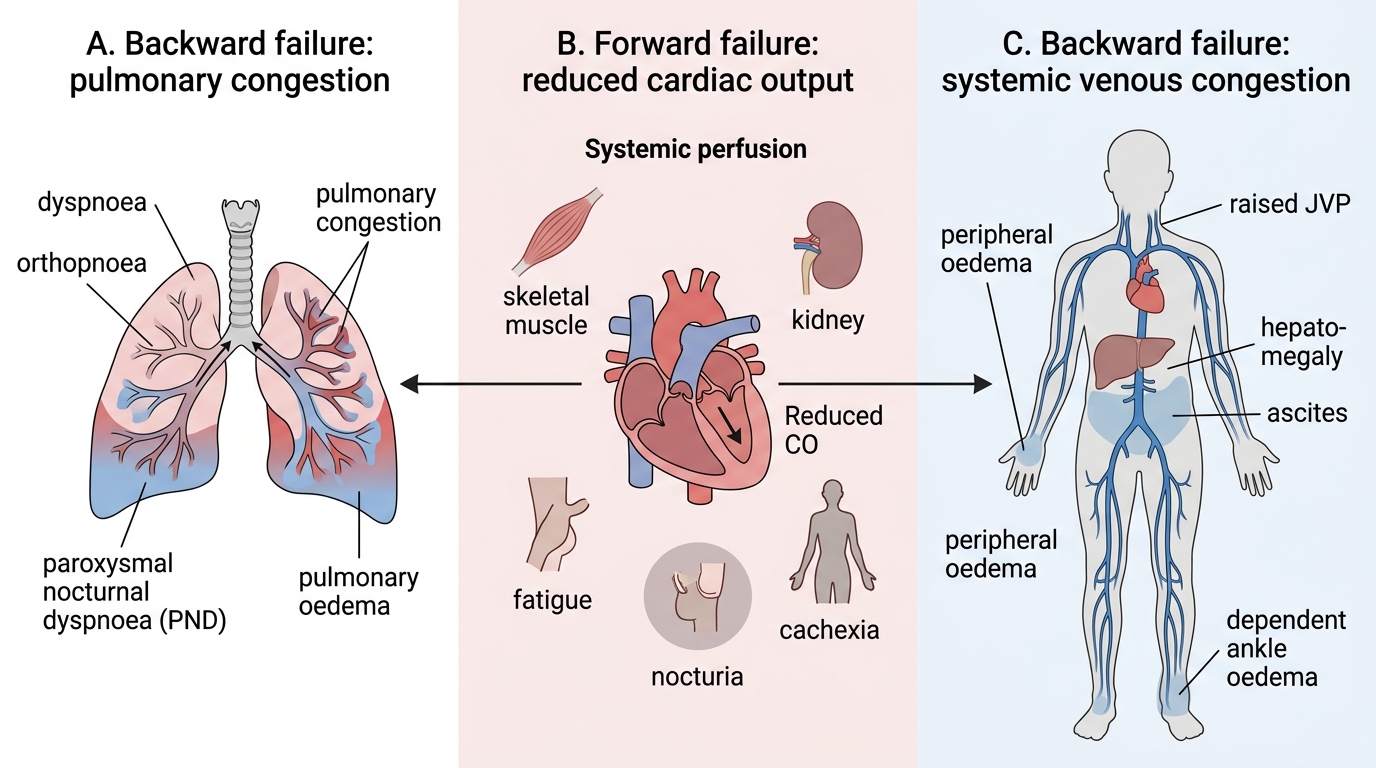
Forward and Backward Failure in Heart Failure
Defining and Staging Heart Failure: LVEF, NYHA, and ACC/AHA Systems
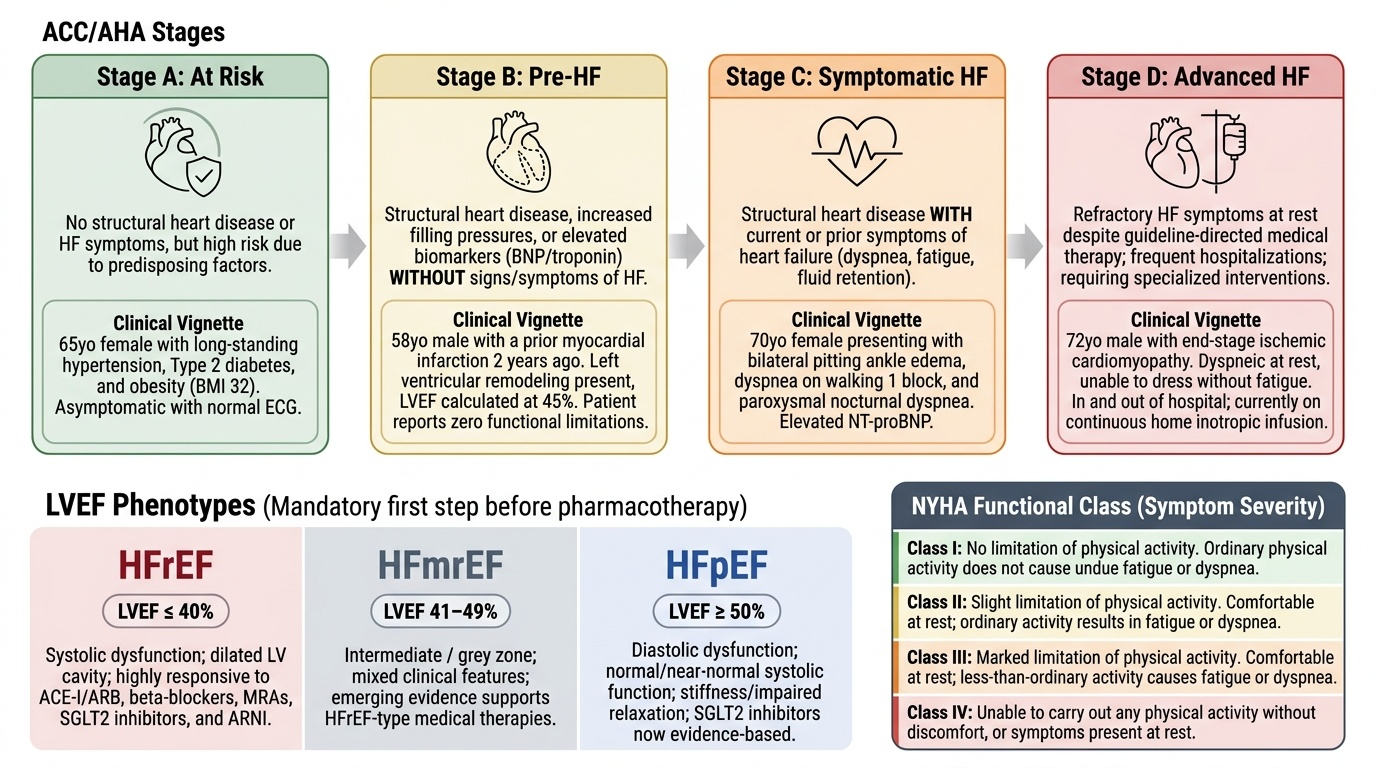
One of the most important conceptual advances in heart failure medicine over the past three decades is the recognition that heart failure encompasses at least three distinct phenotypes based on left ventricular ejection fraction (LVEF) — each with different epidemiology, natural history, and treatment response. The clinician must correctly classify the LVEF phenotype before selecting therapy, because the landmark drug trials that established evidence-based treatment (ACE inhibitors, beta-blockers, aldosterone antagonists) predominantly enrolled patients with reduced LVEF, and the efficacy of these agents in preserved LVEF failure remains more limited. The LVEF-based classification is now the starting framework for every heart failure assessment, and is embedded in both the ESC 2021 and ACC/AHA 2022 guideline algorithms as the mandatory first step before any pharmacotherapy decision.
Provided image
LVEF-based classification (ESC 2021 and ACC/AHA 2022 guidelines):
| LVEF Phenotype | LVEF Range | Abbreviation | Key characteristics |
|---|---|---|---|
| Heart failure with reduced ejection fraction | ≤40% | HFrEF | Systolic dysfunction; dilated LV; responds to ACE-I/ARB, beta-blockers, MRA, SGLT2-I, ARNI |
| Heart failure with mildly reduced ejection fraction | 41–49% | HFmrEF | Intermediate/grey zone; mixed features; emerging evidence for HFrEF-type therapy |
| Heart failure with preserved ejection fraction | ≥50% | HFpEF | Diastolic dysfunction; normal or near-normal systolic function; risk factor-driven; SGLT2-I now evidence-based |
The cut-off values are critical to memorise exactly: HFrEF ≤40%, HFmrEF 41–49%, HFpEF ≥50%. HFpEF is increasingly prevalent (now constituting more than 50% of heart failure diagnoses in developed countries), driven by the epidemics of hypertension, obesity, diabetes, and atrial fibrillation — all of which impair diastolic relaxation and ventricular compliance.
NYHA Functional Classification — the most widely used clinical severity grading system, assessing exercise tolerance:
| NYHA Class | Symptom description |
|---|---|
| Class I | No limitation of physical activity; ordinary activity does not cause symptoms |
| Class II | Slight limitation; comfortable at rest; ordinary activity causes dyspnoea, fatigue, or palpitation |
| Class III | Marked limitation; comfortable at rest; less-than-ordinary activity causes symptoms |
| Class IV | Symptoms at rest; any physical activity causes discomfort |
NYHA classification is used for monitoring disease progression, gauging prognosis, and as an eligibility criterion in clinical trials and for device therapy. It is subjective but reproducible and clinically actionable.
ACC/AHA Staging System (2022) — a complementary staging framework that tracks the structural and functional trajectory from risk factors to end-stage disease:
| Stage | Description | Example |
|---|---|---|
| Stage A (At risk) | Risk factors present; no structural heart disease or symptoms | Hypertension, diabetes, family history |
| Stage B (Pre-HF) | Structural heart disease present; no symptoms of HF | Asymptomatic LV dysfunction, previous MI |
| Stage C (Symptomatic HF) | Structural disease + prior or current HF symptoms | Established HF managed medically |
| Stage D (Advanced HF) | Refractory HF requiring specialised interventions | Inotrope-dependent, LVAD, transplant candidacy |
The ACC/AHA stages are unidirectional and progressive (Stage A → D), whereas NYHA class can fluctuate with treatment. Stages A–B represent the window for primary and secondary prevention; Stages C–D are active heart failure management territory. The practical integration: a patient may be ACC/AHA Stage C, NYHA Class II HFrEF — each descriptor adds a different dimension.
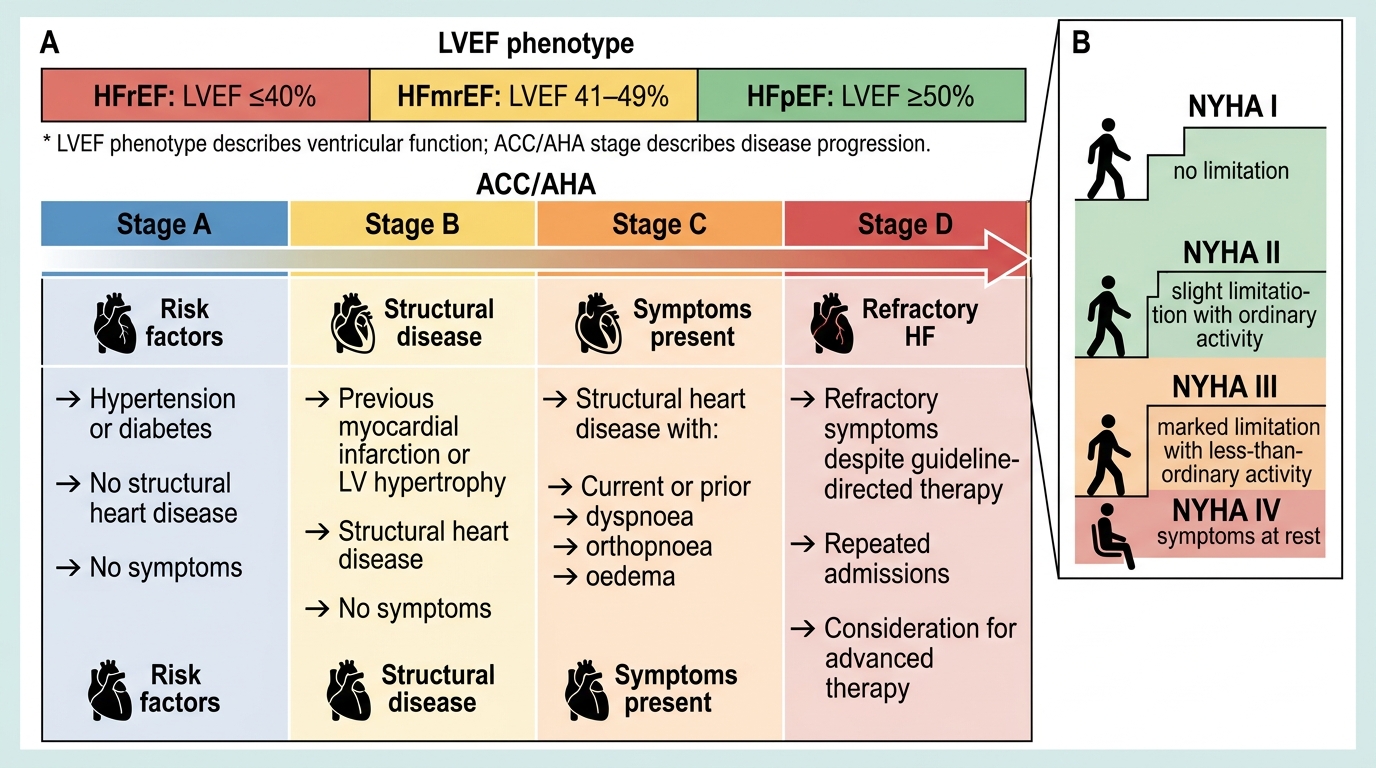
Heart Failure Classification: LVEF Phenotypes, ACC/AHA Stages, and NYHA Class
Pathophysiology and Aetiology: Left vs Right, Systolic vs Diastolic Failure
Understanding heart failure requires distinguishing two orthogonal axes: the anatomical axis (left vs right ventricle) and the functional axis (systolic vs diastolic dysfunction). These axes are independent — left heart failure and right heart failure have different clinical presentations, different aetiologies, and different treatment approaches. Similarly, systolic and diastolic dysfunction can occur in isolation or together.
Left heart failure arises from failure of the left ventricle to maintain adequate systemic output against the high-pressure systemic circulation. The immediate upstream consequence is elevation of left ventricular end-diastolic pressure (LVEDP), which raises left atrial pressure, which in turn raises pulmonary capillary wedge pressure (PCWP). When PCWP exceeds the oncotic pressure of plasma (approximately 25–30 mmHg), fluid transudates into the pulmonary interstitium and alveoli — producing pulmonary oedema. The symptoms, as described above, are predominantly respiratory (dyspnoea, orthopnoea, PND). The common causes of left heart failure include ischaemic heart disease (most common in India), hypertension, dilated cardiomyopathy, valvular disease (aortic stenosis/regurgitation, mitral regurgitation), and tachyarrhythmias. The ECG, chest X-ray, and echocardiogram are the diagnostic triad.
Right heart failure arises from failure of the right ventricle to maintain adequate pulmonary arterial flow against the pulmonary vascular resistance. The upstream consequence is elevation of right atrial pressure and systemic venous pressure. The clinical manifestations are those of systemic venous congestion: elevated JVP, hepatomegaly (and eventually cirrhosis — cardiac cirrhosis — in chronic severe right failure), ascites, and dependent oedema. The most important cause of isolated right heart failure is cor pulmonale — right ventricular failure secondary to chronic lung disease (COPD, interstitial lung disease, pulmonary hypertension). In clinical practice, however, the most common cause of right heart failure is left heart failure — because elevated pulmonary venous pressure from left failure raises pulmonary arterial pressure, eventually overloading the right ventricle. Hence biventricular failure (the classical congestive heart failure picture) is more common than isolated right or left failure in practice.
Systolic dysfunction is impairment of ventricular contraction — the ventricle fails to eject adequately, producing a reduced LVEF (≤40% = HFrEF). The ventricle typically dilates (to maintain stroke volume via the Frank-Starling mechanism), resulting in an eccentric hypertrophy / dilated pattern. Causes: ischaemic cardiomyopathy, dilated cardiomyopathy (idiopathic or secondary to alcohol, viral myocarditis, peripartum), chronic valvular regurgitation.
Diastolic dysfunction is impairment of ventricular relaxation and compliance — the ventricle fails to fill adequately at normal filling pressures, even though systolic contraction may be preserved (LVEF ≥50% = HFpEF). Cardiac output can be maintained only by raising filling pressure, causing pulmonary venous hypertension. The ventricle typically shows concentric hypertrophy (increased wall thickness, normal or reduced cavity size). Causes: hypertension (the most common), hypertrophic cardiomyopathy (HCM), infiltrative disease (amyloid — a classic cause of restrictive physiology), pericardial constriction, diabetes.
Key aetiological framework for heart failure (IM1.1 and IM1.2):
- Ischaemic heart disease / coronary artery disease: commonest cause worldwide and in urban India; acute MI causes acute systolic dysfunction; chronic myocardial ischaemia causes ischaemic cardiomyopathy.
- Hypertension: the most common risk factor, leading to diastolic dysfunction and HFpEF; also a cause of LV hypertrophy and eventual systolic dysfunction.
- Rheumatic valvular disease: particularly important in India and Southeast Asia; mitral stenosis is the archetypical cause; mitral regurgitation, aortic regurgitation, and aortic stenosis all cause heart failure through volume or pressure overload. Rheumatic fever (Group A Streptococcus) causes carditis via molecular mimicry — anti-streptococcal antibodies cross-react with cardiac valve antigens (primarily M-protein of Group A Streptococcus). The Jones Criteria (Revised, 2015) are used for diagnosis. Secondary prophylaxis with benzathine penicillin is mandatory to prevent recurrent rheumatic fever and progressive valvular damage.
- Dilated cardiomyopathy (DCM): idiopathic in the majority; secondary causes include alcohol (toxic cardiomyopathy), viral myocarditis (Coxsackie B, adenovirus, HIV), peripartum cardiomyopathy, anthracycline chemotherapy toxicity, haemochromatosis.
- Hypertrophic cardiomyopathy (HCM): autosomal dominant; mutations in sarcomere proteins (beta-myosin heavy chain, myosin-binding protein C); concentric hypertrophy, diastolic dysfunction, dynamic LVOTO; risk of sudden cardiac death.
- Inflammatory / myocarditis: viral, autoimmune (systemic lupus erythematosus), Chagas disease (Trypanosoma cruzi — relevant in endemic regions), giant-cell myocarditis.
- Congenital heart disease: adult presentations include secundum ASD, VSD, PDA, Eisenmenger syndrome.
- High-output states that precipitate failure in a diseased heart: severe anaemia, thyrotoxicosis, beriberi (thiamine deficiency), arteriovenous fistulae, Paget's disease.
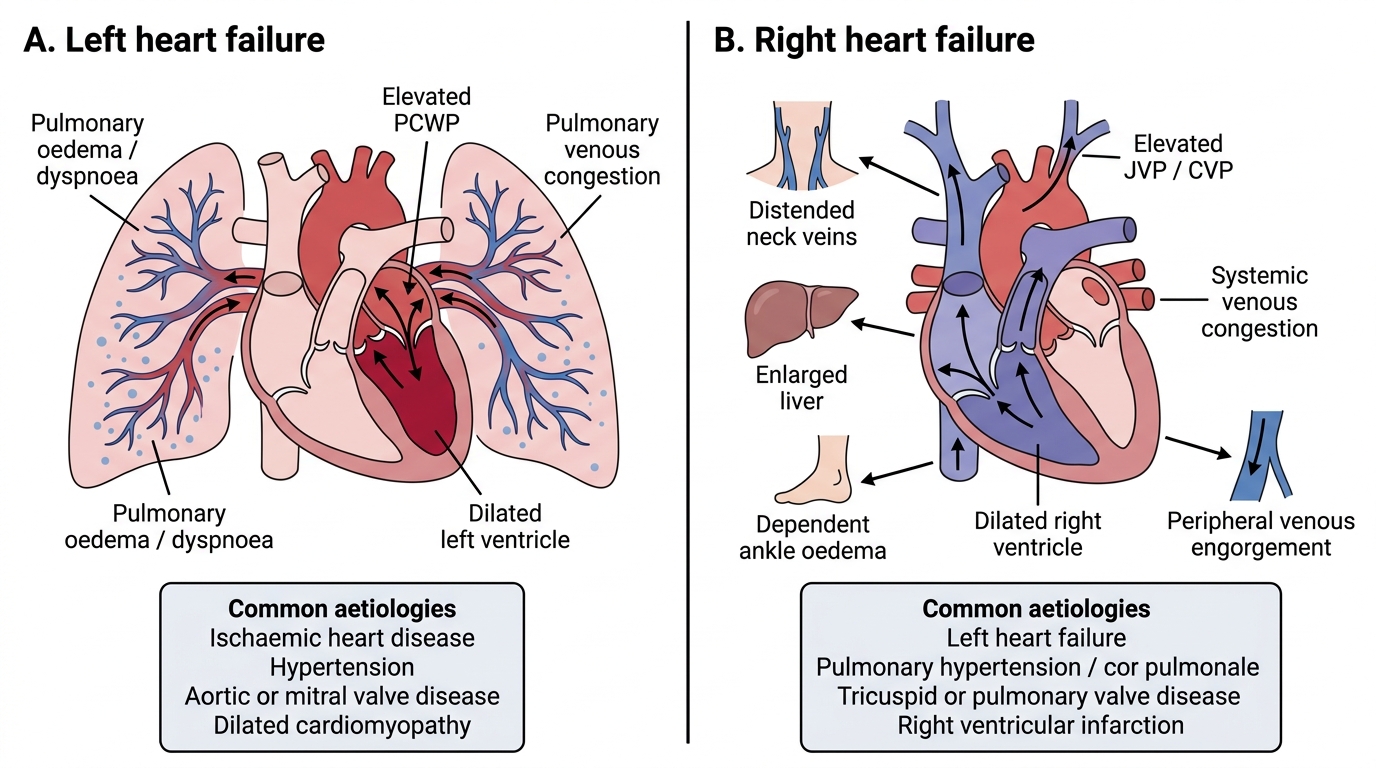
Left versus Right Heart Failure