Page 3 of 25
IM1.1-7 | Heart Failure Foundations and Aetiology — SDL Guide (Part 3)
Diagnosis and Investigation of Heart Failure
The diagnosis of heart failure is clinical, supported by investigations that confirm the structural and functional abnormality, identify the underlying cause, grade severity, and guide management. No single test diagnoses heart failure in isolation; the assessment integrates history, examination, biomarkers, ECG, chest radiograph, and echocardiography. For the finals student, the diagnostic approach must be systematic and linked to the LVEF phenotype classification.
Step 1 — Clinical assessment: The history and examination provide the pretest probability. Symptoms of pulmonary congestion (orthopnoea, PND, dyspnoea) combined with signs (elevated JVP, S3, pulmonary crackles, oedema) generate a strong clinical suspicion. The Framingham criteria are a useful bedside diagnostic framework: major criteria (PND/orthopnoea, elevated JVP, pulmonary crackles, cardiomegaly, S3, hepatojugular reflux, acute pulmonary oedema) and minor criteria (bilateral ankle oedema, nocturnal cough, dyspnoea on ordinary exertion, hepatomegaly, pleural effusion, tachycardia ≥120 bpm). Diagnosis requires 2 major criteria, or 1 major + 2 minor criteria.
Step 2 — Natriuretic peptides (BNP and NT-proBNP): BNP and NT-proBNP are the most important serum biomarkers in heart failure. Their diagnostic utility is highest in an undifferentiated patient presenting with dyspnoea — a normal BNP (<35 pg/mL) or NT-proBNP (<125 pg/mL) has a very high negative predictive value for HF and argues strongly for an alternative aetiology of dyspnoea. Elevated levels support the diagnosis and correlate with severity. NT-proBNP levels vary by age: cut-offs for acute HF are >450 pg/mL (<50 years), >900 pg/mL (50–75 years), >1800 pg/mL (>75 years). Falsely low BNP/NT-proBNP can occur in obesity and in acute flash pulmonary oedema (inadequate time for peptide rise).
Step 3 — 12-lead ECG: The ECG is not diagnostic of HF but identifies causative arrhythmias (AF), prior MI (Q waves), LV hypertrophy (voltage criteria, ST-T changes), bundle branch blocks (LBBB is a marker of dyssynchrony and a CRT indication criterion), and pericardial/infiltrative disease (low voltage in amyloid). A completely normal ECG has a high negative predictive value against significant cardiac dysfunction.
Step 4 — Chest radiograph (CXR): The CXR in heart failure shows a characteristic constellation: cardiomegaly (cardiothoracic ratio >0.5), upper lobe venous diversion (vessels in the upper zones are more prominent than lower zones — the opposite of normal, because elevated LVEDP redirects blood away from the congested lower lobes), Kerley B lines (short, horizontal lines at the lung bases — engorged interlobular lymphatics from interstitial oedema), perihilar haze (bat-wing shadow), bilateral pleural effusions (often right-sided or bilateral, rarely left-sided alone), and in severe pulmonary oedema, alveolar shadowing.
Step 5 — Echocardiography: The 2D transthoracic echocardiogram (TTE) is the cornerstone investigation for heart failure. It directly assesses: LVEF (by Simpson's biplane volumetric method — the reference standard), LV dimensions (dilation vs hypertrophy vs normal), wall motion abnormalities (regional = ischaemic; global = dilated cardiomyopathy), diastolic function parameters (E/A ratio, E/e' ratio, LA volume index — used to diagnose and grade diastolic dysfunction), valvular pathology (stenosis, regurgitation), pericardial effusion, RV size and function, and estimated RVSP (tricuspid regurgitation jet velocity → pulmonary artery pressure via modified Bernoulli equation). Stress echocardiography can unmask ischaemia as a cause of wall motion abnormalities. Transesophageal echocardiogram (TOE) is used when TTE quality is inadequate or for detailed valve assessment (infective endocarditis vegetation, mitral valve morphology).
Step 6 — Additional investigations:
- Full blood count, renal function, electrolytes, liver function, thyroid function: Identifies anaemia, renal failure, electrolyte abnormalities (hypokalaemia, hyponatraemia as severity marker), liver congestion, thyroid disease.
- Coronary angiography / CT coronary angiography: To establish ischaemic aetiology and determine revascularisation candidacy — the most important investigation before labelling a new-onset HFrEF as 'idiopathic dilated cardiomyopathy'.
- Cardiac MRI: The gold standard for myocardial viability, fibrosis characterisation (gadolinium late enhancement — differentiates ischaemic scar from non-ischaemic fibrosis, identifies amyloid, sarcoid, myocarditis), and accurate LVEF measurement when echocardiography is technically limited.
- Nuclear cardiology (myocardial perfusion scintigraphy / radionuclide ventriculography): Assessment of myocardial ischaemia and LVEF (MUGA scan) — useful when echo is limited; less available in India.
- Exercise stress testing: Functional capacity assessment (peak VO₂ on cardiopulmonary exercise testing — the gold standard prognostic marker in HF; peak VO₂ <10 mL/kg/min = high risk, warrants transplant evaluation); also unmasks coronary disease.
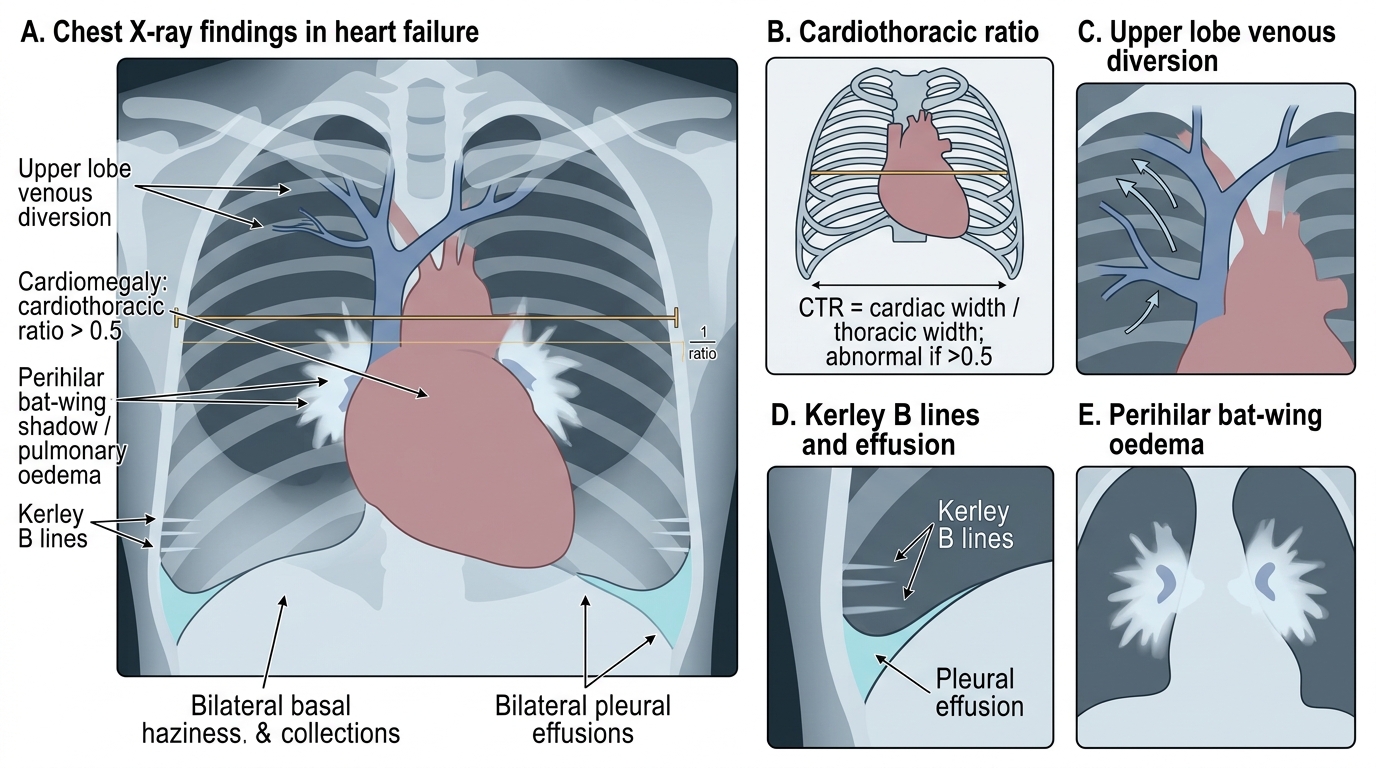
Chest X-Ray Findings in Heart Failure
SELF-CHECK
A 70-year-old woman presents with 3 weeks of progressive dyspnoea. On CXR: cardiomegaly and upper lobe venous diversion. Echocardiogram shows LVEF 55%, normal wall motion, concentric LV hypertrophy (wall thickness 13 mm), and diastolic dysfunction (elevated E/e' ratio 16, LA volume index elevated). Serum NT-proBNP is 980 pg/mL. What is the MOST accurate diagnosis?
A. Heart failure with reduced ejection fraction (HFrEF) secondary to hypertensive heart disease
B. Heart failure with mildly reduced ejection fraction (HFmrEF)
C. Heart failure with preserved ejection fraction (HFpEF) secondary to diastolic dysfunction
D. Non-cardiac cause of dyspnoea — echocardiogram is normal
Reveal Answer
Answer: C. Heart failure with preserved ejection fraction (HFpEF) secondary to diastolic dysfunction
LVEF 55% (≥50%) = HFpEF by definition. The echo shows concentric LV hypertrophy, elevated E/e' ratio, and elevated LA volume index — all diagnostic features of diastolic dysfunction (impaired LV relaxation and filling). NT-proBNP 980 pg/mL is above the diagnostic threshold for a 70-year-old (>900 pg/mL for age 50–75), confirming heart failure. HFrEF requires LVEF ≤40%. HFmrEF requires LVEF 41–49%. The echocardiogram is not normal — it shows structural and functional abnormalities consistent with diastolic dysfunction.
Principles of Management of Heart Failure
The management of heart failure has been transformed over the past 30 years from a purely symptomatic endeavour to a disease-modifying strategy that reduces hospitalisation, reverses ventricular remodelling, and prolongs life. Current management is built on four evidence-based pharmacological pillars for HFrEF and a risk-factor–modification approach for HFpEF, supplemented by non-pharmacological measures and device therapy for selected patients. For the finals student, it is essential to link each drug class to its mechanism, its target within the compensatory cascade, and its proven outcome benefit. This mechanistic understanding — knowing that ACE inhibitors block Ang II, beta-blockers counter catecholamine toxicity, and MRAs prevent aldosterone-driven fibrosis — transforms pharmacotherapy from a memorisation exercise into a logical, retrievable structure that will serve you both in examinations and at the bedside.
Non-pharmacological management (IM1.21):
- Sodium restriction: No more than 2–3 g sodium per day (approximately 5–6 g of table salt), to reduce fluid retention and oedema.
- Fluid restriction: 1.5–2 litres per day in patients with advanced HF or hyponatraemia.
- Daily weight monitoring: Patients should weigh themselves every morning; a weight gain of ≥2 kg over 48 hours warrants urgent review and diuretic dose adjustment (patient self-management education).
- Physical activity: Supervised cardiac rehabilitation and aerobic exercise training improve functional capacity, reduce hospitalisation, and improve quality of life — exercise is NOT contraindicated in stable compensated HF; bed rest worsens deconditioning.
- Vaccination: Influenza and pneumococcal vaccines to reduce infective exacerbations.
- Smoking cessation, alcohol abstinence (especially in alcohol-related cardiomyopathy), weight reduction in obesity (a major driver of HFpEF).
The four disease-modifying drug pillars for HFrEF (LVEF ≤40%):
| Drug class | Mechanism | Landmark trial | Outcome benefit |
|---|---|---|---|
| ACE inhibitor (e.g. enalapril, ramipril) or ARB (e.g. candesartan) if ACE-I intolerant | Blocks RAAS: reduces Ang II, aldosterone; reduces afterload + preload; prevents remodelling | CONSENSUS, SOLVD | Reduces mortality ~25%; reverses remodelling |
| Beta-blocker (e.g. carvedilol, bisoprolol, metoprolol succinate) | Blocks SNS: reduces HR, reduces catecholamine toxicity; reverse remodelling (improves LVEF over 3–6 months) | MERIT-HF, COPERNICUS | Reduces all-cause mortality ~35%; reduces SCD |
| Mineralocorticoid receptor antagonist (MRA; e.g. spironolactone, eplerenone) | Blocks aldosterone: reduces sodium retention, prevents cardiac fibrosis | RALES, EPHESUS | Reduces mortality ~30% in severe HFrEF; reduces hospitalisation |
| SGLT2 inhibitor (e.g. empagliflozin, dapagliflozin) | Reduces cardiac preload (osmotic diuresis/natriuresis); multiple cardioprotective mechanisms | EMPEROR-Reduced, DAPA-HF | Reduces HF hospitalisation + CV death ~25% |
For patients with HFrEF who remain symptomatic on ACE-I + beta-blocker, the ARNI (angiotensin receptor-neprilysin inhibitor, sacubitril-valsartan / Entresto) replaces the ACE inhibitor and further reduces mortality vs enalapril (PARADIGM-HF trial).
Diuretics: Loop diuretics (furosemide) are the mainstay of symptomatic relief in acute and chronic HF — they reduce venous congestion, relieve dyspnoea, and reduce weight. Furosemide does not have proven mortality benefit but dramatically improves symptoms. Thiazide diuretics (hydrochlorothiazide) are added for diuretic resistance. Monitor electrolytes (hypokalaemia, hypomagnesaemia) and renal function during diuresis.
Digoxin (cardiac glycoside): Inhibits Na-K-ATPase; increases intracellular calcium → increased contractility (positive inotrope); slows AV node conduction (rate control in AF). Proven to reduce HF hospitalisation (DIG trial) but no mortality benefit. Role now limited to rate control in HF with AF and symptoms refractory to standard therapy. Narrow therapeutic window; digoxin toxicity (arrhythmias, nausea, visual disturbance — xanthopsia) requires careful monitoring; target level 0.5–0.9 ng/mL.
HFpEF management: No drug has demonstrated clear mortality reduction. Management focuses on: diuretics for congestion relief, aggressive treatment of underlying risk factors (hypertension — target BP <130/80 mmHg, diabetes, obesity, AF rate/rhythm control), and SGLT2 inhibitors (empagliflozin in EMPEROR-Preserved, dapagliflozin in DELIVER) — now the only drug class with evidence for reducing hospitalisation in HFpEF.
Device therapy:
- ICD (implantable cardioverter-defibrillator): Indicated for primary prevention of SCD in HFrEF LVEF ≤35% despite 3 months of optimal medical therapy, NYHA Class II–III. Reduces sudden cardiac death.
- CRT (cardiac resynchronisation therapy): Biventricular pacing for patients with LVEF ≤35%, LBBB morphology with QRS ≥150 ms, NYHA Class II–III. Corrects interventricular dyssynchrony, reverses remodelling, improves LVEF, reduces mortality.
- LVAD (left ventricular assist device): Bridge to transplantation or destination therapy in Stage D HFrEF refractory to all medical therapy.
Management of acute decompensated HF: In the acute setting, the priorities are: (1) Position — sit patient upright (reduces preload, improves respiratory mechanics); (2) Oxygen for hypoxaemia; (3) IV furosemide (20–40 mg IV to start) for rapid diuresis; (4) IV vasodilators (GTN/nitroglycerin) for hypertensive acute pulmonary oedema; (5) Non-invasive ventilation (CPAP/BiPAP) for respiratory failure; (6) Identify and treat precipitant.
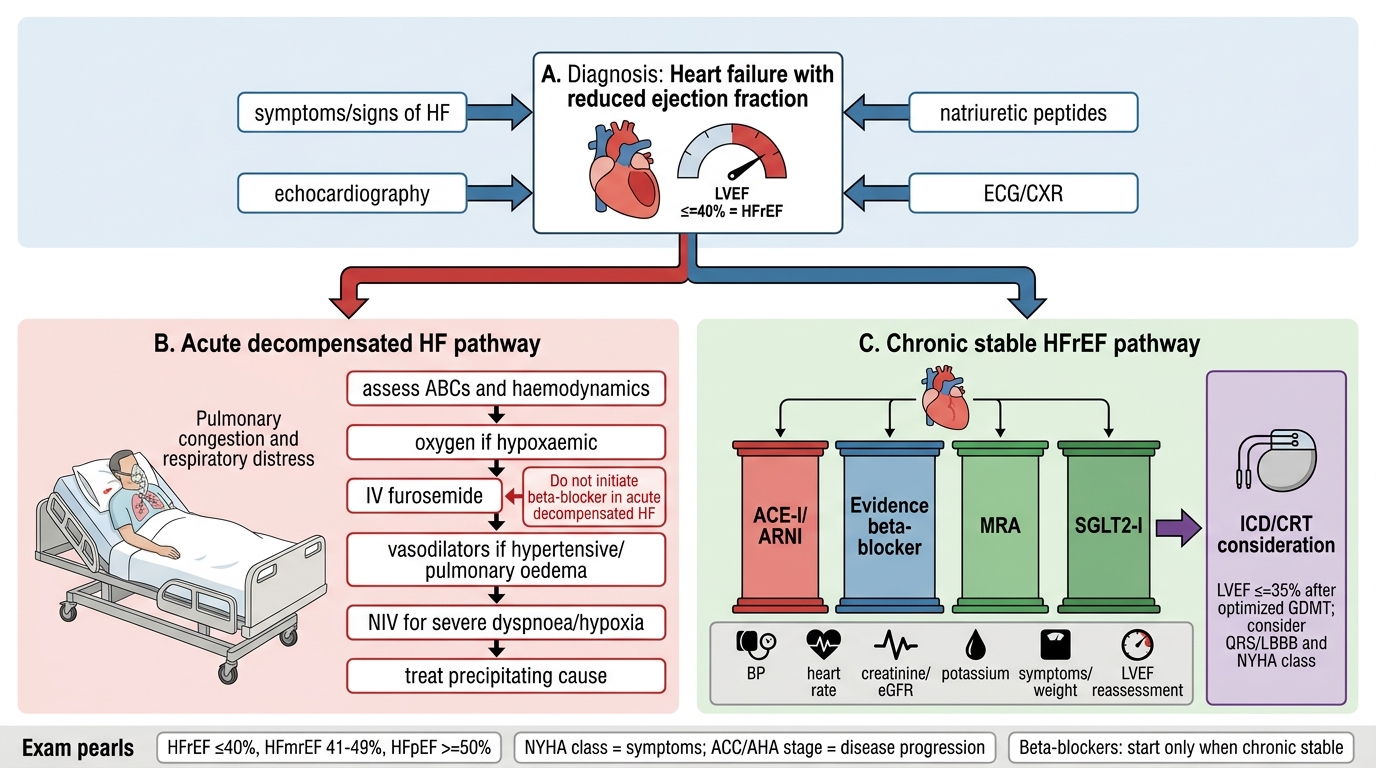
HFrEF Management Algorithm
CLINICAL PEARL
Three high-yield clinical distinctions that frequently appear in examinations and that many students confuse:
1. LVEF cut-offs must be exact: HFrEF is ≤40%, HFmrEF is 41–49%, HFpEF is ≥50%. An LVEF of 40% = HFrEF. An LVEF of 41% = HFmrEF, not HFrEF. The boundary matters because drug trial evidence — ACE inhibitors, beta-blockers, MRA — was built in LVEF ≤40% populations.
2. NYHA class vs ACC/AHA stage are NOT interchangeable: NYHA class describes current symptom burden and fluctuates with treatment; ACC/AHA stage describes structural disease progression and is unidirectional. A patient can be Stage C, NYHA Class I (previously symptomatic but now fully compensated on optimal therapy). Never say 'Stage II heart failure' using NYHA and ACC/AHA terminology interchangeably.
3. Beta-blockers in acute decompensated HF: Beta-blockers are life-saving in chronic stable HFrEF (MERIT-HF, COPERNICUS), but they must NEVER be initiated in acute decompensated heart failure — their negative inotropic effect will worsen haemodynamic instability. If a patient is already on a beta-blocker and presents with acute decompensation, the dose should be halved (or maintained if haemodynamically stable) but NOT abruptly stopped (risk of rebound sympathetic activation). Start beta-blockers only when the patient is euvolaemic, stable, and out of hospital.
Self-Assessment: Integrating Heart Failure Foundations
You have now covered the complete foundations of heart failure: epidemiology and aetiology, LVEF-based and functional staging, the pathophysiology of left versus right and systolic versus diastolic failure, the neurohormonal compensatory mechanisms and their maladaptive consequences, the exacerbating factors that precipitate decompensation, the arrhythmic complications and their mechanisms, the diagnostic approach, and the principles of management. This self-assessment section tests your ability to integrate these concepts across clinical scenarios — the skill that defines the NMC KH-level competency for IM1.1–IM1.7. Read each scenario below carefully, identify the dominant haemodynamic and aetiological pattern, apply the classification and compensatory mechanism frameworks, and arrive at the diagnosis and management plan before reading the provided analysis. The image below serves as an integrative visual anchor for everything covered in this module. Read each scenario, generate your own answer, then review the analysis provided.
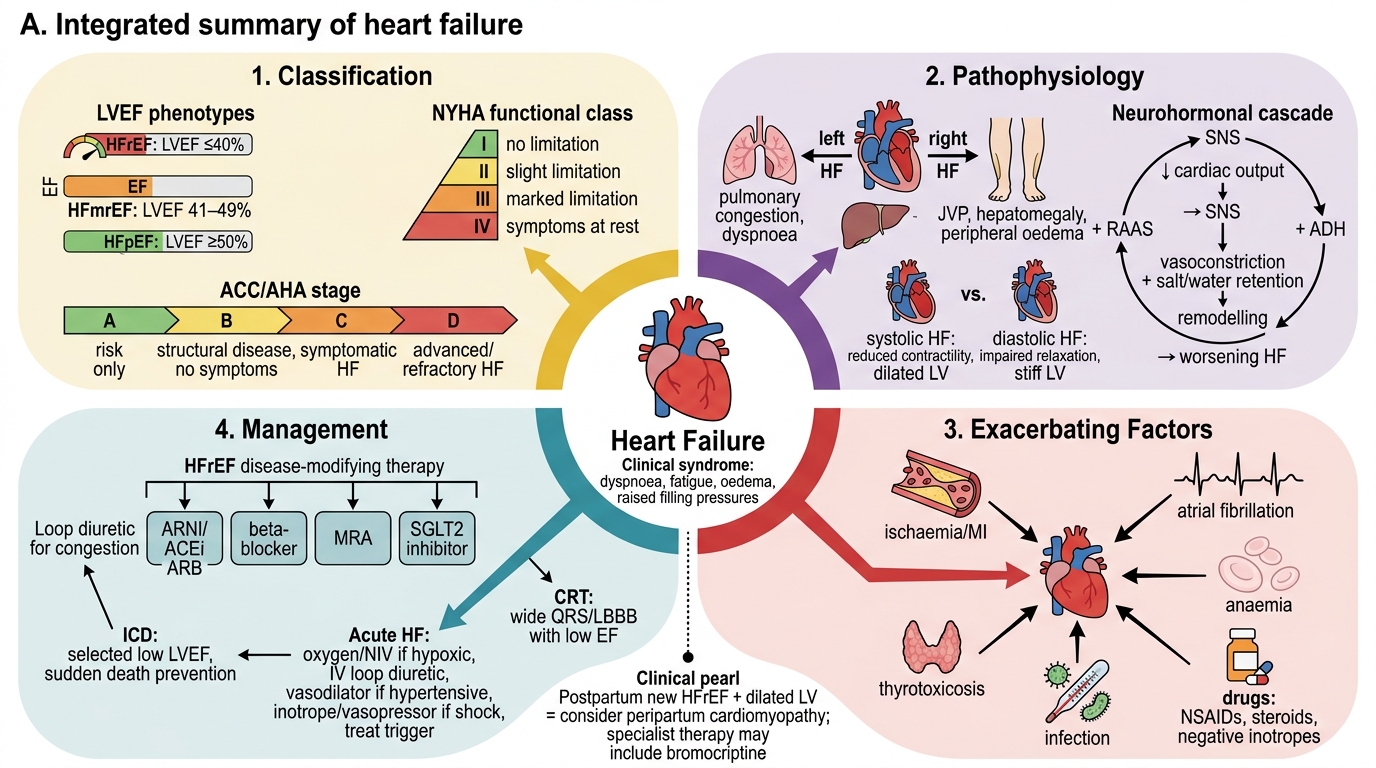
Heart Failure: Integrated Summary
Scenario A: A 45-year-old woman with no previous cardiac history presents with 3 months of progressive dyspnoea and two lower-limb oedema. She delivered a healthy baby 8 months ago. Her LVEF on echo is 30% with global hypokinesia and dilated LV (LV end-diastolic diameter 65 mm). BNP is elevated. What is the most likely diagnosis, and what aetiology-specific management consideration applies?
Analysis: New-onset HFrEF (LVEF 30%) presenting within 12 months of delivery (within 5 months postpartum in most definitions; here 8 months — still within the extended risk window), with global dilated cardiomyopathy pattern = peripartum cardiomyopathy (PPCM). PPCM is an important cause of dilated cardiomyopathy in women of childbearing age in India. Aetiology-specific point: bromocriptine (a dopamine agonist) is used in PPCM specifically — it blocks prolactin secretion, which is implicated in PPCM pathogenesis through a 16-kDa cleavage fragment causing endothelial dysfunction. Bromocriptine is not part of standard HF therapy; its use in PPCM reflects the aetiology-specific approach to management.
Scenario B: A 70-year-old man with CKD and known HFrEF (LVEF 28%) is admitted with acute decompensation. His JVP is elevated, bilateral basal crackles are present, and he is on furosemide 80 mg daily. His serum potassium is 3.1 mEq/L. An ECG shows prolonged QT interval (QTc 520 ms). He is prescribed additional furosemide and an antibiotic (clarithromycin) for a concurrent chest infection. What is the arrhythmic risk, and what monitoring is required?
Analysis: The patient has multiple risk factors for life-threatening arrhythmia: (1) hypokalaemia (K 3.1 mEq/L) — reduces resting membrane potential, promotes EADs; (2) prolonged QTc (520 ms at baseline — >500 ms is a high-risk threshold); (3) clarithromycin is a QT-prolonging antibiotic that further extends the QTc through hERG potassium channel blockade. Adding more furosemide will worsen hypokalaemia. This combination creates a high risk for torsades de pointes (polymorphic VT) progressing to VF. Required: (a) correct potassium to ≥4.0 mEq/L and magnesium to ≥1.0 mmol/L before/during furosemide increase; (b) change antibiotic to one without QT-prolonging risk (e.g. amoxicillin-clavulanate if appropriate); (c) continuous cardiac monitoring; (d) daily ECG.
Scenario C: A 55-year-old man with hypertensive heart disease has LVEF 65% and echo evidence of grade II diastolic dysfunction. He presents with exertional dyspnoea and has an elevated NT-proBNP. He asks why he has heart failure when 'his pump is working fine.' How do you explain HFpEF to him?
Analysis: Explain that the heart has two phases of function: contraction (systole) and relaxation (diastole). In his case, the heart muscle squeezes normally (LVEF 65%), but the problem is in relaxation — years of high blood pressure have made the heart walls thick and stiff. A stiff heart cannot relax and fill properly between beats, so it needs higher pressure to fill the same volume. This elevated filling pressure backs up into the lungs, causing breathlessness on exertion — the same symptom as 'pump failure' but through a different mechanism. Treatment focuses on controlling blood pressure, losing weight, and managing diabetes/AF — the factors that caused the stiffness.